Urinary Catheter Care at Home: A Urologist’s Guide
Most catheter problems I see at home are not bad luck — they trace back to two or three small daily habits. Get those right and you avoid the blockages, leaks, and infections that send people back to the ER.

Good urinary catheter care at home is mostly about a handful of small habits done consistently, not about doing anything complicated. I see this in clinic constantly: the person who ends up back in the emergency room with a blocked or infected catheter is almost never the one who did something dramatically wrong. It’s the one who let the drainage bag sit above bladder level overnight, or skipped the morning clean a few too many times, or stopped drinking enough because getting up was a hassle. A catheter is a tube that gives bacteria a direct road into your bladder, so the daily routine exists to keep that road as clean and as freely draining as possible. This guide walks through exactly what to do each day, how to spot trouble early, and which symptoms mean you stop managing at home and get help. For how this fits the bigger picture of urinary infections, see our UTIs & Infections Hub.
Key Takeaways
- Keep the drainage bag below bladder level at all times — urine that sits in the tube or flows backward is the single most common reason catheters get infected.
- Clean the area where the catheter exits your body once daily with plain soap and water; antiseptic washes do not lower infection rates and can irritate the skin.
- Aim for roughly 2 liters of fluid a day (about 68 fl oz / 8.5 cups) unless your doctor has restricted fluids — dilute urine blocks the catheter far less often.
- Urine that looks cloudy is not by itself a reason for antibiotics; a fever, rigors (violent shivering), flank pain, or the catheter not draining are the signs that need urgent care.
How an indwelling catheter actually sits inside you
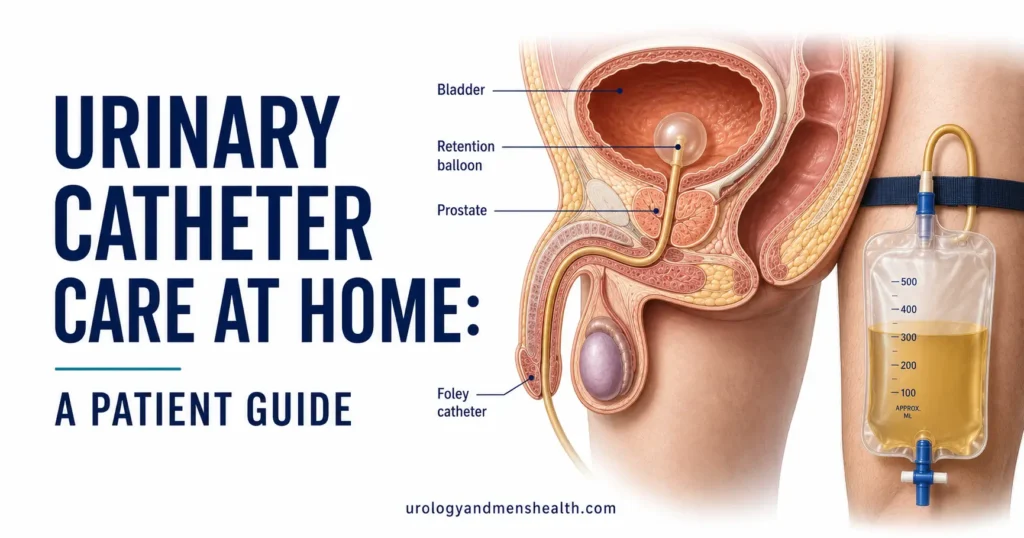
An indwelling catheter — the type most people go home with, often called a Foley — is a soft tube that runs up the urethra into the bladder. Near its tip is a small balloon that gets inflated with sterile water once the tube is in place. That balloon is what holds the catheter inside; it sits at the bladder neck like an anchor so the tube cannot slide out. This is why you must never pull on the catheter — the inflated balloon will not pass back through the urethra and pulling causes real injury.
