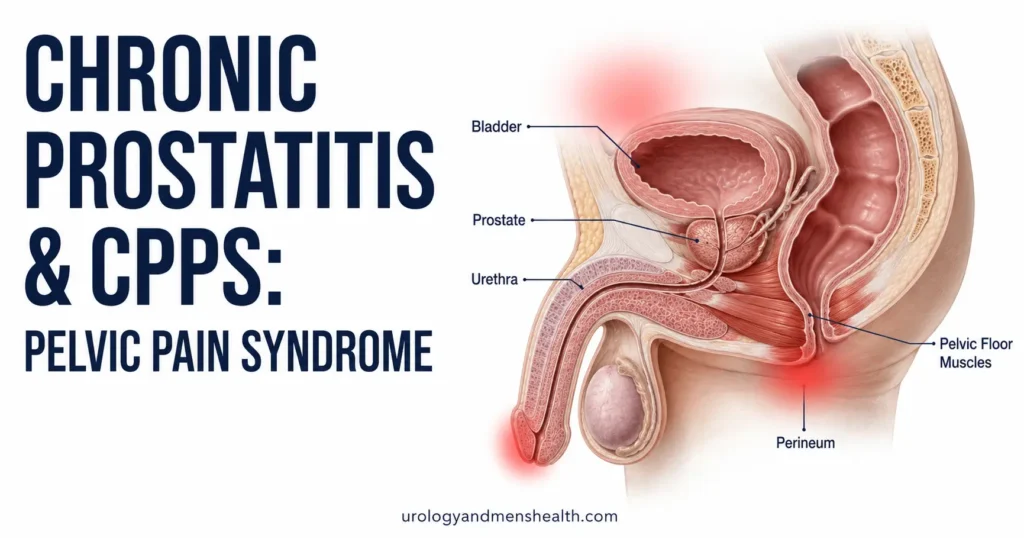
Chronic Prostatitis Treatment & CPPS: What Actually Works
Patients with a constant, dull pelvic ache usually spend months swallowing endless rounds of antibiotics for a "prostate infection" that never goes away. The truth is, if your urine cultures are clear, you don't have an infection—you have Chronic Pelvic Pain Syndrome. This guide explains why taking more Cipro won't help, and how we finally treat the real source of your pain using the proven UPOINT system.

If you have spent six months bouncing between primary care doctors and urologists, swallowed three courses of ciprofloxacin, had a normal urine culture every single time, and still feel that dull ache behind your scrotum or burning at the tip of your penis — you almost certainly do not have a prostate infection. You have chronic pelvic pain syndrome (CPPS), which the National Institutes of Health classifies as Category III prostatitis. It accounts for more than 90% of all prostatitis diagnoses, yet most men cycle through years of failed antibiotics before anyone uses the word. The fix is not stronger antibiotics. It is a phenotype-driven approach called UPOINT that targets the specific drivers of your pain, and effective chronic prostatitis treatment starts with identifying which of six domains is actually firing in your body.
Key Takeaways
- More than 90% of men told they have “prostatitis” actually have CPPS (NIH Category III) — a non-bacterial pain syndrome that does not respond to antibiotics.
- The NIH-CPSI questionnaire is the validated way to measure your symptoms; a score above 14 indicates moderate-to-severe disease worth aggressive treatment.
- UPOINT phenotyping splits CPPS into six domains (Urinary, Psychosocial, Organ-specific, Infection, Neurologic, Tenderness) — each gets a different treatment.
- Pelvic floor physical therapy outperforms antibiotics, alpha-blockers, and anti-inflammatories in head-to-head trials for CPPS men with muscular tenderness.
- Most men improve within 12 weeks of phenotype-matched therapy. The men who do not improve are usually the ones still being treated as if they have an infection.
