Peyronie’s Disease: Curved Erection Treatment Guide
The bend in your erection isn't a punishment for anything you did — it's a scar inside the penis that behaves like keloid tissue. Here's what actually changes the curve, and what's a waste of your money.

When a man notices his erection has developed a new bend, the first thing he usually does is panic in silence. Peyronie’s disease is the most common cause of that bend in men over 40, and I see it almost every week in my clinic. The condition involves scar tissue — a fibrous plaque — inside the penis that won’t stretch like normal tissue, so the shaft curves toward the plaque during erection. It can be painful, it can affect penetration, and it can make sex feel like a problem you are no longer in control of. The good news: most cases stabilise, several treatments genuinely work, and surgery, when needed, has a high satisfaction rate. The bad news: the internet is saturated with vitamin combinations and traction gimmicks that waste your time during the only window when real progress is possible.
Key Takeaways
- Peyronie’s disease is caused by fibrous plaque in the tunica albuginea — not a venereal infection, not “wear and tear,” and not your partner’s fault.
- The acute phase (first 12 months) is when curve and pain change; the chronic phase is when the curve stabilises and surgery becomes safe.
- Curvature under 30 degrees with no functional problem usually needs reassurance, not treatment.
- Xiaflex (collagenase) injections reduce curvature by an average of 17 degrees and are FDA-approved for curves of 30-90 degrees.
- Vitamin E, traction-only protocols, and most “Peyronie’s supplements” have no high-quality evidence — don’t waste the acute phase on them.
What Peyronie’s Disease Actually Is
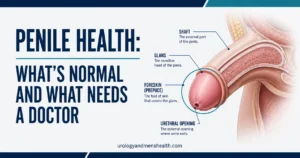
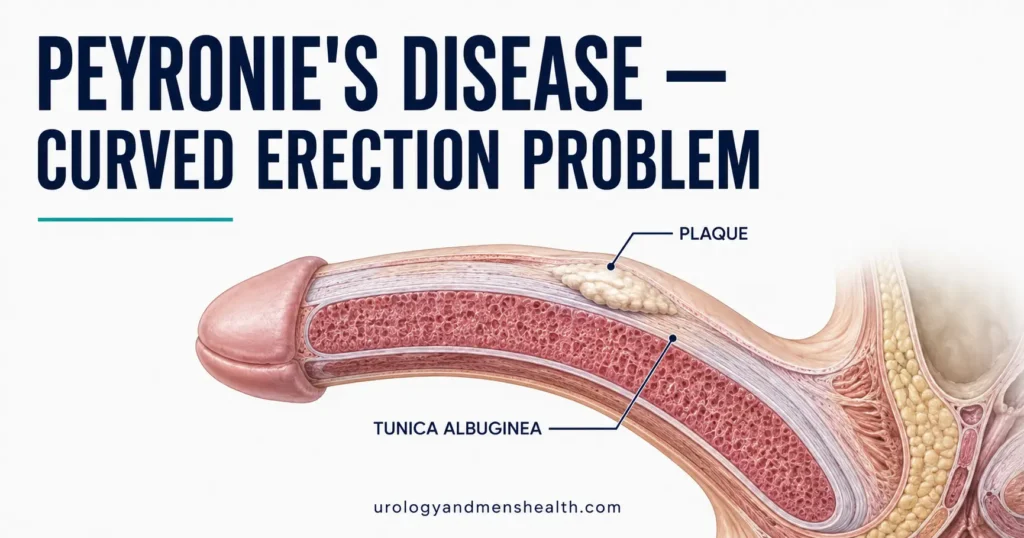
The penis isn’t a single solid structure. It contains two long erectile cylinders called the corpora cavernosa — sponge-like tissue that fills with blood during erection. Wrapping each corpus is a tough fibrous sheath called the tunica albuginea. Think of the tunica as a balloon casing: it stretches uniformly when the cylinders inflate, and that uniform stretch is what produces a straight erection.
