UTI in Men: When It’s Not Normal | Urologist Guide
When a man develops a urinary tract infection, the default response at an urgent care clinic is usually a quick round of antibiotics and a pat on the back. The dangerous reality is that a male UTI is fundamentally different from a female UTI. Because of male anatomy, bacteria rarely reach the bladder unless an underlying structural issue—like an enlarged prostate, a urethral stricture, or even a hidden tumor—is actively helping them get there. Here is the unfiltered clinical truth about why a male UTI is never just a simple infection, and the exact medical investigations you need once the antibiotics run out.


When a woman gets a UTI, her primary care doctor prescribes antibiotics and moves on. When a man gets a UTI, I want to know why. That single word — why — is the difference between appropriate medicine and a missed diagnosis.
UTI in men are fundamentally different from UTIs in women. The male urethra is approximately 20 cm long (around 8 inches) — four to five times the length of the female urethra — and this anatomical advantage means bacteria must overcome a far greater distance to reach the bladder. When they succeed, it almost always means something is helping them get there: an enlarged prostate blocking complete bladder emptying, a urethral stricture creating turbulent flow, a kidney stone harboring bacteria, or — worst case — a bladder tumor providing a surface for infection.
A UTI in a man over 50 should never be treated with antibiotics and forgotten. It should be treated with antibiotics and investigated. In my clinic, approximately 1 in 10 men referred for recurrent UTIs turns out to have a structural abnormality that was driving the infections all along. This article explains what every man needs to know — the real causes, the red flags, and when a “simple UTI” is anything but simple.
Key Takeaways
- UTIs in men are uncommon and should always be investigated — unlike in women, they are rarely “simple” and almost always have an underlying structural or functional cause.
- The most common cause in men over 50 is incomplete bladder emptying from BPH — residual urine acts as a breeding ground for bacteria [1].
- Never treat without a urine culture — empirical antibiotics without culture are a major driver of antibiotic resistance and missed diagnoses.
- Visible blood in urine (hematuria) with a UTI in a man over 40 warrants investigation for bladder cancer — do not dismiss it as “just the infection.”
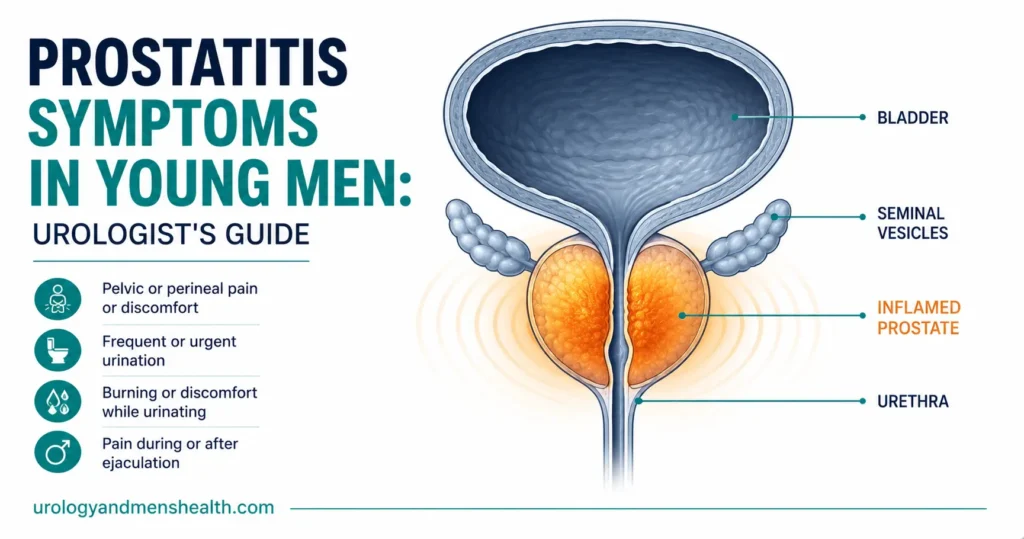
- Many men diagnosed with “recurrent UTIs” actually have chronic prostatitis — a different condition requiring different treatment [2].
- A first UTI in a young man (under 40) should prompt screening for STIs and structural abnormalities.
- Cranberry supplements have minimal evidence for UTI prevention in men — adequate hydration and treating the underlying cause are far more effective.
Why Are UTIs in Men Different?
