Bladder Diverticulum: Symptoms, Causes & Treatment
Most men with a bladder diverticulum don't know they have one — they come to me for "another UTI" or a weak stream that won't quit. The pouch is the part nobody looked for. Here's how I diagnose and treat it.

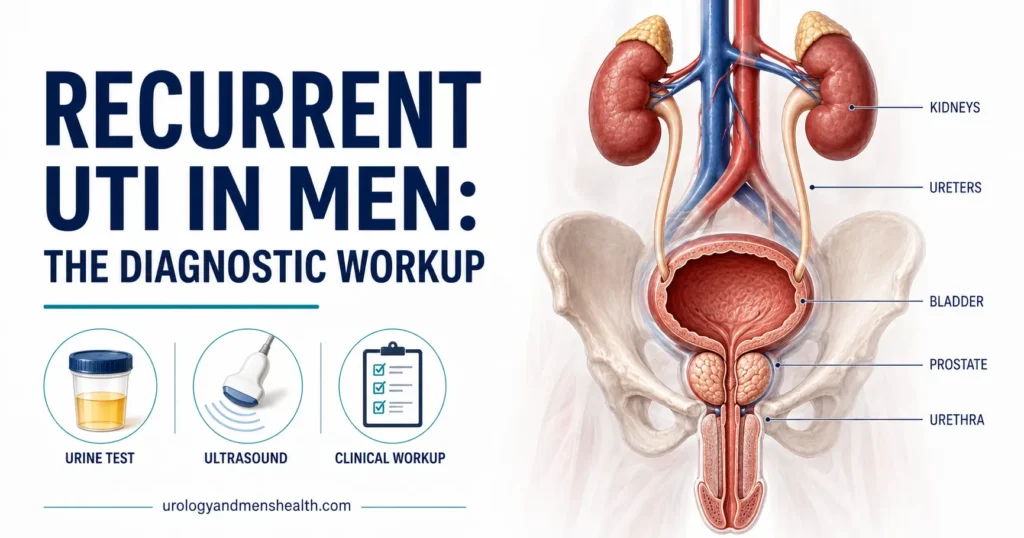
A bladder diverticulum is a pouch that herniates outward from the bladder wall, and most men who have one don’t know it until urine starts misbehaving — a weak stream, an infection that keeps coming back, the strange sensation of needing to urinate twice within a minute. The pouch traps urine that should have left the body. That trapped urine is the problem. In the clinic, I see bladder diverticulum almost always as a downstream signal of something else — usually a long-standing obstruction at the bladder outlet from an enlarged prostate. For the broader picture on how urinary tract infections and obstruction interact in men, see our UTIs and Infections Hub. This guide walks you through what a bladder diverticulum is, why it forms, the symptoms that should raise suspicion, how I diagnose it, and when surgery is the right answer.
Key Takeaways
- A bladder diverticulum is a pouch of mucosa that herniates through the bladder muscle — most are acquired secondary to bladder outlet obstruction, usually from BPH.
- The pouch has no muscle in its wall, so it cannot empty itself; stagnant urine causes recurrent UTIs, stones, and a small but real risk of tumor in older diverticula.
- Diagnosis combines cystoscopy, post-void residual ultrasound, and a CT or MR urogram; urodynamics confirms the underlying outlet obstruction.
- Treatment depends on size and symptoms — small asymptomatic pouches can be observed, but symptomatic diverticula need diverticulectomy combined with relief of the outlet obstruction, or the problem recurs.
What Is a Bladder Diverticulum?
