Epididymitis: The Swollen Testicle That Isn’t Cancer
A sudden, painful, swollen testicle is terrifying, and reading online forums only makes the panic worse. In my experience, the diagnosis is rarely cancer; it is usually epididymitis. However, brushing it off as an infection can cost you a testicle if you actually have torsion. This guide breaks down exactly what is happening and the red flags you cannot ignore.

Epididymitis is the single most common reason a man under 50 ends up in my clinic convinced he has testicular cancer. The swelling appears, the pain builds over a day or two, he Googles “swollen testicle,” sees the word “tumor,” and arrives terrified. In the vast majority of cases, what he actually has is an infection of the epididymis — the coiled tube behind the testicle that stores and transports sperm. It is treatable. It is not cancer. But it is not nothing, either: it can mimic testicular torsion (a surgical emergency), and a small number of cases hide a more serious diagnosis underneath. This guide walks through what epididymitis actually is, how I tell it apart from the conditions it mimics, which antibiotics work, and the red flags that mean you stop reading and go to the emergency room now.
Key Takeaways
- Epididymitis is inflammation of the epididymis — the curved tube behind the testicle — and accounts for around 600,000 US clinic visits each year.
- In men under 35, the cause is almost always a sexually transmitted infection (chlamydia or gonorrhea). In men over 35, it is usually an enteric bacterium (E. coli) tracking down from the bladder or prostate.
- The most dangerous mimic is testicular torsion. If pain came on suddenly within 1-2 hours, your testicle looks higher or twisted, or you are vomiting with the pain, go to the emergency room now.
- Treatment is targeted antibiotics for 10-14 days based on the likely organism. Symptoms usually start improving within 72 hours; full resolution of swelling can take 2-4 weeks.
- Swelling that does not resolve after a full antibiotic course needs an ultrasound and urology review to rule out abscess, tuberculosis, or — rarely — testicular cancer hiding underneath the inflammation.
What Epididymitis Actually Is
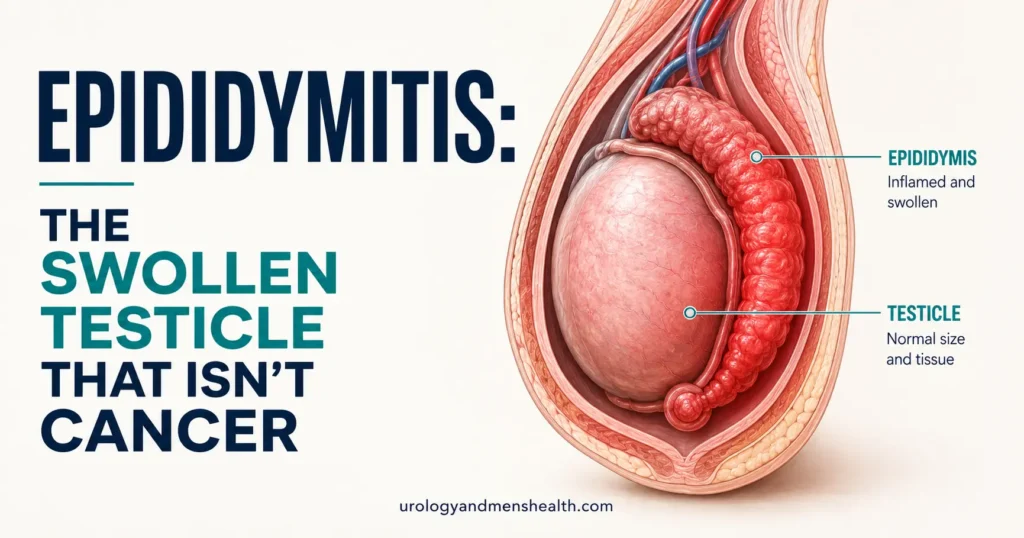
The epididymis is a tightly coiled tube — around 6 meters (20 feet) of tubing folded down to a structure about 5 cm long — that sits along the back of each testicle. Sperm produced inside the testicle pass into the head of the epididymis (the caput), mature as they travel through the body (corpus), and are stored at the tail (cauda) until ejaculation. Epididymitis is inflammation of this tube, almost always caused by bacterial infection. When the inflammation spreads to involve the testicle itself, the condition is called epididymo-orchitis.[1]
What you feel as a “swollen testicle” is rarely the testicle itself. It is the epididymis swelling against the back of the testicle, which makes the entire scrotum tender, hot, and often visibly red. The testicle proper usually feels normal in size and consistency once the swelling settles. The distinction matters: men who feel a lump and assume it is a tumor are usually feeling an inflamed epididymis, which is the curved structure behind the testicle, not the smooth oval of the testicle itself.
