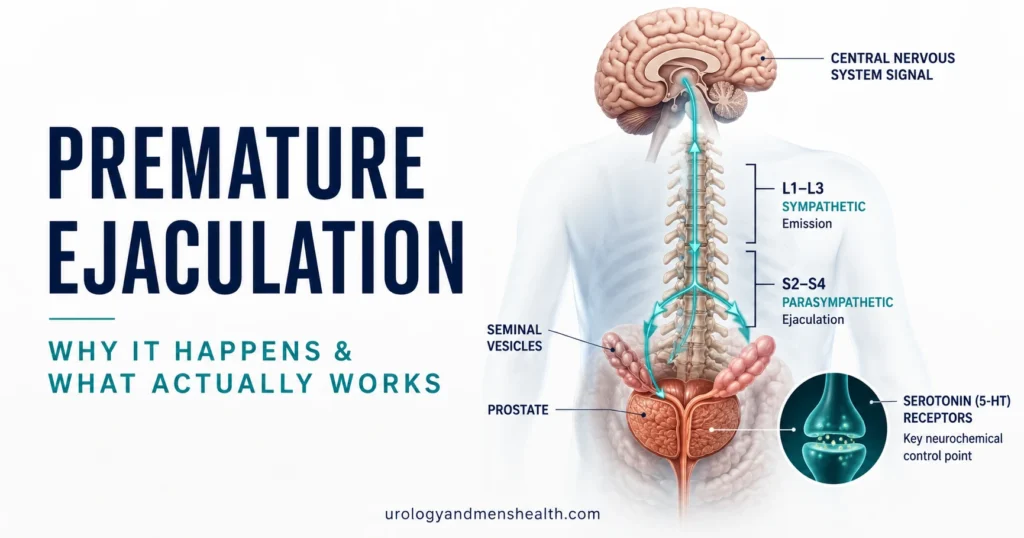
Premature Ejaculation: Why It Happens & What Actually Works
Patients usually suffer in silence for years, assuming a lack of stamina is a permanent personal failure rather than a highly treatable medical condition. The clinical reality is that premature ejaculation is the most common male sexual disorder on earth, and it falls into two completely different biological categories: a lifelong wiring issue, or a newly acquired physical shift. Here is the unfiltered medical protocol I use to identify exactly which mechanism is driving your rapid climax, and the targeted therapies proven to restore control in a matter of weeks.

Premature ejaculation is the most common male sexual disorder worldwide, affecting roughly 20–30% of men at some point in their lives — yet it is also the most under-treated, because most men never bring it up. In clinic, I see two distinct groups: men who have had this since their very first sexual experience, and men whose ejaculatory control was fine for years and then changed. These are biologically different problems with different treatments, and getting that distinction right is the single most important step. The good news is that premature ejaculation responds to treatment in the majority of men — usually within 6 to 12 weeks — once the underlying driver is identified.
Key Takeaways
- Premature ejaculation is defined by an intravaginal ejaculatory latency time (IELT) under 1 minute (lifelong) or a clinically meaningful reduction from previous baseline (acquired), per ISSM 2014 criteria.
- Lifelong and acquired PE are driven by different mechanisms — serotonin receptor sensitivity for lifelong, treatable conditions like anxiety, ED, prostatitis, or hyperthyroidism for acquired.
- Daily SSRIs (paroxetine, sertraline) increase IELT 3- to 8-fold; on-demand dapoxetine increases IELT roughly 2.5- to 3-fold per pooled phase III data.
- Topical lidocaine-prilocaine cream is the highest-yield first-line treatment for many men and is genuinely under-prescribed in primary care.
- Treating co-existing erectile dysfunction first often resolves what looked like premature ejaculation — the two conditions are linked in 30–50% of cases.
What Counts as Premature Ejaculation — The Clinical Definition
The International Society for Sexual Medicine (ISSM) defined premature ejaculation in 2014, and the European Association of Urology adopted the same criteria. Three things must be present: ejaculation that almost always occurs within about one minute of vaginal penetration (for lifelong PE) or a clinically meaningful and bothersome reduction in latency time (for acquired PE), inability to delay ejaculation on all or nearly all penetrations, and negative personal consequences such as distress, frustration, or avoidance of sexual intimacy [1].
That last criterion matters more than men realize. Distress is part of the diagnosis. A man who finishes in two minutes but neither he nor his partner finds it a problem does not have premature ejaculation by clinical definition — he has a sexual style that works for him. Conversely, a man finishing in five minutes who is consumed by anxiety about it may meet diagnostic criteria for acquired PE.
The objective measure clinicians use is intravaginal ejaculatory latency time, or IELT — the time from vaginal penetration to ejaculation, typically measured by stopwatch. In population studies, the median IELT in the general male population is about 5.4 minutes [2]. Men with lifelong PE typically have an IELT under 60 seconds; men with acquired PE usually report IELT under 3 minutes with a meaningful reduction from their prior baseline.