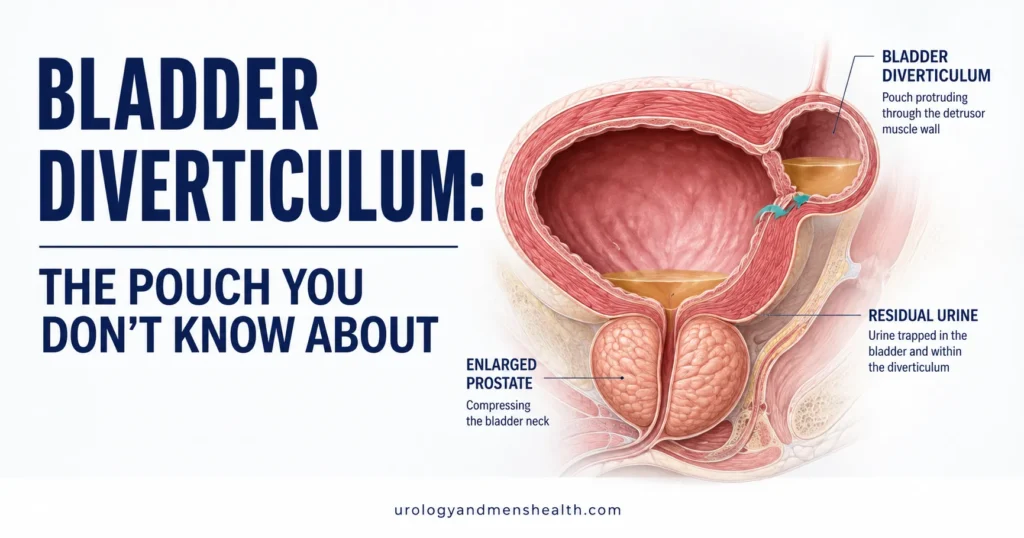
A bladder diverticulum is an outpouching of the inner lining of the bladder (the mucosa) that has pushed its way through gaps in the bladder’s muscle wall. Think of the bladder as a thick muscular balloon. Under normal voiding pressure, the muscle holds the balloon’s shape evenly. When pressure inside the bladder rises chronically — because the outlet is partially blocked — the muscle fibers separate, and the thinner inner lining bulges outward through the weak spots. That bulge becomes a pouch with its own opening into the main bladder, but with one critical difference from the bladder itself: the pouch wall has no muscle.
This is why a bladder diverticulum behaves so differently from the bladder it grew out of. The bladder contracts to empty. The pouch cannot. Whatever urine flows into it during voiding either stays there or flows back into the bladder by gravity after voiding ends. That trapped urine — stagnant, warm, sitting in a closed space — is the root cause of every problem a bladder diverticulum creates.
True versus false diverticula
Urologists distinguish two types. A true diverticulum contains all three layers of the bladder wall (mucosa, muscle, serosa) and is almost always congenital — present from birth, usually solitary, and rare in adults. A false diverticulum (also called acquired or pseudodiverticulum) contains only mucosa and submucosa, with no muscle layer. False diverticula are the kind I diagnose in adult men — they are acquired from years of elevated bladder pressure, and they are the focus of this guide.
What Causes a Bladder Diverticulum in Adults?
In men, the answer is almost always bladder outlet obstruction. The single most common cause is benign prostatic hyperplasia (BPH), where an enlarging prostate compresses the urethra and forces the bladder to push harder against rising resistance. For the full picture on how an enlarged prostate progresses and when surgery enters the conversation, see our guide on BPH treatment and when surgery becomes the answer.
The mechanism is mechanical and slow. A young man’s bladder voids at a pressure of about 30-50 cmH2O. With a partially blocked outlet, that pressure can climb above 80-100 cmH2O during voiding[1]. The detrusor muscle responds first by hypertrophying — the wall thickens, and you can see this on ultrasound as trabeculation, a coarse, ribbed inner surface. Over years, between those thickened muscle ribs, small sacculations appear. Some shrink back; others enlarge into mature diverticula. By the time a 65-year-old man with untreated BPH comes to me with recurrent UTIs, the imaging often shows a trabeculated bladder with one or more diverticula already established.
Other causes of acquired diverticula are less common but worth naming: a urethral stricture (scar tissue narrowing the urethra) produces the same outlet resistance as BPH; neurogenic bladder from spinal cord injury, multiple sclerosis, or diabetes can produce sustained high storage pressure even without anatomical obstruction; and iatrogenic causes include long-standing chronic urinary retention or, rarely, prior bladder surgery that left a weak point in the wall.
In My Practice
A patient comes in with what his primary doctor has called “another UTI.” He has had four in eighteen months. Each one resolves with antibiotics. Each one comes back. He is 67, mentions in passing that his stream has been weak “for years,” and that he sometimes has to urinate again two minutes after he thought he was done. His IPSS is 22. His post-void residual is 180 mL. The ultrasound shows a 4 cm pouch behind his bladder. He does not have “recurrent UTI” as a diagnosis — he has a bladder diverticulum hiding behind decades of unaddressed BPH, and the UTI is what the pouch produces.