In Peyronie’s disease, a localised area of the tunica is replaced by dense scar tissue — a plaque. That patch behaves like a keloid scar on your skin: it doesn’t stretch. So when the rest of the tunica expands during erection, the plaque pulls that segment short, and the penis bends toward it. If the plaque is on the top (dorsum), the erection curves upward; on the bottom (ventral), it curves downward; on the side, it curves left or right. Some men get an hourglass deformity, a hinge effect, or shortening without much obvious curve — all of those are also Peyronie’s.
This is a wound-healing problem, not a sexually transmitted condition. Current evidence suggests repeated micro-trauma during intercourse is the most likely trigger in a genetically susceptible man [1]. The body lays down scar tissue exactly where small tears occurred — but in some men, the scar matures into a thick, contractile, sometimes calcified plaque instead of resolving. For a clinical overview of related sexual health conditions, see our Sexual Health Hub.
Why It Happens — And Who Gets It
The honest answer is that we don’t have a single cause. Peyronie’s affects an estimated 3-9% of men, rising to over 10% in men in their sixties and seventies [2]. The risk factors I see clustering in patients are predictable:
- Age over 50 — tunica albuginea becomes less elastic with age, so micro-tears are more likely to leave a permanent scar.
- Diabetes — high blood sugar interferes with normal wound healing and is a strong independent risk factor.
- Erectile dysfunction — a softer erection bends more during intercourse, increasing micro-trauma risk. This is why treating co-existing ED is often the first step.
- Cardiovascular disease and hypertension — vascular health and penile health share the same biology. If you have a new bend plus weaker erections, the bend is usually not the only problem.
- Dupuytren’s contracture — a similar fibrotic condition in the palm. About 20% of Peyronie’s patients have it. If your dad or brother has the “claw hand,” your risk is real.
- Pelvic or penile injury — a remembered traumatic bend during sex (most patients can name the night it happened), pelvic fracture, or surgical instrumentation.
- Low testosterone — associated with worse outcomes, though not a direct cause. If you have symptoms, review our guide on low testosterone in men over 40.
None of this is your fault. I tell every new Peyronie’s patient the same thing in the first consultation: this is a wound-healing problem in tissue that wasn’t built to scar predictably, and you didn’t cause it by being too rough or too active. What you do have control over is the next 12 months — which is the window where intervention actually changes the trajectory.
Acute vs Chronic Phase — Why Timing Decides Treatment
Peyronie’s disease moves through two distinct phases, and confusing them is the single most common reason men get the wrong treatment.
Acute (active) phase — first 6 to 18 months
The plaque is still forming. The curve is still changing — usually getting worse. Erections are often painful, both with and without an erection. This is the phase where men panic and search the internet, because something is actively going wrong every week. Pain with erection in this phase is a useful clinical marker: it almost always resolves on its own within 12-18 months, even if you do nothing.
This is also the only phase where non-surgical treatment can change the final outcome. Once the plaque calcifies, no injection or device will reverse it.
Chronic (stable) phase — usually after 12 months
The curve has been stable for at least 3 to 6 months. The plaque has matured — often calcified, visible on ultrasound as a bright echo with a shadow behind it. Pain has resolved. The shape you have now is the shape you will have. This is when surgery becomes a genuine option, because operating on an unstable curve risks operating on the wrong angle entirely.
A 54-year-old engineer came to me four months after a sudden, painful bend during sex. He’d already spent £180 on a vitamin E and L-arginine stack from a “men’s health” website and was about to buy a £600 traction device. His curve was 35 degrees, painful, and changing week to week. We stopped the supplements, started intralesional verapamil and oral pentoxifylline, and put him on gentle stretching — no expensive device. Six months later his pain had gone, his curve had stabilised at 28 degrees, and he didn’t need surgery.
The lesson I want every Peyronie’s patient to take from this: the acute phase is short and precious, and the wrong intervention wastes it.