If you want a structured way to see whether your symptoms cross the clinical threshold, the PEDT Premature Ejaculation Diagnostic Tool uses the validated 5-question screen with cutoff scores published in major sexual medicine journals. A score of 11 or above suggests probable PE; 9 or 10 is the diagnostic grey zone.
Lifelong vs Acquired Premature Ejaculation — Why the Distinction Decides Treatment
This is the question I ask every patient first: “Has it always been this way, or did it change?” The answer redirects the entire workup.
Lifelong (Primary) PE
Present from the very first sexual experience. IELT is typically under 60 seconds and has never been longer. The driver is neurobiological — most evidence points to altered serotonin receptor sensitivity, specifically reduced activity at 5-HT2C receptors and increased activity at 5-HT1A receptors in the central nervous system [3]. There is a genetic component; lifelong PE clusters in families. Penile hypersensitivity may contribute in some men but is not the primary mechanism, which is why purely topical treatments work for some lifelong PE patients but not all.
Lifelong PE is the form that responds best to SSRIs and dapoxetine, because these drugs work directly on the serotonin pathway that is the underlying problem.
Acquired (Secondary) PE
Develops after a period of normal ejaculatory function. The IELT was previously 3, 5, 10 minutes — and then dropped. This is the form where the real diagnostic work happens, because acquired PE almost always has an identifiable driver:
- Erectile dysfunction — the most common driver. Men with weakening erections subconsciously rush before they lose firmness, and the rushing pattern becomes wired in.
- Performance anxiety — typically after a stressful sexual experience, a relationship change, or a period of abstinence.
- Chronic prostatitis / chronic pelvic pain syndrome (CPPS) — inflammation lowers the ejaculatory threshold.
- Hyperthyroidism — overactive thyroid raises sympathetic tone and shortens IELT. This resolves with thyroid treatment.
- Recreational drug withdrawal — particularly opioids and benzodiazepines.
- Relationship dynamics — including the situational PE that occurs only with a new partner.
In My Practice
The patient I remember most clearly was a 34-year-old who came to clinic certain he had “developed” lifelong PE in his late twenties — except lifelong PE by definition cannot develop. When I walked him through his timeline he realized his ejaculatory latency had quietly fallen from about 6 minutes to under a minute over 18 months, almost perfectly tracking a period where his morning erections weakened. He did not need an SSRI. He needed his erectile dysfunction treated. Once his erection quality returned on tadalafil 5mg daily, his IELT climbed back to around 4 minutes over 8 weeks without a single dose of dapoxetine or paroxetine.
This pattern — what looks like acquired PE but is actually compensating for early ED — accounts for somewhere between 30 and 50 percent of acquired PE in my clinic, and almost everyone with it has been told by a previous doctor to just try sertraline.
If you suspect your ejaculation issue developed alongside changes in erection quality, screen yourself with the IIEF-5 Erectile Function Assessment before starting any PE treatment. Treating ED first often resolves the apparent PE entirely.
What Actually Causes Premature Ejaculation — The Mechanisms
Ejaculation is a spinal reflex coordinated by sympathetic, parasympathetic, and somatic nerves, with descending modulation from the brain. The two branches of the autonomic nervous system fight for control of the ejaculatory threshold, and serotonin is the most important neurotransmitter setting where that threshold sits. Higher central serotonin activity at the right receptors delays ejaculation; lower activity speeds it up. This is why SSRIs — drugs that increase synaptic serotonin — were noticed to delay ejaculation as a side effect long before they were trialed as a treatment.
For lifelong PE the dominant mechanism is central — serotonin receptor sensitivity inherited from birth. For acquired PE the mechanism is whatever is shifting the ejaculatory threshold in that particular man: a hyperexcitable pelvic floor from chronic prostatitis, a thyroid driving sympathetic overactivity, an anxious cortical state overriding the inhibitory pathways, or an erection that is no longer reliable, training the man to ejaculate fast before things go wrong.
Penile hypersensitivity — the older theory that PE is caused by an over-sensitive glans — has limited evidence as a sole cause. The clinical observation that topical anesthetics help is real, but they help by reducing the volume of afferent signaling to a spinal cord that is already set to a low threshold. The threshold is the problem, not the skin.
ED that is not responding to the usual pills? Download Dr. Khalid’s ED & Sexual Function Action Plan.
Enter your email below to receive Dr. Khalid’s complete ED & Sexual Function Action Plan as a free, printable PDF.
Treatments That Actually Work — A Tiered Approach
The AUA and EAU both recommend a tiered approach: lowest-burden, lowest-side-effect options first, escalating to oral pharmacotherapy when topical and behavioral measures are inadequate. The order I use in clinic follows that logic.