The male urinary tract has several natural defense mechanisms that make infections rare compared to women. The long urethra is the most obvious barrier, but the prostate gland also contributes — prostatic fluid contains zinc and other antimicrobial substances that inhibit bacterial growth [3]. The dry environment around the male urethral opening is also less hospitable to gut bacteria than the female periurethral area.
The result is stark: UTIs affect approximately 3% of men annually, compared to 12–15% of women [4]. When a man does develop a UTI, the odds that it is “just bad luck” are low. In most cases, something has compromised one or more of these natural defenses.
This is why the European Association of Urology (EAU) classifies UTIs in men as “complicated” by definition — meaning they warrant investigation beyond a simple prescription [5]. Unfortunately, in primary care, many male UTIs are still treated as though they were female UTIs: a quick dip test, empirical antibiotics, and no follow-up. This approach misses diagnoses, promotes antibiotic resistance, and puts patients at risk.
The Real Causes — What’s Driving the Infection
1. Benign prostatic hyperplasia (BPH) — the most common culprit over 50
An enlarged prostate compresses the urethra and prevents the bladder from emptying completely. The urine that remains after voiding — called post-void residual (PVR) — is a stagnant pool of warm, nutrient-rich fluid. Bacteria love it. Studies show that a PVR above 100 mL (about 3.4 fl oz) significantly increases UTI risk in men with BPH [1].
The infection isn’t the problem — the obstruction is. Until the obstruction is addressed (with medication or surgery), UTIs will keep recurring no matter how many courses of antibiotics you take.
2. Urethral stricture
A narrowing of the urethra — often from prior instrumentation (catheterization, cystoscopy), previous gonorrhea infection, or trauma — creates turbulent urine flow and incomplete emptying. Like BPH, it creates the conditions bacteria need to thrive. Stricture-related UTIs tend to present with a weak or split stream alongside infection symptoms.
3. Kidney or bladder stones
Stones provide a physical surface on which bacteria can form biofilms — structured bacterial communities that are 100–1,000 times more resistant to antibiotics than free-floating bacteria [6]. This is why stone-related UTIs are notoriously difficult to eradicate with antibiotics alone. The stone must be removed to eliminate the infection reservoir.
Struvite stones (magnesium ammonium phosphate) are particularly concerning because they are caused by certain bacteria (Proteus, Klebsiella) that produce urease, alkalinize urine, and promote stone formation — creating a self-sustaining infection-stone cycle.
4. Catheterization
Any man with an indwelling urinary catheter will develop bacteriuria (bacteria in urine) within 2–4 weeks — this is essentially universal. The catheter provides a direct highway for bacteria to ascend from the skin into the bladder, bypassing all natural defenses. Catheter-associated UTIs (CAUTIs) account for approximately 40% of all hospital-acquired infections [7].
5. Diabetes mellitus
Diabetes impairs immune function, promotes glucosuria (sugar in urine that feeds bacteria), and causes autonomic neuropathy that impairs bladder emptying. Diabetic men have 2–3 times the UTI rate of non-diabetic men, and their infections tend to be more severe and more likely to involve resistant organisms [8].
6. Bladder cancer — the diagnosis nobody wants to miss
This is the reason every urologist takes male UTIs seriously. Bladder tumors can present as recurrent UTIs or as a UTI with hematuria. A tumor disrupts the normal bladder mucosal barrier, creating an environment conducive to secondary infection. In my practice, any man over 40 with a UTI and visible hematuria gets a cystoscopy — no exceptions. The UTI may be the presenting symptom that leads us to an early, treatable cancer.
→ Related Read: The 40+ Men’s Health Checklist — The 5 Tests You Actually NeedSymptoms — What a Male UTI Actually Feels Like
The classic symptoms of a lower UTI (cystitis) in men are similar to women, but men tend to present later because they dismiss early symptoms or attribute them to “prostate trouble”:
- Dysuria — burning or stinging during urination. This is usually the symptom that finally drives men to seek help.
- Frequency and urgency — needing to urinate more often than usual, with a sudden compelling urge that is difficult to defer.
- Cloudy or foul-smelling urine — bacterial metabolism produces volatile compounds that change urine odor.
- Suprapubic discomfort — a dull ache or pressure sensation in the lower abdomen, above the pubic bone.
- Hematuria — blood in the urine, either visible (frank hematuria) or detected only on dipstick (microscopic hematuria).
When the infection involves the prostate or kidneys
If bacteria ascend into the prostate (acute bacterial prostatitis) or up to the kidneys (pyelonephritis), the clinical picture changes dramatically:
- Fever, rigors, and systemic illness — high temperature (above 38°C / 100.4°F), shaking chills, malaise. This is no longer a localized infection — it is now systemic.
