Vasectomy: What to Expect Before, During & After
Most men leave their vasectomy consultation thinking it's a 10-minute procedure with zero downside. The procedure is simple. The counseling, in my experience, is where things go wrong — and that's exactly what to expect from a vasectomy that nobody walks you through.

Most men book a vasectomy expecting a 10-minute procedure, a bag of frozen peas, and a weekend on the sofa. That part is largely true. What I find missing from most pre-op conversations is everything that comes after — the eight to twelve weeks before you can stop using contraception, the small but real risk of chronic scrotal pain, and the fact that “permanent” really does mean permanent. This guide on vasectomy what to expect covers every stage I walk my own patients through, from the consult through the final clearance test. For the bigger picture of male reproductive surgery, see our complete Sexual Health Hub.
Key Takeaways
- A vasectomy takes 10-20 minutes under local anesthesia and most men return to desk work within 2-3 days, but full clearance to stop other contraception takes 8-12 weeks confirmed by semen analysis.
- The no-scalpel technique uses a small puncture (around 10 mm / 0.4 inch) and has roughly half the bleeding and infection rate of the conventional incision approach — ask specifically which technique your urologist uses.
- Failure rate after confirmed clearance is approximately 1 in 2,000 from late recanalization — lower than tubal sterilization but not zero.
- Post-vasectomy pain syndrome — chronic scrotal pain lasting beyond 3 months — affects 1-2% of men and is the single most under-discussed risk during consent.
- Treat vasectomy as permanent at the time of decision. Reversal is technically possible but expensive (around $7,000-$15,000 in the US), often not covered by insurance, and pregnancy success drops sharply after 10 years.
What a Vasectomy Actually Is (and Isn’t)
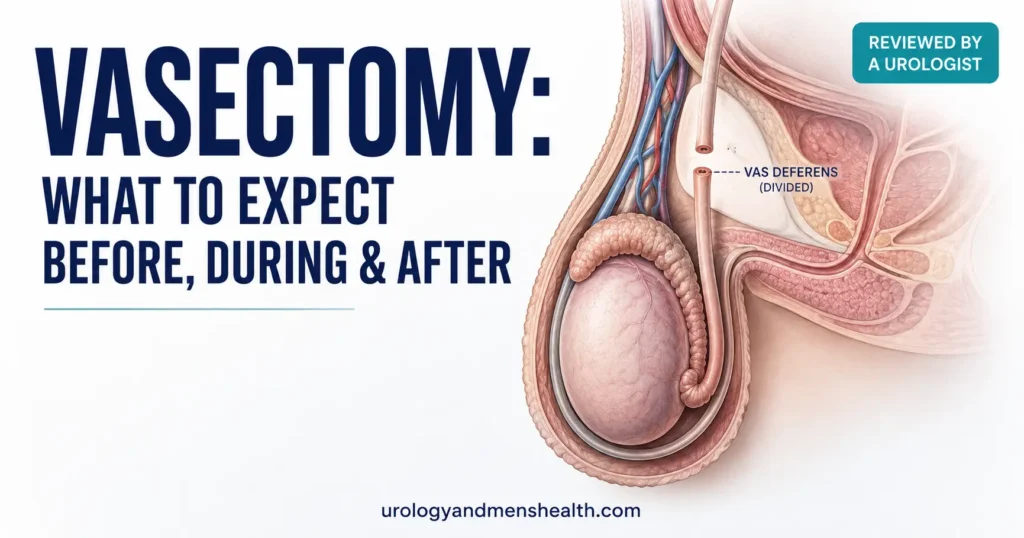
A vasectomy divides the vas deferens — the muscular tube that carries sperm from each testicle into the ejaculatory ducts. There are two of them, one on each side. Cutting and sealing both stops sperm from reaching the semen. That’s the entire mechanism.
Here is what changes after a successful vasectomy: nothing visible to you or to a partner. Testosterone production happens inside the testicle and travels through the bloodstream, not through the vas. Erections, libido, orgasm, ejaculate volume, and sensation all stay the same. Sperm makes up only about 2-5% of ejaculate volume — the rest comes from the seminal vesicles and prostate, which are untouched.
Here is what does not change immediately: your fertility. The vas downstream of the cut still contains millions of motile sperm. It takes 20-30 ejaculations and roughly 8-12 weeks to clear them [1]. Until a semen analysis confirms zero sperm, you can absolutely still cause a pregnancy. This is the single biggest reason vasectomies appear to “fail” — they don’t fail, the couple just stopped using contraception too early.