Whenever a man over 55 has recurrent UTIs, the diagnostic question is not which antibiotic to choose next — it is what is hiding behind the infections.
Bladder Diverticulum Symptoms: What to Watch For
Most small diverticula cause no symptoms and are found incidentally on a scan ordered for another reason. When bladder diverticulum symptoms do appear, they fall into four overlapping patterns, and any one of them in a man over 50 should prompt a urologist to look for a pouch.
1. Recurrent urinary tract infections
This is the most common presenting symptom in older men. Bacteria thrive in stagnant urine; the pouch is a closed, warm, dilute culture medium that the bladder cannot flush out. A man who has had three or more UTIs in a year, or two in six months, needs a structural workup — not another round of antibiotics. For the broader differential on why infections recur in men, see our guide on UTI in men and when to worry.
2. Double voiding
The classic clinical hallmark. You finish urinating, walk away, and within a minute or two you need to urinate again — and a smaller volume comes out. This is the pouch refilling the bladder by gravity after the main void ends. Patients describe it as “I never feel completely empty.” It is mechanically different from urgency in overactive bladder, where the brain misreads a partially full bladder as urgent. If urgency is your dominant symptom, see our guide on overactive bladder in men; if double voiding is dominant, a diverticulum or post-void residual problem is more likely.
3. Obstructive voiding symptoms
Because the pouch almost always exists because of an obstruction, the underlying obstructive symptoms are usually present too: a weak stream, hesitancy at the start, intermittency mid-stream, terminal dribbling, and the feeling of incomplete emptying. These are the same symptoms men score on the IPSS questionnaire; if you have not done one, the IPSS Prostate Symptom Score Calculator takes about three minutes and gives you a number to bring to your appointment.
4. Pain, blood in the urine, or a stone
Less common but more alarming. Stagnant urine deposits calcium and oxalate over months and years; about 5-10% of diverticula contain a stone at the time of diagnosis[2]. The stone may cause flank or pelvic pain, visible blood in the urine (hematuria), or sudden complete obstruction if it floats into the pouch neck. Hematuria in any man over 40 deserves a urology referral — even if the most likely cause is benign, the workup is the same as for bladder cancer until proven otherwise.
Red Flags — See a Urologist Promptly
Book a urology appointment within 2-4 weeks if you have any of these:
- Three or more UTIs in a year, or two in six months
- Visible blood in the urine, even once
- The clear sensation of needing to void again immediately after finishing
- A post-void residual measured at over 100 mL on ultrasound
- New or worsening weak stream alongside any of the above
Go to the emergency room if you cannot urinate at all, have a fever over 38.5°C (101.3°F) with flank or pelvic pain, or pass blood clots large enough to block your stream.
Stuck in the UTI–antibiotic loop? Find out what’s really going on.
Enter your email below to receive Dr. Khalid’s complete Recurrent UTI Eradication Protocol as a free, printable PDF — the same diagnostic flow I use in clinic to find hidden causes like a bladder diverticulum.
Complications of an Untreated Bladder Diverticulum
The diverticulum itself is not malignant. The complications are the reason we treat it.
- Recurrent infection. Urine that sits inside the pouch becomes a sustained bacterial reservoir. Even successful antibiotic treatment of the bladder leaves bacteria inside the pouch, which seed the next infection within weeks.
- Bladder stones. Stagnant urine concentrates minerals; about 1 in 10 diverticula develops a stone over time[2]. Once a stone forms, the cycle of infection and irritation accelerates.
- Upper urinary tract damage. If the diverticulum sits near the ureteral opening — where urine enters the bladder from the kidney — its mass effect can obstruct the ureter, causing hydronephrosis (urine backing up into the kidney) and, eventually, kidney damage.
- Acute urinary retention. A stone or thickened mucus inside the pouch can shift into the pouch neck and suddenly block bladder emptying. This is a urological emergency. Our guide on acute urinary retention covers what to do.
- Tumor formation. The lifetime risk of a tumor developing inside a long-standing diverticulum is about 2-7%, higher than the surrounding bladder[3]. Because the pouch wall has no muscle, any tumor that does form invades through the wall more easily — making early-stage diverticular tumors more aggressive than tumors of the same stage in the bladder proper. This is why I always biopsy or carefully inspect the interior of a diverticulum at cystoscopy.
