Erectile Dysfunction Treatment: A Urologist’s Protocol
Patients usually try a borrowed pill or a random internet supplement, watch it fail, and quietly accept that their ED is permanent. The truth is, the problem is rarely that treatments don't work; it's that you are throwing a generic band-aid at a complex vascular or hormonal failure. This guide outlines the exact, step-by-step clinical protocol I use to identify the true cause of your failing erections and match it with the treatment that actually restores them.

Most men who walk into my clinic for erectile dysfunction treatment have already tried “something” — a sildenafil tablet from a friend, herbal supplements from the internet, lifestyle videos on YouTube. When it did not work, they concluded the problem was unfixable. It almost always isn’t. The reason most ED treatment fails is not that the medications don’t work — it is that the wrong medication is being used, at the wrong dose, for the wrong cause.
ED is not a single disease. It is a symptom with at least six major causes — vascular, hormonal, neurological, medication-induced, psychogenic, and penile structural — and often a combination. A protocol that treats “ED” generically will help some men and miss many. A protocol that diagnoses the underlying cause first and then matches treatment to mechanism delivers very different results. This article walks you through the exact step-by-step approach I use in clinic, the same approach recommended by the American Urological Association and European Association of Urology guidelines [1][2].
One important point before we start: erectile dysfunction is often the first warning sign of underlying cardiovascular disease. The small arteries of the penis narrow before the larger arteries of the heart, meaning ED can precede a heart attack by 3 to 5 years [3]. Before anyone prescribes a pill, the cardiovascular and hormonal workup is non-negotiable. You cannot fix the erection without fixing what caused it to fail.
📋 Key Takeaways
- ED is a symptom, not a disease — the treatment depends entirely on identifying the underlying cause (vascular, hormonal, neurological, or psychogenic)
- Treatment follows a stepwise protocol: lifestyle → oral PDE5 inhibitors → vacuum device → penile injections → penile implant
- Most men do not fail on tablets — they fail to take them correctly. Sildenafil needs to be taken on an empty stomach, with sexual stimulation, and at an adequate dose
- Daily low-dose tadalafil (2.5–5 mg) often works better than on-demand dosing for men with moderate ED, particularly those with BPH or after prostate surgery
- Testosterone must always be checked — low testosterone reduces the effectiveness of PDE5 inhibitors until corrected
- ED is a cardiovascular warning sign. Every man with new-onset ED should have blood pressure, lipid profile, HbA1c, and cardiac risk assessment before treatment
Step 1: Find the Cause Before Prescribing Anything
Before I reach for the prescription pad, every new ED patient receives a structured evaluation. This is usually a single appointment, but it answers the questions that determine every subsequent decision.
The history questions that matter
- Onset — gradual or sudden? Gradual onset typically indicates a vascular or hormonal cause. Sudden onset, especially with normal morning erections, often points to a psychogenic component
- Morning erections — still occurring? Preserved nocturnal and morning erections are the single strongest indicator that the physical machinery is intact, and a psychogenic cause is likely. Loss of morning erections suggests an organic cause
- Performance with different partners or during masturbation? If erections are normal in one context but not another, psychogenic factors dominate
- Risk factors — diabetes, hypertension, smoking, high cholesterol, obesity, prior pelvic surgery or radiation, low mood, medication list
- Symptoms of low testosterone — fatigue, low libido, mood changes, loss of morning erections, reduced shaving frequency
Investigations
- Fasting blood tests — testosterone (measured between 7 and 11 am), SHBG, LH, prolactin, TSH, HbA1c, fasting lipids, full blood count, creatinine and eGFR
- Blood pressure measurement — ideally home readings over a week
- Cardiovascular risk calculation — using the ASCVD Risk Estimator or QRISK3 or a similar validated tool. ED without risk stratification is incomplete care
- Penile Doppler ultrasound — in selected men, particularly young men with vascular risk factors or suspected arteriogenic or venogenic ED
Step 2: Lifestyle (The Foundation Everyone Skips)
Every ED treatment protocol must begin here, because every downstream intervention works better when these foundations are in place. A sildenafil tablet in a smoker with untreated hypertension and a 105 cm waist (about 41 inches) is swimming against the tide.