How Peyronie’s Disease Is Diagnosed
Diagnosis is mostly clinical. Bring photos of your erection from at least three angles — top-down, side, and front — taken at full erection. I cannot overstate how useful this is. Men routinely overestimate or underestimate their own curve, and a flaccid examination tells me nothing about the bend during intercourse.
In the office I will:
- Palpate the plaque — most plaques are felt as a firm cord or nodule along the shaft, usually on the dorsum.
- Measure stretched penile length — to give you a baseline against later shortening.
- Induce an erection in clinic with an intracavernosal injection of vasoactive medication, then measure the curve with a goniometer at peak rigidity. This is the gold-standard objective measurement.
- Perform penile Doppler ultrasound in selected cases — it shows plaque size, location, calcification, and whether your erectile blood flow is preserved. If you have a venous leak, that changes everything about which surgery is appropriate.
- Use the IIEF-5 questionnaire to quantify your erectile function alongside the curve. If your erections are weak, see our IIEF-5 erectile function self-assessment to bring a score to your urology appointment.
I rarely order MRI for Peyronie’s — it adds cost without changing management. Standard X-rays can detect heavy calcification but ultrasound does this better. There is no useful blood test for Peyronie’s disease itself; we test for diabetes, lipids, and testosterone because comorbidities affect outcomes.
What Actually Works — The Treatment Ladder
The American Urological Association 2024 guideline on Peyronie’s disease is the clearest summary of the evidence, and I follow it closely [3]. Here is the honest ladder, from least invasive to most.
1. Reassurance and observation
For a curve under 30 degrees that doesn’t interfere with intercourse, no treatment is the right treatment. The curve may improve a little on its own, will likely stabilise, and surgery has its own risks. About 13% of men experience spontaneous improvement; most do not get worse after the acute phase.
2. Oral medications
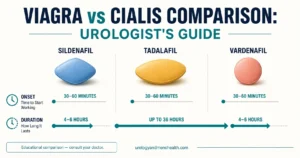
Pentoxifylline (400 mg three times daily) is the oral therapy with the most consistent supportive data — moderate, not dramatic. It is well tolerated and worth a trial during the acute phase. Daily low-dose tadalafil (5 mg) doesn’t reduce curve directly but improves erection quality and may protect against the micro-trauma cycle. Vitamin E, L-arginine, coenzyme Q10, colchicine, and most “Peyronie’s stack” supplements have failed every well-designed trial. Save your money.
3. Traction therapy and vacuum devices
Modern penile traction devices (worn 4-6 hours per day for several months) modestly reduce curvature and prevent shortening when used during the acute phase. They are tedious. Adherence is the limiting factor — men who actually wear them for 30 minutes a day get nothing; men who commit to 4+ hours daily get measurable benefit. Vacuum erection devices used 10 minutes a day appear to help similarly. Both work best combined with another active therapy, not as standalone treatments.
4. Intralesional injections
This is where evidence gets stronger:
- Collagenase clostridium histolyticum (Xiaflex) — FDA-approved for curves between 30 and 90 degrees. Administered as up to 4 cycles of 2 injections each, with modeling at home between cycles. Average curve reduction in the IMPRESS trials was about 17 degrees, or roughly 34% improvement [4]. Common side effects: bruising, swelling, mild pain. Rare but serious: corporal rupture. Expensive — typical total course in the US is $25,000-35,000, often partially insurance-covered with prior authorisation.
- Verapamil — calcium-channel blocker injected directly into the plaque every 2 weeks for 12 weeks. Less effective than Xiaflex but vastly cheaper. A reasonable option where Xiaflex isn’t available or affordable.
- Interferon alpha-2b — third-line, modest effect, mostly used in research centres.
5. Surgery
Reserved for stable, chronic-phase Peyronie’s with curvature severe enough to prevent intercourse — usually over 60 degrees, or with significant hinge effect, hourglass deformity, or co-existing erectile dysfunction. We will return to surgery in detail below.