How a Bladder Diverticulum Is Diagnosed
The diagnostic workup answers three questions: does a diverticulum exist, what is causing it, and is it causing the symptoms? A pouch found incidentally on a CT scan in a man without symptoms is a different clinical situation from the same pouch in a man with three UTIs and a post-void residual of 200 mL.
Step 1: Post-void residual ultrasound
This is the first test I order in any man with recurrent UTIs or obstructive voiding symptoms. You urinate normally, then a bladder ultrasound measures how much urine is left. A post-void residual (PVR) over 100 mL is abnormal in adults; over 300 mL is significant. A diverticulum can artificially raise the PVR because the ultrasound sees both the bladder and the pouch as one volume. If you want to know what your PVR number means before your appointment, use the Post-Void Residual Danger Estimator and bring the result with you. For deeper context on the test itself, see our explainer on post-void residual urine and what it means.
Step 2: Cystoscopy
Direct visualization. A thin flexible scope passes through the urethra into the bladder, and I look at the inside of the bladder under saline distension. A diverticulum appears as a dark oval opening in the bladder wall, usually posterolateral or near the trigone. I inspect the inside of the pouch when the opening is wide enough, looking for stones, plaques of inflammation, or any suspicious lesion that might need biopsy. Cystoscopy also confirms the underlying obstruction — the prostate’s appearance, the size of any median lobe, and whether the bladder shows trabeculation.
Step 3: Cross-sectional imaging
CT urogram (CT with intravenous contrast captured during the urinary phase) gives the most complete picture: it shows the size and shape of the pouch, its position relative to the ureters, any contained stones, and the bladder anatomy. MR urogram is an alternative for men who cannot have iodinated contrast — equally accurate, no radiation, but more expensive and less available. For a diverticulum being considered for surgery, the surgical team needs cross-sectional imaging; cystoscopy alone is not enough to plan the operation.
Step 4: Urodynamics
Urodynamic testing — measuring pressure and flow during a controlled bladder fill and void — is the gold standard for confirming bladder outlet obstruction and for distinguishing obstruction from a poorly contracting bladder muscle. It matters because the management is different: if the bladder muscle is weak (detrusor underactivity) rather than the outlet being blocked, opening the outlet surgically will not solve the emptying problem. AUA guidelines recommend urodynamics before surgical intervention when the clinical picture is mixed[2].
Bladder Diverticulum Treatment Options
Treatment depends on three things: the size of the diverticulum, whether it is causing symptoms or complications, and the underlying cause. There are three broad pathways.
Option 1: Observation
Small (under 3 cm), asymptomatic diverticula found incidentally on imaging — especially in an older man with significant other medical problems — can be watched. Follow-up is a yearly post-void residual ultrasound, plus a repeat scan every 2-3 years to check for size progression, stone formation, or any new wall thickening that might indicate tumor development. If symptoms emerge or the size grows, we move to active treatment.
Option 2: Treat the underlying obstruction first
For men with moderate BPH driving a moderate diverticulum, opening the prostate often is the right first step. TURP (transurethral resection of the prostate) or HoLEP (holmium laser enucleation of the prostate) relieves the outlet pressure that produced the pouch. In small diverticula, the pouch can partially shrink once the high voiding pressures resolve, and the recurrent infections often stop because the bladder finally empties. This works best when the diverticulum is small to moderate, the bladder muscle still contracts well on urodynamics, and the pouch sits away from the ureteral openings.
Option 3: Diverticulectomy
Diverticulectomy is surgical excision of the pouch and closure of the resulting defect in the bladder wall. It is the definitive treatment for large symptomatic diverticula, diverticula containing stones, and any diverticulum suspected of harboring a tumor. The approach is open, laparoscopic, or robotic, depending on the size, position, and the surgeon’s training. AUA and EAU guidance both recognize robotic diverticulectomy as a reasonable approach in centers with the right expertise[4].
Critically, diverticulectomy alone almost never fixes the problem — if the BPH or stricture that caused the pouch is still there, a new pouch can form, or recurrent symptoms continue. The outlet obstruction must be treated in the same operation or shortly before. Most often this means a TURP or HoLEP combined with diverticulectomy under the same anesthesia.