Epididymitis affects roughly 600,000 men in the United States each year, with the highest incidence between ages 14 and 35.[2] It is the most common cause of scrotal pain in men presenting to the emergency room outside the pediatric age group. Despite how common it is, it is consistently misdiagnosed in both directions: missed when it is actually torsion, and over-diagnosed when it is actually something else — including, rarely, testicular cancer.
Why Age Determines the Cause
This is the single most important clinical point in epididymitis and the one most often skipped in patient information online: the bacteria that cause epididymitis differ dramatically based on age. The empiric antibiotic choice depends almost entirely on which age bracket you fall into, because choosing the wrong drug means 10-14 days of unnecessary side effects and a recurrence.
Men under 35: sexually transmitted causes
In men under 35 who are sexually active, the cause is almost always Chlamydia trachomatis or Neisseria gonorrhoeae — the same organisms responsible for most cases of urethritis.[3] The infection starts in the urethra, often with no symptoms (asymptomatic urethritis is the rule, not the exception), and tracks backward up the vas deferens to reach the epididymis. This is why I always ask about sexual history even when the patient insists “it can’t be that” — the original infection may have been silent for weeks.
Men over 35: enteric and prostate-related causes
In men over 35, the cause shifts to Escherichia coli and other enteric bacteria — the same organisms that cause urinary tract infections. The pathway is also different: the bacteria usually originate in the prostate or bladder and track downward. This is why epididymitis in an older man frequently signals an underlying problem with bladder emptying — most often benign prostatic hyperplasia (BPH) creating residual urine that becomes a bacterial reservoir. Treating only the antibiotic course and ignoring the underlying obstruction guarantees recurrence within months.
Special populations
Two groups have different patterns worth flagging. Men who have insertive anal sex can develop epididymitis from enteric organisms (E. coli) even when under 35, so age alone doesn’t dictate antibiotic choice — sexual history does.[3] Men with indwelling catheters or recent urological procedures (cystoscopy, prostate biopsy, TURP) are at risk of catheter-associated epididymitis from a wider range of pathogens, including Pseudomonas and resistant organisms. These cases often need a urine culture before starting antibiotics rather than empiric treatment.
In My Practice
A 29-year-old came to clinic last year embarrassed and certain he had cancer. He had a tender, swollen left testicle that had been building over three days, and he had stopped sleeping because of the worry. On examination the epididymis was clearly thickened and tender along its full length, the testicle itself felt normal, and lifting the testicle eased his pain. He flatly denied any new sexual partners or unprotected sex when I asked the first time. When I explained that under-35 epididymitis is overwhelmingly caused by chlamydia or gonorrhea — usually picked up from a partner who never had symptoms — and that the test was a simple urine sample, he agreed. The chlamydia PCR came back positive. He had been with the same partner for two years.
This is the conversation I have constantly: epididymitis in a young man is a chlamydia infection until proven otherwise, and the awkward question has to be asked even when the patient seems certain it can’t apply.
Symptoms: What Epididymitis Actually Feels Like
The symptom pattern is reasonably consistent and helps distinguish epididymitis from its mimics:
- Gradual onset over hours to days, not minutes. Most men describe waking up with a vague ache that becomes a clear pain over 12-48 hours.
- Pain localized to the back of one testicle, often radiating up into the groin or lower abdomen along the spermatic cord.
- Visible swelling and redness of one side of the scrotum within 24-48 hours. The affected side is usually warm to touch.
- Pain that eases when the testicle is lifted — known as a positive Prehn’s sign. This is suggestive but not diagnostic; do not rely on it alone to rule out torsion.
- Burning on urination, urethral discharge, or increased urinary frequency in around 30-50% of cases (more common in younger men with STI-related disease).
- Low-grade fever and feeling generally unwell. Higher fevers (above 39°C / 102°F) suggest abscess formation or bacteremia and need urgent assessment.
What you should not have: sudden severe pain that arrives in minutes, a testicle that looks visibly higher than the other or sits at an abnormal angle, repeated vomiting, or a hard stone-like swelling that does not soften. Any of those changes the diagnosis entirely. The next section covers exactly why.