- Perineal or rectal pain — suggests prostatic involvement. The prostate is exquisitely tender on examination.
- Loin or flank pain — suggests pyelonephritis (kidney infection). Pain is typically one-sided, deep, and constant.
- Acute urinary retention — the swollen, infected prostate can compress the urethra so severely that the patient cannot urinate at all. This is a urological emergency requiring catheterization.
Diagnosis — Why a Urine Culture Is Non-Negotiable
The single most important message I can convey about a UTI in men is this: never accept treatment based on a urine dipstick alone. A dipstick test detects nitrites and leukocyte esterase, which suggest infection — but they do not tell you which organism is responsible or which antibiotics it is sensitive to.
A midstream urine (MSU) culture identifies the exact bacterium and its antibiotic sensitivity pattern. In an era of rising antibiotic resistance — where up to 30% of E. coli (the most common UTI pathogen) are resistant to trimethoprim in many regions [9] — prescribing without a culture is guesswork. And in men, where the underlying cause matters far more than in women, a culture also helps distinguish true infection from contamination or prostatitis.
What I investigate beyond the culture
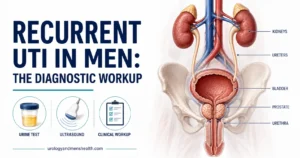
For any man presenting with a UTI, I perform or arrange the following — especially if he is over 40 or has recurrent episodes:
- Flow rate and post-void residual ultrasound — assesses for bladder outflow obstruction (BPH, stricture).
- Renal and bladder ultrasound — checks for stones, hydronephrosis, and bladder wall thickening.
- PSA — if BPH is suspected (but only after the acute infection has resolved, as infection falsely elevates PSA).
- Flexible cystoscopy — for any man over 40 with hematuria, recurrent UTIs, or abnormal imaging.
- CT urogram — if stones, upper tract pathology, or tumor is suspected.
This may seem like a lot for “just a UTI.” But the purpose is to find the reason for the infection, not just treat its symptoms. A UTI in a man is a symptom, not a diagnosis.
Treatment — Getting It Right the First Time
Antibiotic selection
For uncomplicated lower UTIs in men, the EAU guidelines recommend treatment for 7 days — not the 3-day course used in women. This longer course is necessary because of the risk of prostatic involvement, which requires adequate tissue penetration [5].
First-line agents (pending culture results):
- Trimethoprim 200 mg twice daily for 7 days — effective if local resistance rates are below 20%.
- Nitrofurantoin 100 mg twice daily for 7 days — excellent for lower UTIs but does not penetrate prostate tissue. Do not use if prostatic involvement is suspected.
- Fluoroquinolones (ciprofloxacin, levofloxacin) — reserved for prostatic involvement, pyelonephritis, or resistant organisms. These have the best prostate tissue penetration but carry significant side-effect risks (tendon damage, neuropathy, C. difficile) and should not be used as first-line for uncomplicated lower UTIs [10].
Always adjust antibiotics once culture results return. If the culture shows a different sensitivity pattern, switch to the narrowest-spectrum effective agent. This is basic antibiotic stewardship, and it matters enormously in the context of global resistance.
Treating the underlying cause
Antibiotics treat the infection. They do not treat the reason the infection occurred. The long-term strategy must address the underlying problem:
- BPH — alpha-blockers (tamsulosin) and/or 5-alpha-reductase inhibitors (finasteride) to improve voiding and reduce residual urine. Surgery (TURP, HoLEP) for severe cases.
- Stricture — urethral dilatation or urethroplasty.
- Stones — complete stone removal is essential; antibiotics cannot eradicate bacteria within a stone biofilm.
- Bladder cancer — TURBT (transurethral resection of bladder tumor) followed by surveillance.
💡 In My Practice
The pattern I encounter most often is a man in his 60s or 70s who has been treated for three, four, or even five UTIs by his primary care doctor over the preceding 12 months — always with empirical trimethoprim, sometimes without a culture, and always without investigation into the underlying cause. When these patients finally reach my clinic, a bladder ultrasound almost invariably shows 150–250 mL (about 5–8 fl oz) of post-void residual urine from an obstructed, poorly emptying bladder. The prostate has been expanding silently for years. The infection is not the disease — it is the signal. Until the obstruction is addressed, no antibiotic regime on earth will prevent recurrence.