No-Scalpel vs Conventional Technique: Which One You Should Ask For
There are two ways to access the vas deferens through the scrotum, and the difference matters more than most patients realize.
The conventional incision technique uses one or two small cuts (about 1 cm / 0.4 inch) on each side of the scrotum, made with a scalpel. The vas is brought up through the cut, divided, sealed, and the skin is closed with absorbable sutures.
The no-scalpel vasectomy (NSV) uses a sharp pointed forceps to make a single tiny puncture in the scrotal midline — no blade, no sutures, and the opening usually closes itself. The vas is then isolated and divided through the same puncture. The 2012 AUA vasectomy guideline (reaffirmed and amended through 2023) recommends NSV as the preferred technique because it produces roughly half the rate of bleeding, hematoma, and infection compared with conventional incision [2].
What to ask before booking: “Are you performing a no-scalpel vasectomy, and what method are you using to occlude the vas?” The two best occlusion methods, per the same guideline, are mucosal cautery with fascial interposition or open-ended technique with cautery and clips. If your surgeon just ties the cut ends with suture — without cautery — failure rates climb noticeably. This is a fair, specific question and any urologist worth seeing will answer it directly.
The Procedure Itself: A Realistic Walkthrough
You arrive at the clinic. There is no general anesthesia, no IV, no fasting. You change into a gown, lie back, and the scrotum is shaved and cleaned with antiseptic. Local anesthetic — usually 2% lignocaine — is injected into the scrotal skin and around each vas. The injection is the only sharp sensation you’ll feel, and it lasts about 5 seconds per side.
Once the area is numb, the urologist palpates each vas through the scrotal skin, fixes it under a ring clamp, opens the skin (puncture or incision), brings the vas up, divides it, seals both ends (typically by cauterizing the lumen and placing the cut ends in different tissue layers), and returns the vas to the scrotum. Same on the other side. Total operating time: 10-20 minutes for an experienced urologist.
You’ll feel pressure and tugging — that’s normal and expected. Sharp pain is not. If you feel anything sharp during the procedure, tell the surgeon and they’ll top up the local. After about 30 minutes of observation, you can walk out and go home (someone else should drive). You’ll go home with supportive underwear, an ice pack, and oral analgesics — usually paracetamol/acetaminophen with ibuprofen, no opioids needed in most cases.
A patient came back to clinic a week after his vasectomy convinced the surgery had “given him erectile problems.” When we talked through it, what had actually happened was straightforward: he’d been so anxious about the procedure that he’d skipped sleep, drunk too much coffee, and had one disappointing attempt three days post-op while still tender. That snowballed into performance anxiety. By the time I saw him at the four-week check, with normal rest and reassurance, his erections were back to baseline.
Vasectomy does not cause erectile dysfunction. But anxiety and pain absolutely do, and they often masquerade as a “side effect of the surgery” — which is why the pre-op conversation should explicitly cover this.
Recovery Day by Day: What Normal Actually Looks Like
Recovery from a vasectomy is more predictable than almost any other urological procedure, but it’s not zero downtime. Here’s what I tell my patients to plan for.
- Day 0 (procedure day): Strict rest. Ice pack on the scrotum for 20 minutes on, 20 minutes off, for the first 4-6 hours. Supportive snug underwear or a scrotal support — not loose boxers. Take paracetamol 1 g every 6 hours plus ibuprofen 400 mg every 8 hours unless contraindicated.
- Days 1-2: Peak swelling and bruising. Continue scrotal support and ice. Walk around the house, but no lifting anything heavier than a kettle. A small amount of blood spotting on the dressing is normal.
- Days 3-7: Most men return to desk-based work by day 3. Avoid the gym, running, cycling, and any heavy lifting. Showers are fine; avoid soaking the wound in a bath for one week.
- Week 2: Sexual activity can usually resume. Ejaculation may feel slightly tender for the first one or two times — this settles quickly. Vigorous exercise can usually resume from day 10-14.
- Weeks 8-12: First post-vasectomy semen analysis. Until this confirms zero sperm, keep using your previous contraception. This is non-negotiable.
Normal post-op findings that often worry patients but don’t worry me: mild bruising spreading down the scrotum or onto the upper thigh (gravity, not bleeding); a pea-sized firm lump at the vas site that is tender for a few weeks (granuloma — usually settles); and yellowish bruising for up to three weeks. For broader recovery principles after urological surgery, see our pillar on male sexual and reproductive health.
The Semen Analysis — Why 12 Weeks Is the Magic Number
This is the step most likely to be skipped, and the step that determines whether the vasectomy actually worked for you.