Worried about a curved erection getting worse? Get the next-step protocol.
Enter your email below to receive Dr. Khalid’s complete Evidence-Based ED Action Plan as a free, printable PDF — covering ED workup, Peyronie’s overlap, and what to ask your urologist at your next visit.
Surgical Options for Peyronie’s Disease
The three operations a urologist considers depend on three variables: severity of curvature, baseline erectile function, and what trade-off the patient prefers — length versus straightness versus ED risk.
Plication (Nesbit and variants)
The surgeon places permanent sutures on the convex (longer) side of the erection, opposite the plaque, gathering tissue to straighten the shaft. Quick recovery, low complication rate, ED is almost never worsened. The trade-off: you lose length proportional to your curve — typically 1-2 cm for moderate bends, more for severe ones. Best for younger men with curves under 60 degrees and good erections, who would rather be shorter and straight than long and curved.
Plaque incision or excision with grafting
The surgeon makes a relaxing incision in or removes the plaque, then patches the defect with a graft (often porcine pericardium, bovine pericardium, or autologous tissue). Length is preserved. The risk: erectile dysfunction afterward, especially in men whose erections were borderline before — quoted rates range from 10-25% in the published series [5]. Best for severe curves with preserved erectile function.
Inflatable penile prosthesis (implant)
When Peyronie’s disease coexists with significant ED that has not responded to pills or injections, a three-piece inflatable penile prosthesis solves both problems in one operation. The surgeon can usually straighten the shaft manually at the time of implantation; severe curves may also require a relaxing incision. Patient satisfaction rates exceed 90% in dedicated series. This is the right operation for men in their fifties and sixties with a severe curve and unreliable erections — operating on the curve alone in that group sets them up for a second surgery they could have avoided.
The Sex Question — What Most Urologists Won’t Bring Up
Peyronie’s is a sexual condition, not a cosmetic one. The bend matters because of what it does to intercourse and intimacy, not because of how it looks. A few things I always raise with patients, because most won’t ask:
- Position changes solve a lot. Most men with curves under 45 degrees can have comfortable intercourse with positioning adjustments — woman-on-top or side-lying tend to be the most comfortable for dorsal curves. Push the conversation with your partner before you push for surgery.
- Erection quality affects how the curve presents. A soft-but-functional erection bends more, so improving rigidity with a PDE5 inhibitor often reduces the practical impact of the curve even without changing it.
- Mental health matters. Around half of Peyronie’s patients have measurable depression or anxiety related to the condition. Couples counselling and sex therapy referrals aren’t a luxury — for some men they are the most useful intervention I make.
- Don’t avoid sex during the acute phase. Avoidance worsens both the relationship and your erectile function long-term. If pain is the limiting factor, talk to your urologist about what is causing it specifically.
Peyronie’s overlaps significantly with vascular ED. If your bend has been accompanied by a slow decline in morning erections, see our guide on whether your ED is actually a heart warning, and consider that the link between cardiovascular health and erectile function is direct — see our overview of how high blood pressure silently damages the vascular system.
When to Get Seen Urgently
- Sudden severe bend with a pop or audible snap during sex — this is a possible penile fracture (tunica rupture). Go to the emergency room within hours, not days. It is surgically reparable but the window is short.
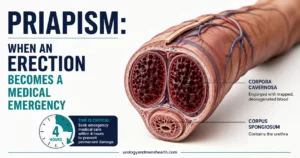
- Painful erection lasting more than 4 hours — priapism, unrelated to Peyronie’s but a separate emergency.
- New lump on the penis with rapid growth over weeks — Peyronie’s plaque grows slowly; rapid growth raises concern for other diagnoses including penile cancer.
- Curve worsening despite ongoing treatment after 12 months — return to your urologist for re-examination. Treatment plan needs to change.
Frequently Asked Questions
Can Peyronie’s disease go away on its own?