- Stop smoking. Smoking directly damages the endothelium of the penile arteries. Stopping improves erectile function measurably within months
- Weight loss. A Mediterranean-style diet and regular exercise improve erectile function independent of weight, but weight loss amplifies the effect [4]
- Aerobic exercise. 150 minutes per week of moderate-intensity exercise improves endothelial function. This is not optional — it is therapeutic
- Sleep. 7 to 8 hours of quality sleep supports testosterone production and cardiovascular recovery. Obstructive sleep apnea should be specifically screened for
- Alcohol moderation. Chronic heavy drinking suppresses testosterone and damages nerves
- Reduce pornography use in younger men, particularly if partnered sex is struggling while masturbation is preserved. This pattern is increasingly common and reversible with structured abstinence
I give every patient a 12-week lifestyle target before or alongside starting medication. Results are measurable — and self-reinforcing — within 6 to 8 weeks.
Step 3: PDE5 Inhibitors (The First-Line Medication)
Phosphodiesterase type-5 (PDE5) inhibitors — sildenafil, tadalafil, vardenafil, and avanafil — are the first-line medical treatment for ED and the correct starting point for the overwhelming majority of men. They work by enhancing the nitric oxide pathway that dilates the penile arteries during sexual stimulation. They do not produce erections by themselves — they require sexual arousal to work.
| Medication | Onset | Duration | Key Note |
|---|---|---|---|
| Sildenafil (Viagra) | 30–60 min | 4–6 hours | Must take on empty stomach — fatty meal delays and weakens effect |
| Tadalafil (Cialis) | 30 min | 24–36 hours | Food-independent. Daily low-dose option available |
| Vardenafil (Levitra) | 30 min | 4–5 hours | Similar to sildenafil; better in some men with diabetes |
| Avanafil (Stendra) | 15–30 min | 6 hours | Fastest onset. Fewer visual side effects |
Why PDE5 inhibitors appear to “fail” (and actually do not)
Roughly 50–70% of men who are told “sildenafil did not work for me” have actually been taking it incorrectly. The common errors are:
- Taken with or after a heavy fatty meal — can delay onset by over an hour and halve the peak concentration
- Inadequate dose — starting at 25 mg and giving up, when 50 or 100 mg is needed
- No sexual stimulation — the tablet alone does not produce erections
- Insufficient trials — current guidance is to attempt at least 6 to 8 properly-dosed occasions before concluding failure [1]
- Untreated low testosterone — PDE5 inhibitor efficacy is reduced in hypogonadal men until testosterone is replaced [5]
Before escalating to second-line treatment, I always make sure the patient has had at least six attempts with maximum-tolerated doses of two different PDE5 inhibitors, on an empty stomach, with sexual arousal, and with testosterone optimized.
➡️ Related Read: Viagra, Cialis, and Sildenafil — The Complete Comparison GuideDaily low-dose tadalafil — an underused option
Instead of taking a tablet before sex, tadalafil 2.5 or 5 mg is taken every single day. This keeps the medication at a steady level in the bloodstream, meaning spontaneous sex is possible without timed dosing. It also improves urinary flow in men with BPH and improves endothelial function over time. For men with moderate ED, BPH, or after prostate surgery during penile rehabilitation, this is often my preferred prescription.
When PDE5 inhibitors are genuinely unsafe
- Current use of nitrates (nitroglycerin, isosorbide mononitrate) — absolute contraindication, can cause life-threatening hypotension
- Recent heart attack, unstable angina, or severe heart failure — cardiology clearance required
- Severe hepatic impairment or non-arteritic anterior ischemic optic neuropathy (NAION)
- Caution with alpha-blockers — use separated by several hours to reduce hypotension risk
Download Your Free Clinical Action Plan
Enter your email below to download Dr. Khalid’s complete Evidence-Based ED Action Plan as a free, printable PDF.