What CPPS Actually Is (And Why Antibiotics Have Been Failing You)
The word “prostatitis” hides four very different conditions. The National Institutes of Health divides them into four categories [1]. Category I is acute bacterial prostatitis — fever, rigors, severely tender prostate on examination, positive urine culture. Category II is chronic bacterial prostatitis — recurrent urinary tract infections with the same organism, prostate confirmed as the reservoir on localization cultures. Both of these respond to antibiotics. Together they make up fewer than 10% of “prostatitis” diagnoses.
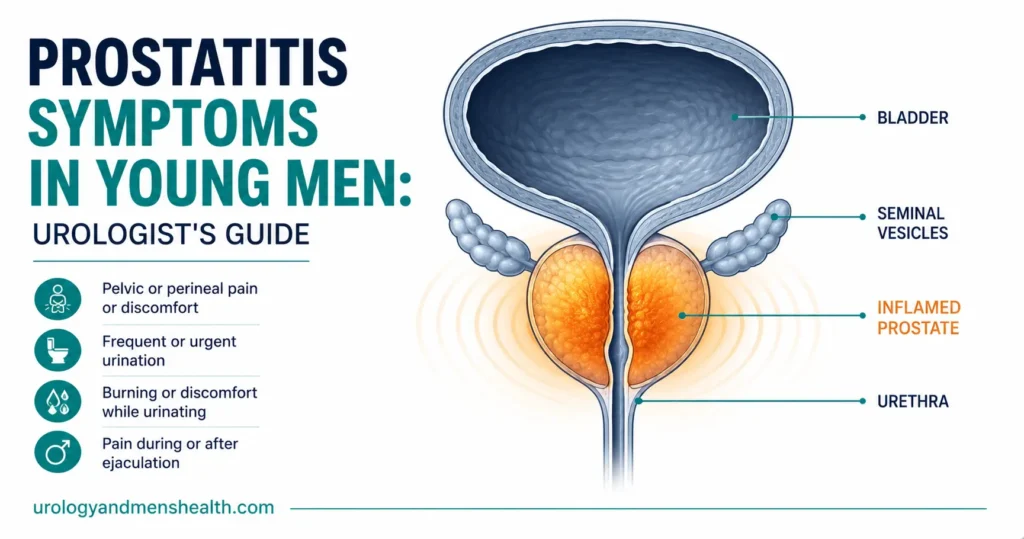
Category III is chronic pelvic pain syndrome (CPPS). No bacteria. No infection. Pain in the perineum, suprapubic area, scrotum, penis, or lower back lasting at least three of the last six months. This is more than 90% of cases. Category IV is asymptomatic inflammatory prostatitis — incidentally found on biopsy or semen analysis in a man with no symptoms, and requires no treatment at all.
Here is why this matters: if your urine culture is repeatedly negative and your symptoms have lasted more than three months, the probability you have a bacterial infection is below 5%. Continuing to take ciprofloxacin or doxycycline at that point is not treatment. It is just causing antibiotic resistance, tendinopathy risk, and gut microbiome damage. The 2022 EAU guideline on chronic pelvic pain explicitly recommends against repeated empirical antibiotic courses for CPPS [2].
The condition is common. Population studies estimate that 8-12% of men experience CPPS symptoms at some point in their lives, with peak prevalence between ages 30 and 50 [3]. It causes more lost workdays and lower quality of life scores than coronary artery disease, Crohn’s disease, or angina in the men who have it.
In My Practice
The pattern I see almost every week: a man in his early thirties walks in with a folder. Inside: three urine cultures (all negative), two semen analyses (one with white cells, one without), and prescriptions for ciprofloxacin, doxycycline, and azithromycin from three different doctors. He has been told he has a “deep-seated infection.” He has not. The white cells in semen are not a urinary tract infection — they are markers of prostatic inflammation, which in CPPS can come from pelvic floor spasm, autoimmune drivers, or simply the inflammatory cascade of chronic pain itself.
The moment I tell a man “this is not an infection, and no amount of antibiotics will fix it,” I usually see two reactions in sequence: relief that someone finally believes him, followed by frustration at the months he spent on the wrong treatment. The relief is the more important one — it is the first step in actually getting better.