Urine drains out of the bladder through small holes near the tip, down the tube, and into a bag. Because the system is closed, your bladder no longer fills and empties on its own — it drains continuously. That continuous open channel is also the catheter’s main downside: it bypasses the natural defenses that normally keep bacteria out of the bladder. Within a few days a thin film of bacteria, called a biofilm, coats the inside of any catheter. This is normal and is not the same as an infection. The goal of home care is to stop that background colonization from tipping over into a true catheter-associated urinary tract infection (a bladder or kidney infection caused by the catheter, often shortened to CAUTI).
Many people end up with a catheter after an episode of being unable to pass urine at all. If that is your situation, it is worth understanding why it happened — our guide to acute urinary retention and what triggers it explains the common causes and what the plan usually is to get the catheter out again.
Your daily catheter care routine
The routine below is what I give patients on the day they go home. None of it takes more than a few minutes, and the consistency matters more than the technique being perfect.
Wash your hands before and after — every time
Soap and water for 20 seconds, or an alcohol gel, before you touch any part of the catheter or bag and again afterward. Your hands are how bacteria reach the system. This one step does more to prevent infection than anything else on this list.
Clean where the catheter exits, once a day
Using plain soap and warm water, gently clean the skin and the first inch of tubing where it exits the body, always wiping away from the body, not toward it. Do this once daily and after every bowel movement. The evidence here is clear and a little counterintuitive: plain soap and water works as well as antiseptic solutions, and the antiseptics can dry and irritate the skin, so skip them unless specifically told otherwise. If you are uncircumcised, gently retract the foreskin to clean and then return it to its normal position.
Keep the bag below your bladder, always
Urine should always flow downhill, away from you. If the bag rises above the level of your bladder — resting it on your lap, hanging it on a bed rail that is too high, lying with it beside you — urine that has already drained can flow back toward the bladder, carrying bacteria with it. When you are up and about, a leg bag strapped to the thigh or calf works well. At night, connect a larger bag and hang it on a stand or frame beside the bed, lower than the mattress. Never let the bag touch the floor.
Empty the bag before it is full
Empty when the bag is about two-thirds full, and at least every 8 hours, through the tap at the bottom. A bag stretched completely full pulls on the system and lets urine pool. Don’t let the drainage tap touch the toilet, a container, or the floor, as that contaminates it. Most leg bags last about a week before they are changed; your nurse will tell you your specific schedule.
Drink enough to keep urine pale
Unless your doctor has restricted your fluids for a heart or kidney reason, aim for around 2 liters a day (about 68 fl oz / 8.5 cups). A well-flushed system blocks far less often, because concentrated urine lets sediment and mineral debris build up and clog the tube. Pale yellow urine is the target. If you want to understand what your output volume signals about bladder emptying more broadly, our explainer on what residual urine measurements mean is a useful companion.
In My Practice
One of the most common calls I get from a patient three or four days after discharge is “the catheter has stopped draining and I’m in pain.” Nine times out of ten, when I ask, the bag has been sitting up on the sofa next to them or the tube has a kink hidden under a blanket. We fix it on the phone by getting the bag below the bladder and straightening the line, and the urine starts flowing within a minute.
If repositioning and unkinking the tube does not restore drainage within a few minutes, treat it as a blockage that needs urgent attention rather than something to wait out overnight.
Living with a catheter and worried about a repeat infection?
Enter your email below to receive Dr. Khalid’s complete Recurrent UTI Eradication Protocol as a free, printable PDF.
Catheter problems and the red flags that need help
A few problems are common and manageable; a smaller set are genuine emergencies. Knowing which is which keeps you out of the ER for things you can handle and gets you there fast for things you cannot.
Leaking around the catheter (bypassing) usually means the bladder is squeezing against the tube — often from constipation pressing on the bladder, from bladder spasms, or from a partial blockage. A small amount is common and not dangerous. First check the tube is not kinked or blocked and that your bowels are moving; persistent leaking should be reported to your nurse, who may check the catheter size or prescribe a medication to calm spasms.
Cloudy or stronger-smelling urine is extremely common with any catheter and, on its own, is not an infection and does not need antibiotics. Nearly everyone with a long-term catheter grows bacteria in their urine without being ill from it — treating that with antibiotics just breeds resistant bugs. What matters is whether you feel unwell with it. Our companion guide on avoiding catheter infections day to day goes deeper on why cloudy urine alone is not the alarm bell people assume it is.