The Three Conditions Epididymitis Gets Confused With
1. Testicular torsion (the dangerous mimic)
Testicular torsion is the twisting of the spermatic cord, which cuts off blood supply to the testicle. It is a true surgical emergency: contemporary data show testicular salvage rates above 90% when surgery happens within 6 hours of pain onset, falling to under 50% by 12 hours and below 10% by 24 hours.[4] A torsed testicle that cannot be saved must be removed.
The classic distinguishing features: sudden onset within minutes (often during sleep or sport), pain that worsens rather than eases when the testicle is lifted, an absent cremasteric reflex (the testicle does not retract when the inner thigh is stroked), and frequent associated nausea and vomiting. The affected testicle often sits higher and at an abnormal horizontal angle. However — and this is the critical point — no single feature reliably distinguishes torsion from epididymitis on examination alone.[5] Around 1 in 5 cases of torsion are initially misdiagnosed as epididymitis at first presentation, and that delay is what costs men their testicle. Doppler ultrasound is the diagnostic test that settles it.
The rule I give patients: any sudden severe scrotal pain in a man under 30, especially when it wakes him from sleep, is torsion until ultrasound proves otherwise. Read the full guide on this here: Testicular Torsion: The 6-Hour Emergency.
2. Testicular cancer (the feared mimic)
This is the diagnosis every man Googling “swollen testicle” is terrified of, and the reason most patients delay coming to clinic at all. The reassuring news: testicular cancer presents very differently from epididymitis. A testicular tumor is usually painless, hard, and felt within the testicle itself — not the soft, tender, posterior swelling of an inflamed epididymis. Tumors typically grow slowly over weeks to months, do not cause fever, do not improve with antibiotics, and are not accompanied by urinary symptoms.
The danger is that an inflamed epididymis can hide a tumor underneath. This is why any swelling that does not resolve completely after a full antibiotic course needs an ultrasound, no exceptions. The fact that the swelling responded somewhat to antibiotics does not rule out cancer; it just delays the diagnosis. Anyone with a residual lump at 4-6 weeks post-treatment gets imaged. The full guide to recognizing testicular cancer is here: Testicular Lumps and Cancer: Self-Exam and Diagnosis.
3. Penile and scrotal skin conditions
Less commonly, men present convinced they have epididymitis when the actual problem is scrotal cellulitis (a skin infection), a hydrocele (painless fluid collection around the testicle), or an inflamed sebaceous cyst on the scrotal skin. These are usually clinically obvious to a urologist but can be mistaken at first glance. The broader review of scrotal and penile health concerns covers when each pattern matters.
Stuck in a cycle of recurrent UTIs? Download Dr. Khalid’s Recurrent UTI Eradication Protocol.
Enter your email below to receive Dr. Khalid’s complete Recurrent UTI Eradication Protocol as a free, printable PDF.
How Epididymitis Is Actually Diagnosed
A competent urological assessment for suspected epididymitis includes three things, in this order:
- A focused history: timing and pattern of onset, sexual history (always asked, regardless of relationship status), urinary symptoms, prior urological procedures, and any history of urinary tract obstruction.
- A physical examination: location and quality of tenderness, presence of urethral discharge, cremasteric reflex, lie of the testicle, and Prehn’s sign. None of these on their own are diagnostic.
- Doppler ultrasound of the scrotum: this is the test that confirms the diagnosis and excludes torsion. Epididymitis shows increased blood flow in the epididymis; torsion shows reduced or absent blood flow in the testicle.[1] Any emergency department evaluating scrotal pain should have access to this within an hour.
Additional tests depend on the suspected cause. In men under 35, a first-pass urine sample for chlamydia and gonorrhea PCR is standard.[3] In men over 35, a midstream urine culture identifies the responsible organism and guides antibiotic choice. Anyone with a high fever, very high white cell count, or signs of systemic infection needs blood cultures and consideration of admission for IV antibiotics.
If you are uncertain whether your symptoms point to a urinary tract infection, an STI, or epididymitis itself, the UTI Risk Assessment for Men can help you organize the picture before your appointment.
Treatment: The Antibiotics That Actually Work
Empiric antibiotic treatment is started immediately on clinical suspicion, before culture results return, because waiting risks abscess formation. The choice of antibiotic depends entirely on the likely organism, which depends on age and sexual history.
