Semen Analysis Results: Which Numbers Actually Matter
Most men leave the clinic with a semen analysis report and no idea which numbers actually predict fertility. I'll walk you through what each line means, which abnormal values change the plan, and which ones I tell patients to stop losing sleep over.

Your semen analysis results arrive as a single page of numbers with no context, and most men I see in clinic walk in convinced one bad value means they’re infertile. That’s almost never true. A semen analysis is a snapshot of a moving target — sperm production runs on a 74-day cycle, and a single abnormal report tells me far less than two reports three months apart. I’ll show you exactly which numbers matter, which ones the lab flags as “low” but I personally ignore, and what each parameter actually predicts about your chance of conceiving. For the full overview of fertility evaluation, see the Sexual Health Hub.
Key Takeaways
- WHO 2021 reference limits are the 5th percentile of fertile men — being “below normal” on one parameter does not mean infertile.
- Total motile sperm count (volume × concentration × progressive motility) predicts natural conception better than any single number on your report.
- One abnormal semen analysis means almost nothing. Two abnormal results 2-3 months apart is when I start a workup.
- Strict morphology below 4% is the most over-interpreted result on the report — alone, it rarely changes management.
- Azoospermia (zero sperm) needs a urologist referral, not a repeat test, and the FSH level determines whether it is obstructive or non-obstructive.
What a semen analysis actually measures
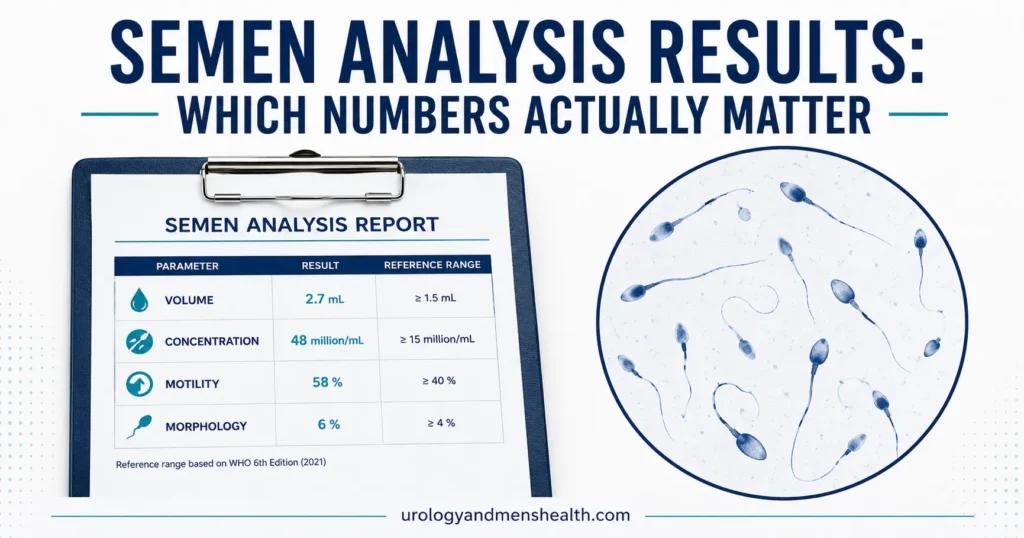
A standard semen analysis reports seven parameters from a single ejaculate collected after 2-7 days of abstinence. The lab measures volume (how much fluid), concentration (sperm per milliliter), total sperm count (volume × concentration), progressive motility (sperm swimming forward in a straight line), total motility (any movement), morphology (percentage with normal shape under strict criteria), and vitality (percentage alive). Each tells you a different piece of the picture.
The cutoffs your lab prints in bold red ink come from the WHO 2021 6th edition reference values — the most current global standard [1]. These are not “normal” values in the everyday sense. They are the 5th percentile of men whose partners conceived within 12 months of trying. In other words, 5% of fertile men fall below each cutoff. That single fact changes how I read every report.
The WHO 2021 reference values, line by line
Here are the lower reference limits from WHO 2021 [1], with a note on what each one actually tells me clinically:
Volume: 1.4 mL or more
That’s about a quarter teaspoon (1.4 mL = roughly 0.05 fl oz). Low volume on its own usually means a collection problem — partial sample lost, short abstinence period, or rarely a blocked or absent ejaculatory duct. If the volume is consistently under 1 mL across two samples, I look for retrograde ejaculation or anatomical obstruction.
Sperm concentration: 16 million per mL or more
This is where most men get worried. The old WHO 2010 cutoff was 15 million/mL; the 2021 update raised it to 16 million/mL based on a larger international fertile-men cohort. Concentration on its own is misleading. A man with 14 million/mL and 3 mL volume has a higher total count than a man with 20 million/mL and 1.5 mL volume.