The AUA recommends one post-vasectomy semen analysis (PVSA) at 8-16 weeks after the procedure [2]. Some surgeons request two. The reason for the delay is biology, not bureaucracy: the vas deferens downstream of the cut contains a reservoir of mature, motile sperm. Studies consistently show that roughly 1 in 5 men still have motile sperm at 6 weeks, and a small number still have sperm at 12 weeks [1]. Clearing this reservoir requires both time and ejaculation — typically 20 or more.
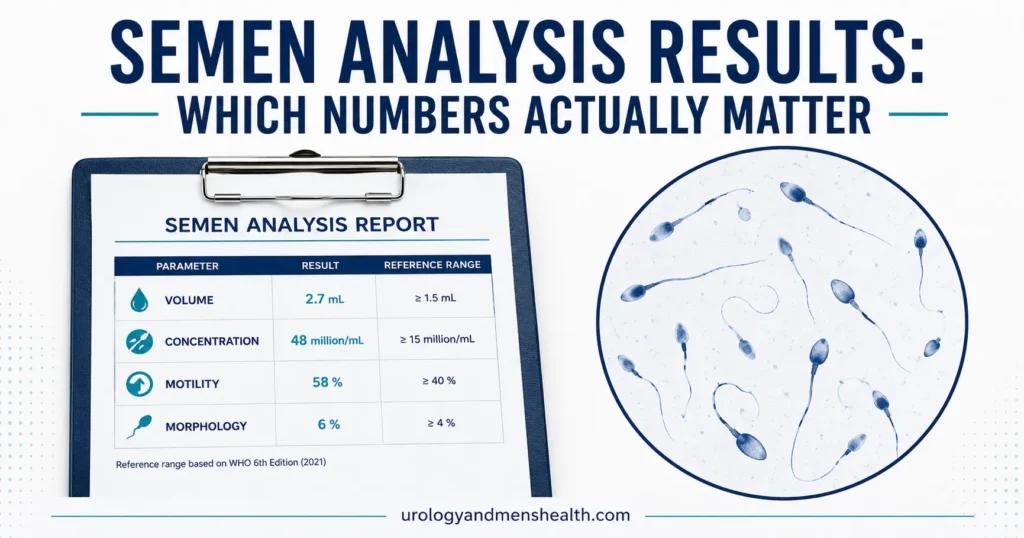
The accepted criterion for “success” is either azoospermia (zero sperm seen) or rare non-motile sperm at less than 100,000 per mL — also called RNMS. RNMS is not a failure; it represents debris-like immotile sperm fragments that can’t cause pregnancy. Persistent motile sperm at 6 months, however, suggests recanalization and the procedure has not worked.
If you understand what your result means and why it matters, our Semen Analysis Interpreter tool walks through each parameter in plain English — including how to read a post-vasectomy result. Use it alongside the lab report your urologist provides.
⚠ Do Not Stop Contraception Until You Have a Clearance Letter
Every “vasectomy baby” I’ve encountered in clinic came from a couple who stopped using contraception based on time elapsed rather than a laboratory result. A urologist’s clearance letter — based on a confirmed PVSA — is the only safe trigger to stop. Until then, your fertility is unchanged.
Failure, Recanalization, and the “1 in 2,000” Number
Vasectomy is the most effective form of male contraception, but it is not 100% effective forever. The two failure modes are different problems with different timelines.
Early failure means the surgery didn’t fully occlude the vas, or the man stopped contraception before clearance. Rate: roughly 1 in 100 procedures, and almost entirely preventable by a confirmed PVSA [2].
Late recanalization means a microscopic channel reforms between the two cut ends of the vas — sometimes months or years after a confirmed clearance. The cited rate is approximately 1 in 2,000 procedures over a lifetime [3]. For comparison, that is roughly half the long-term failure rate of female tubal sterilization. It’s small, but it’s not zero, and any urologist who tells you “100% guaranteed” is overselling.
The practical implication: if a previously confirmed-cleared man’s partner becomes pregnant years later, the right next step is a fresh semen analysis before assuming infidelity or making any other accusation. I’ve had this conversation more than once. It is rare but real.
Thinking about a vasectomy — or about reversing one?
Enter your email below to receive Dr. Khalid’s complete Evidence-Based ED & Sexual Health Action Plan as a free, printable PDF — including the questions to ask before signing any urological consent form.
Post-Vasectomy Pain Syndrome: The Risk Nobody Talks About
This is the conversation I make sure to have with every patient before signing a consent form, and it is the one most consultations skip.