Likely sexually transmitted (most men under 35)
The 2021 CDC STI Treatment Guidelines recommend ceftriaxone 500 mg intramuscular single dose plus doxycycline 100 mg twice daily for 10 days.[3] The European IUSTI 2024 guideline updated the ceftriaxone dose to 1 g intramuscular to reflect rising gonococcal resistance, and removed the previous routine addition of azithromycin.[6] Both regimens cover chlamydia and gonorrhea reliably. Sexual partners from the previous 60 days must be tested and treated, regardless of whether they have symptoms.
Likely enteric organism (most men over 35)
The standard regimen is a fluoroquinolone — usually levofloxacin 500 mg once daily for 10 days, or ofloxacin 300 mg twice daily for 10 days.[3] Trimethoprim-sulfamethoxazole is an alternative where local resistance patterns favor it. In men with mixed risk factors (older but sexually active with new partners, or men who have insertive anal sex), combination therapy with ceftriaxone 500 mg IM single dose plus levofloxacin 500 mg daily for 10 days covers both pathways.[3]
Supportive measures that genuinely help
- Scrotal elevation with a supportive jock strap or athletic supporter, day and night for the first week. This is the single most effective thing you can do to reduce pain.
- Cold compresses (an ice pack wrapped in a towel) applied for 15 minutes every few hours during the first 48 hours.
- NSAIDs — ibuprofen 400-600 mg every 8 hours with food, or naproxen 500 mg twice daily — for both pain and anti-inflammatory effect.
- Bed rest for the first 24-48 hours, then gradual return to light activity. Avoid strenuous exercise or heavy lifting for 2-3 weeks.
- Sexual rest until you and any partner have completed treatment, to prevent reinfection.
Most men notice meaningful improvement in pain within 48-72 hours of starting the correct antibiotic. If you are not feeling significantly better at 72 hours, the diagnosis or the antibiotic choice is wrong — you need to be reassessed. Full resolution of the swelling typically takes 2-4 weeks, and some men have low-grade tenderness for up to 8 weeks afterwards, which is normal.
When Epididymitis Becomes Chronic
Around 15-20% of men with acute epididymitis go on to develop chronic epididymitis — defined as pain and discomfort in the epididymis lasting more than 3 months.[7] This is a frustrating condition for both patients and urologists because the inflammation is no longer driven by active infection, and antibiotics rarely help once it has set in.
Chronic epididymitis often overlaps with chronic prostatitis and pelvic pain syndromes, and management is similar: a combination of NSAIDs, pelvic floor physiotherapy, neuropathic pain medications (amitriptyline, pregabalin) where the pain has a burning or shooting quality, and stress management. A small number of men with intractable chronic pain ultimately need surgical epididymectomy, but this is a last resort and the pain does not always resolve even after surgery.
Red Flags: When to Stop Reading and Go to the ER
Emergency Department Now — Not Later
Any of the following means you stop self-managing and go to the nearest emergency room immediately. Do not wait for a primary care appointment, do not wait until morning, do not try ice and ibuprofen first:
- Sudden severe scrotal pain that arrived in minutes rather than building over hours
- The affected testicle looks higher than the other, or sits at a horizontal or twisted angle
- Repeated vomiting accompanying the pain
- Fever above 39°C (102°F), especially with shaking chills (rigors)
- A hard, stone-like swelling that does not soften, or a separate painless lump within the testicle itself
- Pain that is not improving after 72 hours of correct antibiotic treatment
- You are under 30 with sudden pain — assume torsion until ultrasound proves otherwise
The 6-hour window for testicular torsion is real. Salvage rates above 90% within 6 hours collapse to below 10% by 24 hours.[4] A man who waits until morning to “see if it gets better” frequently arrives in clinic the next day with a testicle that cannot be saved. The cost of an unnecessary ER visit for what turns out to be epididymitis is a few hours and a co-pay. The cost of staying home with missed torsion is permanent.
Prevention and What to Do After Recovery
Most cases of epididymitis are preventable. The specific measures depend on the cause:
- For STI-related disease: consistent condom use, testing every 3-12 months depending on number of partners, and ensuring that any positive partner notification is acted on quickly. The infection that gave you epididymitis was almost certainly silent in the partner who passed it.
- For enteric/UTI-related disease in older men: address the underlying obstruction. If you have BPH symptoms (weak stream, hesitancy, incomplete emptying, nocturia), get the prostate properly assessed. Treating the BPH usually prevents recurrence; ignoring it usually means another episode within 12 months.
- After any urological instrumentation (cystoscopy, prostate biopsy, TURP, catheterization): make sure prophylactic antibiotics were appropriately given. Speak up if you develop scrotal pain in the days afterwards — post-procedural epididymitis is a recognized complication and needs prompt treatment.