Tier 1: Behavioral Techniques
The start-stop technique (stop stimulation just before the point of ejaculatory inevitability, wait until arousal drops, resume) and the squeeze technique (gentle squeeze of the glans at the same point) are the two classical behavioral approaches. Evidence from Cochrane review suggests they roughly triple baseline IELT in compliant patients, though dropout rates are high and a partner is generally required for effective application [4]. Pelvic floor muscle training — daily Kegels — has surprisingly good evidence in lifelong PE, with one randomized trial showing IELT improvement from about 32 seconds to 146 seconds at 12 weeks.
Behavioral techniques alone are usually insufficient for severe lifelong PE but work well as adjuncts to medication or topicals.
Tier 2: Topical Anesthetics
Lidocaine-prilocaine cream (EMLA, or the prescription PE-specific formulation Fortacin in Europe) applied to the glans 20–30 minutes before intercourse roughly increases IELT by a factor of 4 to 8 in placebo-controlled trials. This is genuinely under-prescribed. Most primary care doctors jump to sertraline without trying lidocaine first, which is backwards — topical anesthetic has dramatically fewer systemic side effects.
The two cautions: it must be washed off or applied under a condom before intercourse to avoid numbing the partner, and a small percentage of men dislike the reduced sensation. Lidocaine spray formulations (such as Fortacin metered-dose spray) avoid the wash-off problem and are now first-line in EAU guidance.
Tier 3: Oral Pharmacotherapy
Two main strategies — daily SSRIs and on-demand dapoxetine.
Daily SSRIs (paroxetine 20mg, sertraline 50–100mg, fluoxetine 20mg, escitalopram 10mg) are the most effective oral option, increasing IELT by a factor of 3 to 8 across studies. Paroxetine consistently shows the largest effect. The trade-off is daily medication, a 2-week onset to full effect, and side effects including nausea, fatigue, reduced libido, and rarely persistent post-SSRI sexual dysfunction. SSRIs are used off-label for PE in most countries, prescribed by urologists and sexual medicine specialists with consent for off-label use.
Dapoxetine (Priligy) is the only SSRI specifically licensed for PE in many countries, including the UK, EU, and Australia. It is short-acting, taken 1–3 hours before intercourse, and increases IELT roughly 2.5- to 3-fold in pooled phase III data [5]. It is not licensed in the United States, where men typically receive off-label sertraline or paroxetine instead. Dapoxetine is less effective than daily SSRIs but avoids the daily-medication burden and has a cleaner safety profile.
The deeper pharmacology of which SSRI to pick for which patient is covered in my detailed guide to SSRIs and dapoxetine for premature ejaculation.
Tier 4: Combination and Cause-Directed Therapy
For men who do not respond to monotherapy, combining lidocaine with an SSRI is more effective than either alone. For men with co-existing ED, a PDE5 inhibitor (tadalafil or sildenafil) combined with dapoxetine or daily SSRI outperforms PE treatment alone — and is the regimen I most often prescribe in clinic for men with both conditions. The 2024 EAU guidelines explicitly endorse this combination for PE with concurrent ED.
For acquired PE driven by an underlying condition — prostatitis, hyperthyroidism, anxiety disorder — treating the underlying condition often resolves the PE without specific PE-directed treatment.
A comparison of when to use numbing creams versus oral pills for premature ejaculation covers the trade-offs in more depth.
When Premature Ejaculation Is Really an Erection Problem
I have already mentioned this but it is worth its own section because of how often it is missed. Roughly 30 to 50 percent of men presenting with acquired PE have undiagnosed or subclinical erectile dysfunction. The clinical mechanism is straightforward: as erection quality declines, the man unconsciously rushes intercourse to finish before losing rigidity. Over weeks and months this rushing pattern conditions a shorter IELT, and by the time the man presents he is genuinely ejaculating prematurely — but the root cause is the erection, not the ejaculation.
Clinically the giveaway is the timeline: an adult man, previously normal IELT, with a gradual decline that correlates with weakening morning erections, reduced erection firmness during foreplay, or partial loss of rigidity during intercourse. The temptation in primary care is to prescribe an SSRI. The right move is to assess erectile function first.
This is covered in detail in the article on ED and cardiovascular health — why morning erections are a vascular check, and the general treatment framework in the step-by-step ED treatment protocol.
When to See a Urologist for Premature Ejaculation
See a Urologist If Any of These Apply
- Your IELT has dropped meaningfully from a previously normal baseline — this is acquired PE and needs a workup to identify the cause.
- PE is accompanied by reduced erection firmness, lost morning erections, or pain on ejaculation — these point to ED, prostatitis, or another treatable condition.
- You have visible blood in the semen, persistent pelvic pain, urinary symptoms, or testicular pain alongside PE.
- PE began shortly after starting a new medication — particularly thyroid medication, decongestants, or stimulants.