Post-vasectomy pain syndrome (PVPS) is chronic, intermittent or constant scrotal pain that persists for at least 3 months after the procedure. The AUA-cited incidence is approximately 1-2% of men, with about 1 in 1,000 affected severely enough to seek further intervention [2]. The two main mechanisms are congestive epididymitis (back-pressure of sperm in the epididymis behind the divided vas) and chronic neuropathic pain (irritation of the small nerves around the vas).
What it feels like: a dull aching pain in one or both testicles, often worse after exercise, prolonged sitting, or ejaculation. Most men describe it as a 3-5 out of 10 baseline pain that flares to 7-8 occasionally.
Treatment, in stepwise order: anti-inflammatories and scrotal support; pelvic floor physiotherapy if there’s a muscle-tension component; spermatic cord block to confirm a neural cause; and as a last resort, microsurgical denervation of the spermatic cord or vasectomy reversal — which paradoxically relieves PVPS in roughly 50-70% of selected cases [4]. If you develop PVPS, ask your urologist whether to see a fellowship-trained microsurgeon within 6 months rather than waiting years.
For anyone reading this before their procedure: the 1-2% rate is not high, but it is real. If chronic pain elsewhere in your body would change your decision, factor this in. For broader context on chronic scrotal pain causes, our article on male reproductive anatomy and what can go wrong covers related conditions.
Is It Really Permanent? The Reversal Reality
Vasectomy reversal — vasovasostomy — exists. It works. But you should not have a vasectomy assuming reversal is a realistic backup plan.
The reasons: reversal is a microsurgical procedure performed under general anesthesia, lasting 3-5 hours, requires a fellowship-trained microsurgeon, and costs approximately $7,000-$15,000 in the US — often entirely out of pocket, since most insurers classify it as elective [5]. Success depends heavily on the obstructive interval — the time between vasectomy and attempted reversal. Patency rates (sperm returning to the ejaculate) are around 90% at under 3 years, but drop to roughly 70% at 10 years and 30-50% beyond 15 years [5]. Live-birth rates are always lower than patency rates because partner fertility, partner age, and sperm quality after reversal all matter.
The other option after vasectomy is surgical sperm retrieval (PESA or TESA) plus IVF/ICSI. This bypasses the vas entirely and is sometimes the better path when the female partner has fertility constraints of her own. It is also expensive (around $15,000-$25,000 per cycle in the US) and not always covered.
Practical advice: if you are under 30, in a new or uncertain relationship, or undecided about future children, I will usually advise waiting and discussing long-acting reversible contraception (LARC) for your partner instead, or condoms with periodic re-discussion. Vasectomy is the right answer when you and your partner are genuinely finished, not when you’re “probably” finished. If you’ve already had a vasectomy and want to reconsider, our future guide on vasectomy reversal decision-making walks through who is and isn’t a good candidate.
Vasectomy vs Female Sterilization vs Other Methods
Couples often compare vasectomy with female tubal sterilization (sometimes called “having your tubes tied” or laparoscopic salpingectomy). The differences matter both medically and ethically — this is a decision that affects two people.
Vasectomy is performed under local anesthesia, takes 15 minutes, has a 1-2 day major recovery, and carries a major complication rate of well under 1%. Female sterilization is performed under general anesthesia, takes 30-60 minutes, has a 5-7 day major recovery, and carries a roughly 5-10× higher rate of major complications because it is an intra-abdominal procedure [6]. The long-term failure rate of female sterilization is also higher (roughly 1 in 200 lifetime vs 1 in 2,000 for vasectomy after clearance).
On every clinical and economic metric, vasectomy is the lower-risk, lower-cost option. Yet female sterilization is performed several times more often in the US. That gap is not medical — it’s social.
The other comparison worth making is with a long-acting reversible IUD — particularly for couples who are “probably” but not certainly done. Modern hormonal IUDs are 99.8% effective, last 5-8 years, and are reversible. For some couples, an IUD plus a 2-year “are we sure?” period is the wiser sequencing than a permanent procedure done in a hurry. If you’re weighing reproductive options more broadly, our piece on how vascular health intersects with sexual function is also worth a read — many men considering vasectomy in their 40s and 50s have other circulatory factors that affect future erectile function.
If you have ED concerns separately from the vasectomy decision, our IIEF-5 self-assessment tool takes 2 minutes and gives you a validated severity score to bring to your urologist.