- For all men: resume gentle monthly testicular self-examination once the swelling has fully resolved. This is the only way to spot a new lump early, particularly if you are in the age range (15-44) where testicular cancer is most common.
If you are at all unsure when to seek urological review beyond simple recovery, the broader guide on when a young man should see a urologist covers the full set of warning signs across all conditions.
Frequently Asked Questions
How long does epididymitis take to fully heal?
Pain usually starts improving within 48-72 hours of starting the correct antibiotic. Visible swelling typically takes 2-4 weeks to resolve completely, and some men have low-grade tenderness for up to 8 weeks afterwards — this is normal. If any swelling persists at 6 weeks, you need a follow-up ultrasound to rule out abscess or, rarely, an underlying testicular cancer that was masked by the inflammation. Read the testicular cancer self-exam guide for what to look for during recovery.
Can epididymitis cause infertility?
A single uncomplicated episode of epididymitis treated promptly with the right antibiotic almost never causes infertility. Repeated or untreated episodes can scar the epididymis and obstruct sperm passage, which is one reason why finishing the full antibiotic course matters even after symptoms improve. Men with persistent fertility concerns after epididymitis should have a semen analysis 3-6 months post-recovery to confirm normal sperm function.
How do I tell epididymitis from testicular torsion at home?
You cannot reliably tell them apart at home, and this is the most important point in the entire condition. Sudden onset within minutes, pain that worsens when the testicle is lifted, vomiting, and an absent cremasteric reflex all suggest torsion — but no single feature rules torsion out, and around 1 in 5 cases of torsion are initially misdiagnosed as epididymitis at first presentation. Any sudden severe scrotal pain in a man under 30 should be assumed to be torsion until a Doppler ultrasound proves otherwise. The full testicular torsion emergency guide walks through the 6-hour window in detail.
Do I need to tell my sexual partner I have epididymitis?
If you are under 35 or if testing has identified chlamydia or gonorrhea as the cause, yes — current and recent (within the previous 60 days) sexual partners need to be tested and treated, regardless of whether they have symptoms. The infection that gave you epididymitis was almost certainly silent in the partner who passed it, which means they need treatment even if they feel fine. Most US states have anonymous partner notification services through public health departments if the conversation is difficult.
Why does epididymitis keep coming back?
Recurrent epididymitis in men over 35 almost always signals an underlying problem with bladder emptying — most commonly an enlarged prostate (BPH) creating residual urine that becomes a bacterial reservoir. In younger men, recurrence usually means reinfection from an untreated partner or a missed concurrent STI. Either way, a recurrent case needs a urology referral for proper investigation rather than just another antibiotic course — repeating the same treatment without finding the cause guarantees another episode within months.
Can I have sex while being treated for epididymitis?
You should avoid sex until both you and any sexual partner have completed treatment and any symptoms have resolved — typically a full 7-10 days after starting antibiotics. Having sex during treatment risks reinfecting your partner (or being reinfected by them if they were the original source) and may worsen the inflammation. After full recovery there are no long-term restrictions on sexual activity, although using condoms reduces the risk of a future STI-related recurrence.
References
- Bonkat G, Bartoletti R, Bruyère F, et al. European Association of Urology Guidelines on Urological Infections: Summary of the 2024 Guidelines. European Urology. 2024;86(1):27-41. EAU Guidelines
- McConaghy JR, Panchal B. Epididymitis: An Overview. American Family Physician. 2016;94(9):723-726. PubMed
- Centers for Disease Control and Prevention. Sexually Transmitted Infections Treatment Guidelines, 2021: Epididymitis. CDC. 2021. CDC
- Sharp VJ, Kieran K, Arlen AM. Testicular Torsion: Diagnosis, Evaluation, and Management. American Family Physician. 2013;88(12):835-840. AAFP
- Schmitz D, Safranek S. How useful is a physical exam in diagnosing testicular torsion? Journal of Family Practice. 2009;58(8):433-434. PubMed
- Street EJ, Justice ED, Kopa Z, et al. The 2024 European guideline on the management of epididymo-orchitis. International Journal of STD & AIDS. 2024. IUSTI Guideline
- Nickel JC, Siemens DR, Nickel KR, Downey J. The patient with chronic epididymitis: characterization of an enigmatic syndrome. Journal of Urology. 2002;167(4):1701-1704. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.