How CPPS Actually Feels — The Symptom Pattern
CPPS pain is not a single symptom. It is a constellation of overlapping complaints that vary day to day, often triggered by stress, prolonged sitting, ejaculation, or constipation. The most common patterns I see in clinic:
- Perineal ache — a deep, dull pressure between the scrotum and anus, often described as “sitting on a golf ball”
- Suprapubic discomfort — pressure or aching above the pubic bone that mimics a UTI but with negative cultures
- Penile tip pain or burning — particularly at the meatus, often worse after ejaculation
- Testicular ache — usually one-sided, dull, with no swelling or tenderness on examination
- Urinary symptoms — frequency, urgency, hesitancy, slow stream, or sensation of incomplete emptying
- Pain with ejaculation — during, immediately after, or hours later (post-orgasmic pain)
- Lower back or inner thigh referral — from pelvic floor muscle trigger points
One critical pattern: men with CPPS often describe their pain as worse after sitting for long periods (commuting, desk jobs, long flights) and partially relieved by walking or warm baths. This is a major clue that the driver is muscular, not infectious — bacteria do not care whether you sit or stand.
Sexual dysfunction shows up alongside CPPS in roughly 40-50% of cases. Erectile difficulties, reduced libido, and premature ejaculation are common, partly from the chronic pain itself, partly from the anticipatory anxiety around ejaculation pain. If you are dealing with PE alongside your pelvic pain, the causes and treatment of premature ejaculation overlap meaningfully with CPPS management.
How CPPS Is Diagnosed — Scoring Your Symptoms First
Diagnosis of CPPS is one of exclusion. There is no scan, no blood test, no urine test that confirms it. What we do is rule out conditions that look like CPPS but require different treatment, then quantify your symptom severity to guide therapy.
The first step in any reasonable workup is the NIH Chronic Prostatitis Symptom Index (NIH-CPSI). This is a validated 13-question instrument scoring pain, urinary symptoms, and quality of life impact [4]. Total scores range from 0 to 43. A score of 0-14 is mild, 15-29 is moderate, and 30-43 is severe. We use the score both to confirm the diagnosis is serious enough to warrant active treatment and to track response over time. If your score does not drop by at least 6 points after 12 weeks of treatment, the phenotype was probably misread and the plan needs revision.
→ Score your CPPS severity with our NIH-CPSI CalculatorAfter scoring, the rest of the workup looks like this. A midstream urine culture rules out bacterial cystitis. A two-glass or four-glass localization test (pre-massage and post-massage urine samples) helps distinguish CPPS from chronic bacterial prostatitis. A digital rectal examination assesses prostate tenderness and pelvic floor muscle tone — this is the step most often skipped, and the most informative. A urethral swab for chlamydia and gonorrhea is appropriate in sexually active men. A flow study and post-void residual measurement screen for bladder outlet obstruction. Transrectal or pelvic MRI is reserved for atypical cases or treatment failures.
I do not routinely order PSA in young men with CPPS — prostate inflammation falsely elevates PSA and creates anxiety about cancer that the data does not justify in this age group. If PSA must be checked (men over 50, family history), interpret it knowing inflammation can push it 1-2 ng/mL above baseline.
The UPOINT Framework — Why One-Size-Fits-All Has Failed
For most of the last thirty years, CPPS treatment was a roulette wheel: try antibiotics, then alpha-blockers, then anti-inflammatories, then antidepressants, and hope something worked. The response rate was dismal — around 30% for any single therapy. In 2009, Dr. Daniel Shoskes at the Cleveland Clinic proposed the UPOINT system, and it changed practice [5]. UPOINT phenotypes each man into one or more of six clinical domains, and you treat the domains he actually has.
- U — Urinary: frequency, urgency, slow stream, post-void residual > 100 mL. Treatment: alpha-blockers (tamsulosin, alfuzosin, silodosin), bladder training, antimuscarinics if urgency dominates.