Step 4: Testosterone Optimization (Run in Parallel)
A morning total testosterone level (measured between 7 and 11 am, ideally on two separate days) is essential before or early in the treatment pathway. Low testosterone does two things that matter here:
- It reduces libido, contributing directly to reduced erections
- It reduces the efficacy of PDE5 inhibitors, so tablets that “should” work often do not
In hypogonadal men (total testosterone typically under 8–12 nmol/L (about 230–350 ng/dL) with relevant symptoms), testosterone replacement therapy (TRT) should be initiated with appropriate cardiovascular and prostate risk assessment [6]. Testosterone alone rarely fixes ED in isolation, but it restores the baseline physiology that lets other treatments work.
➡️ Related Read: Low Testosterone in Men Over 40 — Signs Your Doctor Might MissStep 5: Vacuum Erection Device (Often Underrated)
A vacuum erection device (VED) is a simple mechanical pump that draws blood into the penis, with a constriction ring slipped onto the base to maintain the erection. It is drug-free, carries virtually no systemic risk, and produces a functional erection in the great majority of men.
I often recommend it in these scenarios:
- PDE5 inhibitors not tolerated or contraindicated (e.g. nitrate users)
- Part of penile rehabilitation after radical prostatectomy — daily use from 2 to 4 weeks post-surgery improves long-term function and preserves penile length
- Older patients who prefer a non-pharmacological approach
The erection feels different — the penis is cooler and hinged at the base rather than rigid throughout — but it is functionally adequate for intercourse, and many patients come to prefer it after experience.
Step 6: Intracavernosal Injections (When Tablets Fail)
When lifestyle, maximum-dose PDE5 inhibitors, and testosterone optimization are not enough, the next step is intracavernosal injection therapy. A small dose of alprostadil (Caverject, Edex) or a compounded Trimix (alprostadil + papaverine + phentolamine) is injected into the side of the penis with a tiny insulin needle before intercourse.
The psychological barrier to injections is substantial, but the results are excellent. Response rates are around 85–90% even in men who have failed oral therapy [7]. The technique is quick, the needle is painless for most men after the first one or two attempts, and the erection is reliable.
I always teach the first dose in clinic with careful titration, and review for:
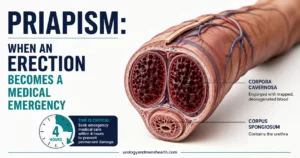
- Priapism — erection lasting over 4 hours is a medical emergency. Rare if dose is correctly titrated
- Penile pain — more common with alprostadil alone; often reduced with Trimix
- Bruising or fibrosis with long-term use — typically minor with proper technique
Step 7: Penile Implant (The Definitive Solution)
Penile prosthesis implantation is reserved for men who have failed or cannot use all less invasive options. An inflatable three-piece prosthesis is surgically implanted into the corpora cavernosa, with a reservoir in the abdomen and a pump in the scrotum. The man controls the erection by squeezing the pump.
Despite being a surgical option, the outcomes are genuinely impressive:
- Patient satisfaction rates above 90% — the highest of any ED treatment [8]
- Reliable, on-demand erections that last as long as wanted
- No further medications, devices, or injections required
- Complication rates have fallen steadily — modern infection rates are under 2% with coated devices
The biggest limitation is irreversibility — the erectile tissue is damaged during implantation, so removal without replacement will leave permanent ED. For men who have exhausted other options, however, it is transformative.
A Note on Shockwave Therapy
Low-intensity extracorporeal shockwave therapy (Li-ESWT) has received significant marketing attention. The evidence is genuinely mixed. Some studies in men with mild-to-moderate vasculogenic ED show modest improvement in erectile function scores, with the effect mediated by improved endothelial function and possibly new vessel formation [9]. Other trials show no clinically meaningful benefit.
My honest position: it is not a scam, but it is also not a miracle. For men with mild vascular ED who are PDE5 responders looking for an adjunct, it is a reasonable option to discuss. It is not appropriate as a first-line treatment, and it should not be marketed as a cure. Be wary of expensive “packages” offered by clinics that do not proceed via stepwise evaluation.