Total sperm count: 39 million per ejaculate or more
This is the number I look at first. It captures both volume and concentration in a single value. Total count above 39 million is the reassuring zone. Between 5 and 39 million is “oligozoospermia” — reduced count, but plenty of men in this range conceive naturally. Below 5 million is severe oligozoospermia and gets a workup.
Progressive motility: 30% or more
Progressive means swimming forward in a roughly straight line. Sperm that wiggle in place don’t reach an egg. Below 30% progressive motility is “asthenozoospermia.” This is the parameter most affected by collection delays — a sample that sits at room temperature longer than 60 minutes before processing will show falsely low motility. I always ask the lab how long the sample sat before analysis.
Total motility: 42% or more
Total motility includes progressive plus non-progressive (twitching in place). Total motility is less useful clinically than progressive motility alone — non-progressive sperm don’t fertilize. I track progressive.
Morphology (strict criteria): 4% or more
This is the most over-interpreted result on the report. Even in highly fertile men, only about 4-15% of sperm have “perfectly normal” shape under strict Kruger criteria. Morphology below 4% in isolation — with normal count and motility — rarely changes how I manage a couple. The evidence linking isolated low morphology to reduced natural conception is weak [2].
Vitality: 54% or more alive
Only reported when total motility is very low. If most sperm are motionless, the lab checks whether they are immotile-but-alive (suggesting tail or structural defects) or immotile-and-dead (suggesting epididymal or environmental damage). Vitality changes the diagnostic path.
The single number that matters most: total motile count
If you take only one number from your report, take this one. Total motile sperm count (TMSC) = volume (mL) × concentration (million/mL) × progressive motility (%). It captures the three parameters that actually deliver sperm to the egg.
- TMSC above 20 million: natural conception is the expected outcome in the absence of female-factor problems.
- TMSC 5-20 million: natural conception is possible but slower. IUI (intrauterine insemination) becomes a reasonable next step if 12 months of trying haven’t worked.
- TMSC 1-5 million: natural conception unlikely. IUI may still work, but IVF with ICSI becomes the more efficient option.
- TMSC below 1 million: ICSI is almost always required.
Your lab report probably doesn’t calculate TMSC for you. Do it yourself, or use our Semen Analysis Interpreter to plug in your numbers and see where they fall.
In My Practice
A man in his early thirties came in last year terrified after a screening semen analysis his GP ordered showed “morphology 2%, concentration 14 million/mL.” His wife was already crying in the consult room. I calculated his TMSC: 2.8 mL × 14 × 38% progressive = 14.9 million motile sperm. Reassuring number. I repeated the test 10 weeks later after he cut alcohol, dropped 6 kg, and stopped the daily 40-minute hot bath. TMSC came back at 27 million. His wife was pregnant within four months.
The lesson I tell every patient: lab “below reference” flags are not infertility diagnoses, and lifestyle changes move the numbers faster than most men expect.
Sperm morphology: why I push back on isolated low results
Strict Kruger morphology evaluates each sperm head, midpiece, and tail under high magnification against rigid criteria. A sperm is counted “normal” only if every dimension and shape falls within tight bounds. Tolerances are tighter than what nature requires for fertilization. The result: even men with proven natural conception routinely score 4-10% normal forms.
A 2017 meta-analysis pooled studies looking at isolated teratozoospermia (low morphology, normal count, normal motility) and found no meaningful reduction in natural pregnancy rates compared with men with all-normal parameters [2]. AUA and ASRM 2021 joint guidelines on male infertility no longer treat isolated low morphology as an indication for assisted reproduction [3].
Where morphology does matter: when it is severely low (under 1%) and combined with other abnormalities, or when specific morphologic syndromes appear (globozoospermia, where every sperm has a round head and no acrosome). Those are distinct clinical entities and they do get IVF-ICSI referrals.
Worried your semen analysis means infertility? Get the next-step playbook
Enter your email below to receive Dr. Khalid’s complete Evidence-Based ED & Male Fertility Action Plan as a free, printable PDF — including a semen analysis interpretation checklist and the lifestyle interventions with the strongest evidence behind them.
When to repeat, when to refer
Sperm production runs on a roughly 74-day spermatogenesis cycle, plus another 10-14 days of epididymal maturation [3]. Anything that affected your testicles three months ago — a fever, a course of antibiotics, a heavy training block, a stressful work month — shows up in today’s report. That is why a single result rarely means what patients fear it means.