- P — Psychosocial: depression, anxiety, catastrophizing, perceived stress. Treatment: cognitive behavioral therapy (CBT), SSRIs or SNRIs (duloxetine has the best pain-modulating evidence), stress reduction.
- O — Organ-specific: tender prostate on examination, hematospermia, calcifications on imaging, prostatic-origin pain. Treatment: anti-inflammatories (NSAIDs short-course), quercetin 500 mg twice daily, 5-alpha reductase inhibitors in older men with prostatic enlargement.
- I — Infection: positive cultures, atypical organisms on extended culture, recent partner with STI. Treatment: targeted antibiotic course (this is the only domain where antibiotics are appropriate).
- N — Neurologic/Systemic: pain outside the pelvis (irritable bowel, fibromyalgia, chronic fatigue), central sensitization. Treatment: pregabalin, gabapentin, low-dose amitriptyline, duloxetine.
- T — Tenderness of pelvic floor muscles: palpable trigger points in levator ani, puborectalis, obturator internus. Treatment: pelvic floor physical therapy with trigger-point release, internal myofascial work, paradoxical relaxation training.
Most men have two or three domains firing simultaneously. The strongest single predictor of treatment response in modern series is correctly identifying which domains apply and treating all of them in parallel [6]. Treating only one domain when three are active is why so many men cycle through medications without improvement.
Months of pelvic pain and no real answers? Download Dr. Khalid’s Chronic Prostatitis / CPPS Guide.
Enter your email below to receive Dr. Khalid’s complete Chronic Prostatitis / CPPS Guide as a free, printable PDF.
Pelvic Floor Physical Therapy — The Underused First-Line Treatment
If I could change one thing about how CPPS is managed in the United States, it would be this: pelvic floor physical therapy should be offered to every man with CPPS at the first visit, not as a last resort after every drug has failed. The data has been clear for over a decade.
A randomized trial by Anderson and colleagues at Stanford showed that 72% of CPPS men with palpable pelvic floor trigger points achieved at least moderate improvement with paradoxical relaxation training plus internal trigger-point release, compared with around 30% for standard medical therapy [7]. The men in the physical therapy arm averaged a 12-point drop in NIH-CPSI scores. That is a clinically transformative result — the kind of change patients describe as “getting their life back.”
What does pelvic floor PT actually look like? A specialized pelvic floor physical therapist (this is not generic physiotherapy — the practitioner needs men’s pelvic health training) performs an internal digital examination of the pelvic floor muscles, identifies trigger points, and uses sustained pressure release techniques to deactivate them. You will be taught reverse Kegels (relaxation, not contraction — most CPPS men have hypertonic pelvic floors and Kegels make them worse), diaphragmatic breathing, and posture corrections. Sessions are typically weekly for 8-12 weeks, with substantial home practice in between.
The barrier is access. There are fewer than 1,500 certified men’s pelvic floor physical therapists in the United States, concentrated in major metropolitan areas. If you cannot access one in person, telehealth pelvic floor PT exists and has reasonable evidence for the home-exercise components. Ask your urologist for a specific referral by name — generic physiotherapy practices often lack the specialized training and will give you the same hip and core exercises that have not helped you.
Medications That Help — And the Ones That Do Not
Medication choice should follow UPOINT phenotype, not a default protocol. Here is what the evidence supports for each domain.
Alpha-blockers (tamsulosin 0.4 mg, alfuzosin 10 mg, silodosin 8 mg). Best evidence in alpha-blocker-naive men with urinary symptoms (U-domain positive). A 2019 Cochrane review found modest benefit on NIH-CPSI scores compared with placebo, with the largest effects in men who had not previously used these drugs [8]. Expect 4-6 weeks before judging response. Common side effects: dizziness, retrograde ejaculation (especially with silodosin — worth knowing if fertility matters).