The cases that occupy most of my clinical concern are those presenting with frank hematuria alongside a UTI. My threshold for cystoscopy in this situation is low and deliberate: any man over 40 with visible blood in the urine gets a flexible cystoscopy once the acute infection has cleared. On two separate occasions within the past two years, this approach revealed early-stage transitional cell carcinoma of the bladder in men whose hematuria might otherwise have been dismissed as a consequence of the infection alone. Early detection in both cases allowed curative endoscopic resection. Hematuria during a UTI is not reassuring — it is an indication for investigation.
I see a significant number of men who have been prescribed four or more courses of antibiotics for what was labeled recurrent UTI, when the actual diagnosis is chronic bacterial prostatitis or chronic pelvic pain syndrome. The distinction matters enormously because these conditions require completely different treatments. A urine culture that returns negative in a symptomatic patient is the first clue you are not dealing with a simple bladder infection. When I take a full history and ask about perineal discomfort, incomplete emptying, and pain after ejaculation — symptoms nobody had asked about — the picture often becomes clear within minutes of the consultation.
One factor I encounter regularly in my patient population is the use of herbal preparations — various traditional formulations and internet-purchased supplements — as first-line treatment before seeking medical review. This delays presentation, can partially mask symptoms, and occasionally complicates the diagnostic picture. I now ask about this routinely at first consultation, framing the conversation without judgment. The goal is disclosure, not criticism — and these conversations have changed management on more than one occasion.
Stuck in a cycle of recurrent UTIs? Download Dr. Khalid’s Recurrent UTI Eradication Protocol.
Enter your email below to receive Dr. Khalid’s complete Recurrent UTI Eradication Protocol as a free, printable PDF.
Prevention — What Actually Reduces Recurrence
The internet is full of UTI prevention advice — cranberry juice, probiotics, D-mannose — but for men, the evidence is thin. Here is what actually works:
- Address the underlying cause — by far the most effective prevention strategy. If BPH is causing incomplete emptying, no amount of cranberry extract will prevent recurrence.
- Adequate hydration — 2–2.5 liters of fluid daily (around 70–85 fl oz / 8–10 cups) dilutes urine and increases voiding frequency, flushing bacteria before they can establish infection.
- Complete bladder emptying — double voiding (urinating, waiting 30 seconds, then trying again) can reduce PVR in men with mild obstruction.
- Good hygiene — particularly important for uncircumcised men, where bacteria can colonize the subpreputial space. Gentle daily retraction and cleaning reduces bacterial load.
- Cranberry products — the evidence for UTI prevention in men is virtually non-existent. The modest evidence that exists is in women, and even there, the effect size is small [11]. I do not routinely recommend cranberry supplements to male patients.
Common Misdiagnoses — When It’s Not Actually a UTI
Chronic prostatitis / CPPS
This is the most common misdiagnosis I see. A man presents with urinary frequency, perineal discomfort, and perhaps mild dysuria. A dipstick shows leukocytes. He is diagnosed with a UTI and given antibiotics. The symptoms improve partially, return when antibiotics stop, and the cycle repeats. After three or four courses, someone finally sends a proper urine culture — which comes back negative.
What he actually has is chronic prostatitis / chronic pelvic pain syndrome (CPPS) — a non-bacterial inflammatory condition that antibiotics cannot cure. It requires a completely different approach: alpha-blockers, anti-inflammatories, pelvic floor physiotherapy, and time [2]. Misdiagnosing CPPS as recurrent UTIs leads to unnecessary antibiotic exposure and months of frustration.
Sexually transmitted infections
In sexually active men under 40, many apparent UTIs are actually urethritis caused by chlamydia or gonorrhea. The symptoms overlap significantly — burning on urination, urethral discharge (though this may be subtle), and frequency. A standard MSU culture will miss these organisms. If STI is suspected, specific nucleic acid amplification tests (NAATs) on a first-void urine sample are required.
Overactive bladder
Frequency and urgency without dysuria in an older man is more likely overactive bladder (OAB) than UTI, especially if urine culture is negative. This is a bladder muscle problem, not an infection, and is treated with bladder training and anticholinergic or beta-3 agonist medications.
⚠️ When to See a Doctor — Urgently
- Fever above 38°C (100.4°F) with urinary symptoms — suggests the infection has spread beyond the bladder to the prostate (acute prostatitis) or kidneys (pyelonephritis). May require IV antibiotics and hospital admission.