When to Call Your Urologist After the Procedure
⚠ Call Your Surgeon Same-Day If You Have:
- Scrotal swelling that becomes rapid, hard, or larger than a tennis ball — this can indicate a hematoma needing drainage
- Fever above 38°C / 100.4°F, or chills
- Increasing redness, warmth, or pus from the wound site after day 3 (signs of infection)
- Pain that is increasing rather than decreasing after day 5, or that is not controlled by paracetamol plus ibuprofen
- Blood-soaked dressings that need changing more than once
- Inability to urinate within 8 hours of the procedure
For each of these, the action is the same: call the practice number you were given at discharge, or attend the emergency room if you cannot reach your surgeon and the swelling or pain is severe. A scrotal hematoma drained early is straightforward; one ignored for 48 hours becomes a much bigger problem.
Frequently Asked Questions
Will a vasectomy change my sex drive, erections, or orgasms?
No. Testosterone production happens inside the testicle and travels through the bloodstream, not through the vas deferens — which is the only structure divided during the procedure. Libido, erection quality, orgasm sensation, and ejaculate volume all remain unchanged after a vasectomy. What can change temporarily is psychological comfort during sex if there’s pain or anxiety in the first 2-3 weeks. If you have separate concerns about erection quality, the IIEF-5 self-assessment is a useful starting point.
How long after a vasectomy can I have sex without contraception?
Not until your urologist gives you a clearance letter based on a post-vasectomy semen analysis showing either zero sperm or rare non-motile sperm under 100,000 per mL. That typically happens 8-12 weeks after the procedure and at least 20 ejaculations later. The “what to expect from a vasectomy” timeline most patients hear is misleadingly short — the surgery is fast, but clearance is not. Until you have written confirmation, your fertility is unchanged.
What is the realistic failure rate of a vasectomy?
After a confirmed clearance semen analysis, the late failure rate is approximately 1 in 2,000 procedures over a lifetime — caused by microscopic recanalization between the divided ends. Before clearance, the apparent failure rate is much higher, but this is almost entirely from couples stopping contraception too soon rather than the surgery itself failing. Compared with female tubal sterilization at roughly 1 in 200 long-term failure, vasectomy is the more reliable permanent option.
What is post-vasectomy pain syndrome, and how common is it?
Post-vasectomy pain syndrome is chronic scrotal pain lasting more than 3 months after the procedure, affecting approximately 1-2% of men. About 1 in 1,000 cases is severe enough to need specialist intervention. The pain comes from either congestive back-pressure in the epididymis or irritation of the small nerves around the divided vas. Treatment is stepwise — anti-inflammatories, pelvic floor physiotherapy, nerve blocks, and as a last resort microsurgical denervation or reversal. If you develop persistent pain, ask your urologist for a referral to a fellowship-trained microsurgeon within 6 months.
Is no-scalpel vasectomy actually better than the conventional technique?
Yes, on every measurable outcome. The no-scalpel vasectomy uses a small puncture instead of an incision and has roughly half the rate of bleeding, hematoma, and post-op infection compared with conventional incision technique. The 2012 AUA Vasectomy Guideline, reaffirmed through 2023, recommends NSV as the preferred approach. When you book your consultation, ask specifically: “Do you perform no-scalpel vasectomy, and do you occlude the vas with mucosal cautery and fascial interposition?” Both questions are appropriate and any urologist worth seeing will give you a clear answer.
Can a vasectomy be reversed, and how successful is reversal?
Yes, but you should not have a vasectomy assuming reversal is a realistic backup. Vasectomy reversal (vasovasostomy) is a microsurgical procedure costing approximately $7,000-$15,000 in the US, usually not covered by insurance. Sperm-return rates are around 90% if reversed within 3 years, dropping to 70% at 10 years and 30-50% beyond 15 years. Live-birth rates are always lower than sperm-return rates because partner fertility matters too. Decide on a vasectomy as if it is permanent, because for many men it functionally is.
References
- Griffin T, Tooher R, Nowakowski K, Lloyd M, Maddern G. How little is enough? The evidence for post-vasectomy testing. J Urol. 2005;174(1):29-36. PubMed
- Sharlip ID, Belker AM, Honig S, et al. Vasectomy: AUA guideline. American Urological Association. 2012, reaffirmed 2015, amended 2023. AUA
- Awsare NS, Krishnan J, Boustead GB, Hanbury DC, McNicholas TA. Complications of vasectomy. Ann R Coll Surg Engl. 2005;87(6):406-410. PubMed
- Tan WP, Levine LA. An overview of the management of post-vasectomy pain syndrome. Asian J Androl. 2016;18(3):332-337. PubMed
- Patel AP, Smith RP. Vasectomy reversal: a clinical update. Asian J Androl. 2016;18(3):365-371. PubMed
- Hendrix NW, Chauhan SP, Morrison JC. Sterilization and its consequences. Obstet Gynecol Surv. 1999;54(12):766-777. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.