Quercetin 500 mg twice daily. A bioflavonoid with anti-inflammatory effects. The Shoskes 1999 randomized trial showed significant symptom improvement at 4 weeks in the quercetin arm versus placebo [9]. Best for O-domain phenotype (organ-specific tenderness). Side effects minimal. Take on an empty stomach for absorption.
NSAIDs (ibuprofen, naproxen). Useful for short-term flare management — not as long-term monotherapy. Prolonged daily use risks gastric, renal, and cardiovascular complications. I use a 7-10 day course during acute exacerbations, not as chronic therapy.
Pregabalin, gabapentin, amitriptyline, duloxetine. For N-domain phenotype with neuropathic features, central sensitization, or fibromyalgia overlap. Duloxetine has the strongest evidence for chronic pelvic pain with mood component — it treats both. Start low, titrate slowly. Expect 4-8 weeks for full effect.
Antibiotics (fluoroquinolones, doxycycline, trimethoprim-sulfamethoxazole). Only if I-domain is positive — meaning a positive culture, atypical organisms identified, or recent confirmed exposure. A single 4-6 week course of a culture-targeted antibiotic is reasonable. Repeat courses without positive cultures are not. The risk of fluoroquinolone tendinopathy alone — including spontaneous Achilles rupture — should give every urologist pause before reaching for ciprofloxacin a third time in a man with negative cultures.
What does not work well in CPPS: 5-alpha reductase inhibitors as monotherapy in young men (some role in older men with prostatic enlargement), botulinum toxin injections (limited evidence), prostatic massage as a treatment (an outdated approach in non-bacterial CPPS), and prostatectomy (absolutely contraindicated — the prostate is not the source of pain in CPPS).
Lifestyle Changes That Actually Move the Needle
The men who do best in my clinic are not the ones who try every drug. They are the ones who change three or four behaviors and stick with them.
- Reduce prolonged sitting. Stand every 30 minutes for two minutes. Use a kneeling chair or saddle stool for desk work. Bicycle commuters with CPPS should switch to upright bars and a noseless saddle, or stop cycling for 8 weeks to test the trigger.
- Eliminate dietary triggers in a structured way. The four most common culprits are caffeine, alcohol, spicy food, and acidic foods (citrus, tomatoes). Remove all four for 4 weeks, then reintroduce one at a time over 2-week intervals. Many men identify one or two clear triggers — coffee is the most common.
- Treat constipation aggressively. Straining at stool spasms the pelvic floor. Aim for daily soft formed stool with adequate fiber (25-30 g daily) and water (2.5 liters per day, or around 85 fl oz / 10 cups).
- Sleep 7-8 hours. Sleep deprivation increases central pain sensitivity. The N-domain phenotype is much harder to manage in chronically sleep-deprived men.
- Address the stress component honestly. CPPS is not “in your head” — but stress modulates pain perception in every chronic pain condition, and CBT specifically targets pain catastrophizing in a way that drugs do not.
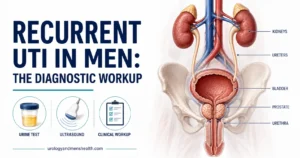
The lifestyle piece overlaps with broader urological health considerations — particularly for men who develop pelvic symptoms alongside other warning signs. If you are also dealing with urinary changes, our guide on UTI in men and when to worry covers the symptom overlap that often confuses the picture. And if your pain started after an episode of acute prostatitis, the differences between that and CPPS are covered in our piece on prostatitis symptoms in young men.
When Standard Treatment Fails — What Comes Next
About 20-25% of men do not achieve adequate improvement with first-line UPOINT-guided therapy. Before declaring treatment failure, the first question is whether the phenotype was correct. Re-examine the pelvic floor. Re-do the NIH-CPSI. Ask honestly whether the patient adhered to the pelvic floor PT or stopped after three sessions because progress felt slow.
For genuine treatment-resistant CPPS, second-line options include:
- Intrapelvic injections. Trigger-point injections with local anesthetic and steroid into the levator ani, performed by an interventional pain specialist. Modest evidence; reserved for focal trigger points that have not released with manual PT.