- Visible blood in urine alongside UTI symptoms — especially if you are over 40. Must be investigated for bladder cancer once the infection is treated.
- Complete inability to urinate (urinary retention) — a medical emergency. Go to the emergency room (ER) immediately. This can occur with acute prostatitis when the swollen prostate blocks the urethra completely.
- Three or more UTIs in 12 months — recurrent UTIs in a man mandate specialist investigation. Do not accept repeated courses of antibiotics without a workup.
- UTI symptoms that persist despite completing a full antibiotic course — suggests a resistant organism, incorrect diagnosis (prostatitis, STI), or an undiscovered structural problem.
- Confusion, rapid heart rate, or feeling very unwell with a UTI — suggests urosepsis, a life-threatening condition where infection enters the bloodstream. Call 911 or your local emergency number.
Frequently Asked Questions
Is it normal for men to get UTIs?
No — that is the central message of this article. A UTI in men is uncommon (affecting approximately 3% per year compared to 12–15% in women), and when it occurs, it usually has an identifiable underlying cause. A healthy young man with a normal urinary tract should not be getting UTIs. If you have had one, it is worth investigating; if you have had two or more, it is essential. See our 40+ men’s health checklist for the full screening picture.
Can a UTI in a man be sexually transmitted?
A standard UTI (caused by E. coli or similar gut bacteria) is not sexually transmitted. However, urethritis caused by chlamydia or gonorrhea mimics UTI symptoms closely — burning on urination, discharge, and frequency. These are sexually transmitted and require specific testing (NAAT on first-void urine) and partner notification. If you are sexually active and develop UTI symptoms, especially with urethral discharge, ask your doctor to test for STIs alongside the standard urology workup.
Do cranberry supplements prevent UTIs in men?
The evidence is negligible. Most cranberry research has been conducted in women, and even in that population, the benefit is modest at best. In men, where UTIs are driven by structural and functional causes (BPH, stones, strictures), no cranberry product addresses the underlying problem. Adequate hydration and addressing the root cause are far more effective strategies. Read our men’s health checklist for the actual evidence-based screening priorities.
How long should antibiotics be taken for a male UTI?
The EAU recommends 7 days for uncomplicated lower UTIs in men — longer than the 3-day course used in women. If the infection involves the prostate (acute bacterial prostatitis), treatment extends to 2–4 weeks, using an antibiotic with good prostatic penetration (typically a fluoroquinolone or trimethoprim). Completing the full course is critical, even if symptoms resolve early — stopping early promotes resistance and relapse. More on prostatic infection in our prostatitis guide.
Should I worry about antibiotic resistance with a UTI in men?
Yes, and you should insist on a urine culture before starting treatment. Empirical antibiotics chosen without culture data are wrong approximately 20–30% of the time, meaning you take a full course of medication that does nothing for the actual organism while breeding resistance. If your primary care doctor prescribes antibiotics based on a dipstick alone, politely ask for a culture to be sent alongside — see our checklist for what every man over 40 should request at the appointment.
📚 References
- Meigs JB, et al. Incidence rates and risk factors for acute urinary retention: the health professionals follow-up study. J Urol. 2004;172(4 Pt 1):1424–1428. PubMed
- Krieger JN, et al. NIH consensus definition and classification of prostatitis. JAMA. 1999;282(3):236–237. PubMed
- Fair WR, et al. Prostatic antibacterial factor: identity and significance. Urology. 1976;7(2):169–177. PubMed
- Foxman B. Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Am J Med. 2002;113(Suppl 1A):5S–13S. PubMed
- Bonkat G, et al. EAU Guidelines on Urological Infections. European Association of Urology. 2024. EAU Guidelines
- Costerton JW, et al. Bacterial biofilms: a common cause of persistent infections. Science. 1999;284(5418):1318–1322. PubMed
- Hooton TM, et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults. Clin Infect Dis. 2010;50(5):625–663. PubMed
- Nitzan O, et al. Urinary tract infections in patients with type 2 diabetes mellitus: review of prevalence, diagnosis, and management. Diabetes Metab Syndr Obes. 2015;8:129–136. PubMed
- Public Health England (now UKHSA). English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report. 2023. UK Gov
- European Medicines Agency. Restrictions on use of fluoroquinolone and quinolone antibiotics. 2019. EMA
- Jepson RG, et al. Cranberries for preventing urinary tract infections. Cochrane Database Syst Rev. 2012;10:CD001321. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.