A blocked catheter — no urine draining for a couple of hours, often with lower-belly pain or pressure — is urgent. Reposition the bag below the bladder and straighten the tube first. If nothing flows within a few minutes, the catheter needs flushing or changing and you should contact your nurse or out-of-hours service promptly, because a blocked catheter with a full bladder is painful and risks backing pressure up to the kidneys.
Go to the ER Now If
These signs point to a serious infection or dangerous obstruction and need same-day emergency assessment, not a wait-and-see:
- A fever, shaking chills, or violent shivering (rigors) — the clearest sign a catheter infection has reached your bloodstream or kidneys.
- The catheter stops draining and your lower belly is painful or swollen despite repositioning the bag and unkinking the tube.
- Bright-red blood, or blood clots, in the urine (a few pink-tinged days after insertion can be normal — fresh red blood or clots is not).
- Pain in your side or lower back with feeling unwell, suggesting the infection has moved up to a kidney.
- If you have a spinal cord injury at or above mid-back level: a sudden pounding headache, sweating, and a flushed face — this can signal autonomic dysreflexia from a blocked catheter and is a medical emergency.
Beyond spotting trouble, you can lower your baseline risk. Two free tools help: gauge your own profile with the UTI risk assessment for men, and if your catheter is temporary, talk with your team about the right product using the catheter size and type selector, since an oversized catheter is a frequent and avoidable cause of bypassing and irritation.
Frequently Asked Questions
What does good urinary catheter care at home actually involve each day?
Daily urinary catheter care at home comes down to four habits: wash your hands before and after touching the system, clean the catheter exit site once with plain soap and water, keep the drainage bag below bladder level at all times, and drink enough to keep your urine pale. Empty the bag when it is two-thirds full. These steps, done consistently, prevent most blockages and infections. Our infection-prevention guide covers the why behind each.
How do I clean a catheter, and should I use antiseptic?
Clean the skin and the first inch of tubing where the catheter exits your body once a day with plain soap and warm water, wiping away from the body. Antiseptic solutions are not recommended for routine care — studies show they do not lower infection rates compared with soap and water, and they can irritate the skin. If you are uncircumcised, gently clean under the retracted foreskin, then return it to position.
Is cloudy urine in my catheter a sign of infection I should worry about?
Usually not on its own. Cloudy, stronger-smelling urine is very common with any catheter and reflects normal bacterial colonization, not necessarily a catheter infection. Antibiotics are not needed for cloudy urine alone, and overusing them breeds resistance. The signs that do matter are a fever, rigors, flank pain, or feeling generally unwell — those mean you seek care. If unsure, the UTI risk assessment can help you frame the conversation.
Why is my catheter leaking urine around the tube?
Leaking around the catheter, called bypassing, usually means the bladder is contracting against the tube. The most common triggers are constipation pressing on the bladder, bladder spasms, or a partial blockage in the tube. Check first that the tube is not kinked and that your bowels are regular. If leaking persists, your nurse may review the catheter size or prescribe a medication to settle bladder spasms — don’t simply size up the catheter yourself.
What should I do if my catheter stops draining?
Act quickly. Lower the drainage bag below your bladder and straighten any kinks in the tube — this restores flow most of the time. If no urine drains within a few minutes and your lower belly feels full or painful, treat it as a blockage and contact your nurse or out-of-hours service the same day. A blocked catheter with a full bladder can push pressure back to the kidneys, and waiting overnight is not safe. Understanding how urinary retention behaves helps you judge the urgency.
References
- European Association of Urology. EAU Guidelines on Urological Infections: catheter-associated UTI. EAU Guidelines. 2024. EAU
- National Institute of Diabetes and Digestive and Kidney Diseases. Urinary Catheters. NIDDK. 2024. NIDDK
- Lam TBL, Omar MI, Fisher E, et al. Types of indwelling urethral catheters for short-term catheterisation in hospitalised adults. Cochrane Database Syst Rev. 2014;(9):CD004013. Cochrane
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.