- Sacral neuromodulation. An implanted device modulating S3 nerve root activity. Limited but real evidence in CPPS with significant urinary symptoms refractory to other measures.
- Pudendal nerve blocks. Diagnostic and sometimes therapeutic for true pudendal neuralgia (a specific entity, not the same as CPPS — characterized by pain in the pudendal nerve distribution worsened by sitting and relieved by sitting on a toilet seat).
- Hyperbaric oxygen therapy. Emerging evidence; not standard of care but reasonable in research-setting protocols.
What I avoid in treatment-resistant CPPS: any irreversible surgical procedure on the prostate, urethra, or pelvic floor. The condition is functional and inflammatory, not structural. Operating on it almost always makes it worse.
Red Flags That Need Immediate Evaluation
Most CPPS is not dangerous, but these features need urgent assessment to rule out other conditions:
- Fever above 38°C (100.4°F) with pelvic pain — possible acute bacterial prostatitis or abscess
- Visible blood in urine (hematuria) — needs cystoscopy and imaging to exclude bladder cancer or stones
- Hard, fixed nodule on prostate examination — prostate cancer evaluation
- Inability to pass urine for more than 8-12 hours — acute urinary retention, an emergency
- Weight loss, night sweats, or bone pain alongside pelvic pain — needs urgent oncological workup
- New-onset erectile dysfunction with severe pain — vascular assessment alongside CPPS treatment
What Realistic Recovery Looks Like
I want to be honest about the timeline because most men are not, and the disappointment when expectations are not met derails treatment. CPPS that has been present for less than six months typically responds within 12 weeks of phenotype-matched treatment. CPPS that has been present for years takes 6-12 months of consistent multi-domain therapy before a meaningful drop in NIH-CPSI scores. Complete symptom resolution happens in maybe 30-40% of patients. Substantial improvement — a return to normal work, relationships, and exercise — happens in 70-80%.
Flares are part of the condition. Even men who are doing well will have a bad week after a stressful work deadline, a long flight, or an infection elsewhere in the body. Flares are not treatment failure. They are part of the natural pattern of a chronic pain condition, and they respond to short-term escalation of whatever worked the first time — a week of NSAIDs, an extra pelvic floor PT session, a few days of warm sitz baths.
The men who recover most fully share three traits: they accepted early that this would be a months-to-years process rather than weeks, they did the pelvic floor work consistently, and they addressed the psychological dimension without treating it as an insult. The men who do worst are the ones who keep searching for a single missed infection, a single drug that will fix everything, or a single surgeon who will operate the pain away. None of those exist.
Frequently Asked Questions
How is chronic prostatitis treatment different when there is no bacterial infection?
For CPPS (NIH Category III), antibiotics are not the answer because there is no bacterial infection to treat. Effective chronic prostatitis treatment uses the UPOINT framework to identify which of six domains is driving your symptoms — urinary, psychosocial, organ-specific, infection, neurologic, or pelvic floor tenderness — and applies a domain-matched intervention. Pelvic floor physical therapy is the single most underused first-line option, with response rates around 70% when muscular tenderness is present. Score your symptoms with the NIH-CPSI before deciding on a treatment plan.
Can CPPS go away on its own without treatment?
Spontaneous resolution happens in roughly 20-25% of men within 12-24 months, but most untreated CPPS persists or worsens. The longer the central nervous system has time to “learn” the pain pattern (central sensitization), the harder it becomes to reverse. Early phenotype-matched treatment within 6 months of symptom onset has substantially better outcomes than treatment started after years of symptoms. The 70-90% of men told they have a “deep infection” who continue antibiotics for months are not getting better — they are getting more sensitized.
What are the most common CPPS symptoms doctors miss?