About 13% of men experience spontaneous improvement in curvature during the acute phase, but full resolution is uncommon. Most men’s curves stabilise rather than resolve. The realistic best-case for untreated mild Peyronie’s disease is a stable curve under 30 degrees with no functional problem — see our guide on treating erectile dysfunction if rigidity is also a concern, because weaker erections make existing curves more functionally limiting.
How long does the acute phase of Peyronie’s last?
The acute phase typically lasts 6 to 18 months. During this time the curve changes, the plaque forms, and erections are often painful. Pain resolves on its own within about 12 months in most men. Surgery should be deferred until the curve has been stable for at least 3 to 6 months — operating on an unstable curve risks operating on the wrong angle and needing a second procedure.
Do Xiaflex injections cure Peyronie’s disease?
Xiaflex (collagenase clostridium histolyticum) does not cure Peyronie’s disease — it reduces curvature. Average curve reduction across the IMPRESS trials was about 17 degrees, or roughly 34% improvement. Many men report meaningful improvement in sexual function, but a residual curve often remains. Xiaflex is FDA-approved for curves between 30 and 90 degrees in the chronic phase, and works best alongside daily modelling at home.
Will Peyronie’s disease cause erectile dysfunction?
Peyronie’s disease and erectile dysfunction overlap heavily — about half of Peyronie’s patients have measurable ED, and the two conditions share vascular and metabolic risk factors. The plaque itself can sometimes interfere with venous closure during erection, causing a soft-distal erection (rigid base, soft tip). If your erections are weaker as well as curved, vascular workup is part of the standard evaluation. Treating co-existing ED often improves the practical impact of the curve.
What’s the difference between Peyronie’s disease and a normal curved penis?
Most men have some natural curve to their erection, often slight and present since adolescence — this is congenital and not Peyronie’s disease. Peyronie’s is an acquired condition with a typical onset in middle age, a clearly palpable plaque in the tunica albuginea, often a remembered injury event, and progressive change over weeks to months. If the bend has been there since you became sexually active and isn’t changing, you have congenital curvature, not Peyronie’s, and you don’t need treatment unless it interferes with intercourse.
Does vitamin E really help with Peyronie’s disease?
No. Vitamin E was the first widely-used oral therapy for Peyronie’s and remains the most commonly self-prescribed — but every well-designed randomised trial has shown it performs no better than placebo. The same applies to L-arginine, coenzyme Q10, and most over-the-counter “Peyronie’s support” supplements. The 2024 AUA guideline does not recommend vitamin E for Peyronie’s disease. Spend the acute phase on therapies with real evidence: pentoxifylline, intralesional injection, traction with adherence, or daily tadalafil for co-existing ED.
References
- Devine CJ Jr, Somers KD, Jordan SG, Schlossberg SM. Proposal: trauma as the cause of the Peyronie’s lesion. Journal of Urology. 1997;157(1):285-290. PubMed
- Stuntz M, Perlaky A, des Vignes F, Kyriakides T, Glass D. The prevalence of Peyronie’s disease in the United States: a population-based study. PLOS One. 2016;11(2):e0150157. PubMed
- Nehra A, Alterowitz R, Culkin DJ, et al. Peyronie’s Disease: AUA Guideline. American Urological Association. 2024 update. AUA Guidelines
- Gelbard M, Goldstein I, Hellstrom WJG, et al. Clinical efficacy, safety, and tolerability of collagenase clostridium histolyticum for the treatment of Peyronie’s disease in 2 large double-blind randomized placebo controlled phase 3 studies (IMPRESS I and II). Journal of Urology. 2013;190(1):199-207. PubMed
- Hatzichristodoulou G, Osmonov D, Kübler H, Hellstrom WJG, Yafi FA. Contemporary review of grafting techniques for the surgical treatment of Peyronie’s disease. Sexual Medicine Reviews. 2017;5(4):544-552. PubMed
- European Association of Urology. Sexual and Reproductive Health Guidelines — Peyronie’s Disease section. EAU 2024. EAU Guidelines
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.