💡 In My Practice
The single most useful thing I tell men in their first ED consultation is that sildenafil needs to be taken on an empty stomach. An astonishing number of patients I see have been taking it after dinner for months, concluding it does not work. A heavy meal, particularly a fatty one, can delay absorption by over an hour and dramatically reduce peak concentration. The fix is often as simple as shifting the timing — take the tablet an hour before a light meal, not with or after a heavy one.
I have a low threshold for ordering a morning testosterone level. Low testosterone is under-diagnosed in men of South Asian descent in our region, partly because symptoms like fatigue and low libido are often dismissed as stress or aging. When the testosterone comes back at 7 or 8 nmol/L (around 200–230 ng/dL) and the man has been on sildenafil for a year without benefit, the conversation changes completely. Replace the testosterone first, and often the sildenafil begins to work.
The psychogenic component is more common than most patients — and doctors — acknowledge. When a young man tells me his erections are excellent during masturbation and absent with his partner, I do not order a penile Doppler. I ask careful questions about anxiety, relationship pressures, and sometimes pornography use. The treatment for this pattern is behavioral, relational, and sometimes psychological — not pharmacological. A prescription would be a disservice.
I also strongly believe in daily low-dose tadalafil for men with moderate ED, BPH, or early diabetes. Taking 5 mg every evening transforms the experience of sex from something that needs to be planned around a tablet to something spontaneous again. Many men who bounced between different on-demand medications for years have their quality of life restored by simply switching to daily dosing.
Finally — the single most important thing I tell every new ED patient is that this is not just about sex. Erectile dysfunction is a vascular event happening in a small artery, and it often predicts a larger vascular event in the heart within 3 to 5 years. Blood pressure, cholesterol, glucose, and smoking all need addressing. Fix the cardiovascular picture and you often fix the erection in the process. Miss the cardiovascular picture and you are treating a symptom while the disease progresses.
When to See a Urologist Promptly
Most ED can wait for a routine appointment. A small subset of presentations cannot. Five patterns warrant urgent assessment rather than a primary-care prescription.
⚠️ When to See a Urologist Promptly
- Sudden onset ED in a previously well man — deserves a full cardiovascular workup, not reassurance
- ED with chest pain, breathlessness, or exertional symptoms — see a doctor urgently; cardiac clearance is essential before PDE5 inhibitors
- Erection lasting more than 4 hours (priapism) — this is a urological emergency. Go to the emergency room (ER) immediately; delay over 6 hours risks permanent damage
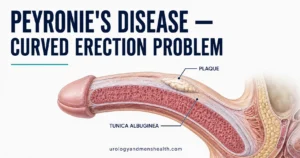
- ED after pelvic trauma or with penile curvature — structural causes (Peyronie’s disease, venous leak) need specific assessment
- ED with neurological symptoms (numbness, weakness, new bowel or bladder dysfunction) — requires neurological evaluation for spinal cord or cauda equina pathology
Erectile Dysfunction Treatment: Frequently Asked Questions
How many times should I try sildenafil before deciding it doesn’t work?
Current evidence-based guidance recommends at least 6 to 8 properly-dosed attempts before concluding that a PDE5 inhibitor has failed. “Properly dosed” means empty stomach (for sildenafil), adequate dose (50 to 100 mg), sufficient time before intercourse, and with sexual stimulation. If the first three attempts fail, the issue is often technique rather than the medication itself. Before escalating, review the dose, timing, and whether testosterone has been checked. See our complete comparison of sildenafil, tadalafil, and vardenafil for dosing detail.
Is erectile dysfunction treatment permanent, or do I have to stay on medication forever?
It depends entirely on the cause. Psychogenic ED, ED from low testosterone, ED from medication side effects, and ED from controllable cardiovascular risk factors are all potentially reversible with treatment of the underlying cause. Long-standing vascular ED in a man with established diabetes and significant arterial disease is usually managed rather than cured — but managed well, sexual function can still be excellent. Very few cases are truly irreversible; most are “treatable, with the right treatment”. Read our guide to ED and cardiovascular risk to understand why fixing the underlying cause often fixes the erection.