The three most missed CPPS symptoms are perineal pressure worsened by sitting (often dismissed as “you sit too much”), post-ejaculatory pain that lasts hours or days (often missed because it is embarrassing to mention), and pain referral patterns that mimic other conditions — testicular ache without swelling, penile tip burning without infection, and lower back pain with no spinal cause. A digital rectal exam assessing pelvic floor muscle tenderness (not just prostate texture) is the diagnostic step most often skipped.
How does pelvic pain syndrome in men relate to premature ejaculation or erectile problems?
Sexual dysfunction co-occurs with CPPS in 40-50% of cases. Pelvic floor muscle spasm and chronic pain alter both ejaculatory control and erectile function directly, and anticipatory anxiety about post-ejaculatory pain compounds the problem. Treating the CPPS often improves the sexual symptoms within the same timeframe. If premature ejaculation persists after CPPS treatment, the specific PE treatment pathway applies separately, often with SSRI options that also help the neurologic domain of CPPS.
Is UPOINT phenotyping done in standard urology practices, or only at specialized centers?
UPOINT-guided care is the international standard recommended by both AUA and EAU guidelines, but real-world uptake is patchy. Many general urology practices still default to antibiotic-and-alpha-blocker protocols regardless of phenotype. If your urologist has not assessed your pelvic floor on examination, has not screened for psychosocial domain features, and has not asked about pain outside the pelvis, you are not getting UPOINT-guided care. A second opinion at a urology center with a dedicated chronic pelvic pain or men’s health clinic is reasonable if you have had more than 3 months of unsuccessful treatment.
Can diet really make a meaningful difference in CPPS symptoms?
For some men, yes — but the response is highly individual. Caffeine, alcohol, spicy food, and acidic foods are the four most common dietary triggers identified in cohort studies of CPPS men. A structured elimination of all four for 4 weeks, followed by sequential reintroduction over 2-week intervals, identifies clear triggers in roughly 40% of men. Caffeine is by far the most commonly identified — and the hardest one to give up consistently. Diet alone rarely resolves CPPS, but identifying and eliminating triggers reduces flare frequency and improves the response to other treatments.
References
- Krieger JN, Nyberg L Jr, Nickel JC. NIH consensus definition and classification of prostatitis. JAMA. 1999;282(3):236-237. PubMed
- Engeler D, Baranowski AP, Berghmans B, et al. EAU Guidelines on Chronic Pelvic Pain. European Association of Urology, 2024. EAU Guidelines
- Krieger JN, Riley DE, Cheah PY, et al. Epidemiology of prostatitis: new evidence for a world-wide problem. World J Urol. 2003;21(2):70-74. PubMed
- Litwin MS, McNaughton-Collins M, Fowler FJ Jr, et al. The National Institutes of Health chronic prostatitis symptom index: development and validation of a new outcome measure. J Urol. 1999;162(2):369-375. PubMed
- Shoskes DA, Nickel JC, Rackley RR, Pontari MA. Clinical phenotyping in chronic prostatitis/chronic pelvic pain syndrome and interstitial cystitis: a management strategy for urologic chronic pelvic pain syndromes. Prostate Cancer Prostatic Dis. 2009;12(2):177-183. PubMed
- Polackwich AS, Shoskes DA. Chronic prostatitis/chronic pelvic pain syndrome: a review of evaluation and therapy. Prostate Cancer Prostatic Dis. 2016;19(2):132-138. PubMed
- Anderson RU, Wise D, Sawyer T, Chan CA. Sexual dysfunction in men with chronic prostatitis/chronic pelvic pain syndrome: improvement after trigger point release and paradoxical relaxation training. J Urol. 2006;176(4):1534-1539. PubMed
- Franco JV, Turk T, Jung JH, et al. Pharmacological interventions for treating chronic prostatitis/chronic pelvic pain syndrome. Cochrane Database Syst Rev. 2019;10:CD012552. PubMed
- Shoskes DA, Zeitlin SI, Shahed A, Rajfer J. Quercetin in men with category III chronic prostatitis: a preliminary prospective, double-blind, placebo-controlled trial. Urology. 1999;54(6):960-963. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.