- You have tried over-the-counter lidocaine sprays for more than 6 weeks without meaningful benefit.
- PE is causing significant relationship distress or sexual avoidance — this is exactly what treatment is designed to address.
At your appointment, expect questions about IELT (the stopwatch measurement, ideally averaged over a few weeks), whether the problem is lifelong or acquired, whether it happens with all partners or only some, and whether erection firmness, libido, or urinary function have changed. Basic investigations include a focused genital examination, testosterone level if libido is affected, TSH for thyroid function, and a urinalysis if prostatitis is suspected. Imaging or specialist tests are rarely needed for uncomplicated PE.
Bring a completed PEDT screening score to the appointment — it shortens the consultation and gives the urologist an objective baseline to measure treatment response against.
Frequently Asked Questions
Can lifelong premature ejaculation be cured permanently, or only managed?
Lifelong premature ejaculation is currently managed rather than cured. The underlying serotonin receptor biology does not change, but daily SSRIs or on-demand dapoxetine produce sustained IELT improvements as long as the medication is taken. Many men eventually reduce dosage or switch to on-demand-only after a few years of treatment, as confidence and conditioning improve. Combining medication with pelvic floor training and behavioral techniques produces the most durable results. Use the PEDT score to track your response objectively over time.
How long does it take for SSRIs to start working for premature ejaculation?
Daily SSRIs such as paroxetine or sertraline produce a partial effect within the first week, but the full IELT improvement is usually not seen until 2 to 4 weeks of consistent dosing. Dapoxetine works on-demand, with effects from the first dose taken 1 to 3 hours before intercourse. If you have been on a daily SSRI for 6 weeks at a therapeutic dose without meaningful improvement, that medication is unlikely to work for you and a switch — usually to paroxetine, which has the largest effect size — is reasonable. See more on the SSRI options for premature ejaculation.
Are lidocaine sprays or numbing creams safe to use long-term?
Topical lidocaine-prilocaine cream and lidocaine sprays are generally safe for ongoing use when applied correctly, with no documented harm from prolonged regular application. The main practical issues are reduced sensation that some men find unacceptable, the need to wash off or use a condom to avoid numbing the partner, and rare local skin irritation. Persistent use without effect after 6 to 8 weeks suggests the underlying mechanism is more central than peripheral and oral pharmacotherapy may be needed.
Can performance anxiety alone cause premature ejaculation?
Yes — anxiety is one of the most common drivers of acquired premature ejaculation, particularly in men whose IELT was previously normal. The mechanism is sympathetic nervous system overactivation, which raises ejaculatory drive and shortens latency. Treatment with cognitive-behavioral therapy or short-term as-needed medication can be highly effective. If anxiety is the sole driver, daily SSRIs can address both the anxiety and the PE simultaneously, though they should always be started by a doctor familiar with both indications.
Does premature ejaculation get worse with age?
Lifelong premature ejaculation tends to remain stable or sometimes improve modestly with age as men gain experience and confidence. Acquired premature ejaculation, however, often correlates with conditions that increase with age — particularly erectile dysfunction, prostatitis, and metabolic disease — so the prevalence of acquired PE rises in men over 50. If your PE has worsened in your 40s or 50s, a urological assessment is worthwhile because there is usually a treatable driver.
Will treating premature ejaculation affect my fertility or my partner’s chance of conceiving?
None of the standard PE treatments — SSRIs, dapoxetine, lidocaine, behavioral techniques — meaningfully reduce sperm count or quality. Daily SSRIs can occasionally cause ejaculatory volume reduction or delayed ejaculation that complicates timed intercourse for conception; in those cases switching to on-demand dapoxetine, lidocaine spray, or a treatment pause around the fertile window solves the problem. Discuss conception plans with your urologist before starting daily medication so the choice can be tailored.
References
- Althof SE, McMahon CG, Waldinger MD, et al. An update of the International Society of Sexual Medicine’s guidelines for the diagnosis and treatment of premature ejaculation (PE). Sex Med. 2014;2(2):60-90. PubMed
- Waldinger MD, Quinn P, Dilleen M, Mundayat R, Schweitzer DH, Boolell M. A multinational population survey of intravaginal ejaculation latency time. J Sex Med. 2005;2(4):492-497. PubMed
- Waldinger MD. The neurobiological approach to premature ejaculation. J Urol. 2002;168(6):2359-2367. PubMed
- Cooper K, Martyn-St James M, Kaltenthaler E, et al. Behavioral therapies for management of premature ejaculation: a systematic review. Sex Med. 2015;3(3):174-188. PubMed
- McMahon CG, Althof SE, Kaufman JM, et al. Efficacy and safety of dapoxetine for the treatment of premature ejaculation: integrated analysis of results from five phase 3 trials. J Sex Med. 2011;8(2):524-539. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.