What recovery looks like
An indwelling urethral catheter stays in place for 10-14 days to let the bladder closure heal under low pressure. Before catheter removal, a cystogram (a contrast X-ray of the bladder) confirms no leakage at the repair. Most men return to desk work in 2-3 weeks and to heavier activity in 6 weeks. The recurrent UTIs that drove the diagnosis usually stop within 1-2 months, once the pouch and the outlet are both fixed. Post-void residual normalizes over the first few months as the chronically stretched bladder muscle recovers some tone.
Frequently Asked Questions
Can a bladder diverticulum go away on its own?
A mature acquired bladder diverticulum will not fully disappear on its own — the herniated mucosa is permanent. However, a small diverticulum can partially shrink and become symptomatically silent once the underlying outlet obstruction is relieved, for example after a successful TURP or HoLEP. Larger diverticula stay the same size or grow, and observation alone is only appropriate for small, asymptomatic pouches found incidentally.
How do I know if my recurrent UTIs are from a bladder diverticulum versus something else?
The pattern matters more than the count. Recurrent UTIs in a man over 50 with a weak stream, double voiding, or a measured post-void residual over 100 mL strongly point toward a structural cause — and a bladder diverticulum is one of the top suspects. The workup is the same either way: post-void residual ultrasound, cystoscopy, and a CT or MR urogram. Younger men with recurrent UTIs more often have other causes, which our guide on UTI in men covers in detail.
Is bladder diverticulum surgery dangerous?
Diverticulectomy is a well-established operation with a complication rate in the 5-10% range at experienced centers[4]. The main risks are bleeding, urinary leak from the repair site (which is why we use a catheter for 10-14 days), injury to the nearby ureter if the pouch sits close to the ureteral opening, and the usual anesthetic risks. The risk-benefit calculation favors surgery for any symptomatic diverticulum, because the alternative — continued recurrent infection, stone formation, and the small but real tumor risk — is worse over time.
Can a bladder diverticulum cause cancer?
The diverticulum itself is not a cancer. However, the lifetime risk of a tumor developing inside a long-standing bladder diverticulum is about 2-7%, which is higher than in the rest of the bladder[3]. Because the pouch wall has no muscle, any tumor that forms invades through the wall earlier than the same tumor would in the bladder proper, making early diagnosis important. This is why we inspect the inside of every diverticulum at cystoscopy and biopsy anything suspicious.
What is the difference between a bladder diverticulum and an overactive bladder?
They are entirely different problems with overlapping symptoms. A bladder diverticulum is a structural pouch on the bladder wall that traps urine; overactive bladder is a functional problem where the bladder muscle contracts at low volumes, producing urgency. The key clinical signal is what dominates: if double voiding and recurrent UTIs dominate, look for a diverticulum; if urgency and frequency without infection dominate, see our guide on overactive bladder in men. Some older men have both, and the diagnostic workup separates them.
Will I need a catheter for the rest of my life after diverticulectomy?
No. The catheter is temporary — 10-14 days after surgery to let the bladder closure heal. After that, most men urinate normally, often better than they did before surgery if the BPH was treated at the same time. Long-term catheter use is only needed in the small subset of men whose bladder muscle has been so chronically overstretched that it does not regain effective contraction even after the obstruction is relieved; urodynamic testing identifies this before surgery so the conversation is honest.
References
- Abrams P, Cardozo L, Wagg A, Wein A (eds). Incontinence: 6th International Consultation on Incontinence. ICI-ICS. International Continence Society; 2017. ICS
- Sandhu JS, Bixler BR, Dahm P, et al. Management of Lower Urinary Tract Symptoms Attributed to Benign Prostatic Hyperplasia: AUA Guideline Amendment 2023. J Urol. 2024;211(1):11-19. AUA
- Tamas EF, Stephenson AJ, Campbell SC, et al. Histopathologic features and clinical outcomes in 71 cases of bladder diverticula. Arch Pathol Lab Med. 2009;133(5):791-796. PubMed
- Gratzke C, Bachmann A, Descazeaud A, et al. EAU Guidelines on the Assessment of Non-neurogenic Male Lower Urinary Tract Symptoms including Benign Prostatic Obstruction. Eur Urol. 2015;67(6):1099-1109. EAU
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.