Can I buy ED tablets online safely?
Sildenafil is available through regulated online pharmacies in the US, UK, and most Commonwealth countries after a brief health check. In principle, this is safe for healthy men without cardiovascular risk factors. However, bypassing a proper evaluation means missing the diagnosis of underlying cardiovascular disease or low testosterone, which is the real threat ED is signaling. For a first episode, see a primary care doctor or urologist properly — the investigations matter more than the prescription. Our low testosterone guide explains what to ask for at your first appointment.
Do supplements for erectile dysfunction work?
The evidence is mostly disappointing. L-arginine at high doses (3–5 g per day) has modest evidence for mild ED. Panax ginseng has weak supporting data. Most other supplements marketed for male sexual function have minimal or no evidence, and some have contained undisclosed prescription PDE5 inhibitors, which is genuinely dangerous for men on nitrates. Spend the money on a proper medical review rather than supplements. The stepwise erectile dysfunction treatment protocol in this article will deliver more value than any over-the-counter product.
I had a radical prostatectomy — will erectile dysfunction treatment still work for me?
Yes, usually, though the approach differs. After prostatectomy, penile rehabilitation starts early — typically daily low-dose tadalafil, vacuum device use, and sometimes early intracavernosal injections — specifically to preserve erectile tissue while the nerves recover, which can take 12 to 24 months. Starting this protocol early makes a significant difference to long-term recovery. If oral medications remain ineffective after 18 months of rehabilitation, injection therapy and penile implant are both highly effective options with excellent satisfaction rates in post-prostatectomy patients [10].
What is the success rate of penile implant surgery?
Patient satisfaction rates with modern three-piece inflatable penile prostheses are consistently above 90%, the highest of any ED treatment. Modern coated devices have reduced infection rates to under 2%, and revision surgery is uncommon when implantation is performed by a high-volume surgeon. The main considerations are irreversibility (the erectile tissue is altered during implantation) and cost. For men who have failed all less invasive options, the procedure is genuinely transformative — most patients in our practice report they wished they had pursued it sooner.
📚 References
- Burnett AL, Nehra A, Breau RH, et al. Erectile Dysfunction: AUA Guideline. American Urological Association. 2018 (amended 2023). AUA Guidelines
- European Association of Urology. EAU Guidelines on Sexual and Reproductive Health. EAU. 2024. EAU Guidelines
- Thompson IM, Tangen CM, Goodman PJ, et al. Erectile dysfunction and subsequent cardiovascular disease. JAMA. 2005;294(23):2996–3002. PubMed
- Esposito K, Giugliano F, Di Palo C, et al. Effect of lifestyle changes on erectile dysfunction in obese men: a randomized controlled trial. JAMA. 2004;291(24):2978–2984. PubMed
- Shabsigh R, Kaufman JM, Steidle C, Padma-Nathan H. Randomized study of testosterone gel as adjunctive therapy to sildenafil in hypogonadal men with erectile dysfunction who do not respond to sildenafil alone. J Urol. 2004;172(2):658–663. PubMed
- Mulhall JP, Trost LW, Brannigan RE, et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. American Urological Association. 2018. AUA Guidelines
- Linet OI, Ogrinc FG. Efficacy and safety of intracavernosal alprostadil in men with erectile dysfunction. N Engl J Med. 1996;334(14):873–877. PubMed
- Bernal RM, Henry GD. Contemporary patient satisfaction rates for three-piece inflatable penile prostheses. Adv Urol. 2012;2012:707321. PubMed
- Clavijo RI, Kohn TP, Kohn JR, Ramasamy R. Effects of Low-Intensity Extracorporeal Shockwave Therapy on Erectile Dysfunction: A Systematic Review and Meta-Analysis. J Sex Med. 2017;14(1):27–35. PubMed
- Salonia A, Burnett AL, Graefen M, et al. Prevention and management of postprostatectomy sexual dysfunctions. Part 2: recovery and preservation of erectile function, sexual desire, and orgasmic function. Eur Urol. 2012;62(2):273–286. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.