First semen analysis is abnormal: what to do
If your first analysis shows any parameter below the WHO 2021 cutoff, ask your doctor for a repeat test in 10-12 weeks, not sooner. A repeat at 4 weeks samples sperm produced during overlapping cycles — it will not give you a clean second data point. Use the 10-12 week gap to make any lifestyle changes you can (see the next section), so the repeat reflects your new baseline.
Two abnormal analyses: now we work it up
Two semen analyses showing the same pattern of abnormality, 10-12 weeks apart, is what AUA/ASRM 2021 define as the threshold for a formal male infertility workup [3]. That workup includes a urologist physical exam (scrotal exam for varicocele, testicular volume, vas deferens palpation), hormone panel (FSH, LH, total testosterone, prolactin), and sometimes scrotal ultrasound. For the bigger picture on what comes next, read our deep dive on male infertility causes and evaluation.
Azoospermia: don’t repeat, refer
If the report says azoospermia — zero sperm in the ejaculate after centrifugation — this is not the moment to wait three months and try again. Ask for an immediate urology referral and request an FSH level at the same time. FSH separates obstructive azoospermia (normal FSH, normal testicular volume — sperm production is fine but the pipe is blocked) from non-obstructive azoospermia (high FSH, smaller testes — sperm production itself is impaired). The two have very different treatment paths, including the possibility of surgical sperm retrieval for IVF.
Red Flags — Get a Urology Referral Within 2 Weeks
Don’t wait for a repeat semen analysis if any of these are present alongside your results:
- Azoospermia (zero sperm) on the report.
- Severe oligozoospermia — total sperm count under 5 million.
- A palpable scrotal mass, persistent testicular pain, or one testis noticeably smaller than the other.
- Loss of libido, erectile dysfunction, or breast tissue development alongside the abnormal result (suggests hormonal cause).
- History of undescended testis, testicular cancer treatment, chemotherapy, or pelvic radiation.
- Recurrent miscarriages (3 or more) — this needs DNA fragmentation testing, not just standard analysis.
Lifestyle changes that actually move the numbers
The 74-day cycle is a feature, not a bug. It means any change you make today shows up in a semen analysis 10-12 weeks from now. These are the interventions with the strongest evidence base — and the magnitudes are not small.
- Stop smoking. Smokers have roughly 13% lower sperm concentration and 17% lower total count than non-smokers in pooled analyses [4]. The effect reverses within 3-6 months of quitting.
- Cut scrotal heat exposure. Hot baths over 40°C (104°F), saunas more than twice a week, prolonged laptop-on-lap use, and tight underwear all raise scrotal temperature 1-2°C above the 33-34°C that spermatogenesis requires. Heat-induced drops in sperm count reverse in 8-12 weeks.
- Lose weight if BMI is above 30. Obesity is associated with lower total sperm count and higher rates of oligozoospermia, mediated by altered estrogen-to-testosterone ratios in adipose tissue. A 5-10% body weight loss measurably improves semen parameters in most men [5]. Read more on what GLP-1 drugs do to sperm parameters.
- Reduce alcohol. Daily heavy drinking (over 25 units/week) drops sperm count and motility. Moderate drinking (under 14 units/week) shows minimal impact in most studies. For wellness context across the lifestyle picture, see our Men’s Wellness Hub.
- Address sleep. Men sleeping under 6 hours per night have lower sperm motility than men sleeping 7-8 hours; men sleeping over 9 hours also do worse. The U-shape is real and the mechanism is hormonal.
- Stop or substitute testosterone replacement. Exogenous testosterone suppresses LH and FSH and is one of the most common causes of severe oligozoospermia or azoospermia I see in men under 40. If you are on TRT and want to conceive, talk to your doctor about switching to clomiphene or hCG. Read the full picture in TRT: what I tell patients before starting, and screen yourself first with our Low Testosterone Symptom Quiz.
After vasectomy: a different kind of semen analysis
The post-vasectomy semen analysis is not interpreted like a fertility evaluation. The goal here is the opposite — confirming the absence of sperm. Current AUA guidance considers a vasectomy successful when a single post-procedure sample at 8-16 weeks shows azoospermia, or shows only rare non-motile sperm (under 100,000 non-motile sperm per mL) [3]. Until you have that confirmation, you are not sterile. For what to expect from the procedure itself, see our guide on vasectomy: what no one tells you before.
Frequently asked questions about semen analysis results
How long should I abstain before a semen analysis?
The WHO 2021 standard is 2-7 days of abstinence before collection. Shorter than 2 days lowers volume and total count; longer than 7 days raises volume but reduces progressive motility because older sperm accumulate. I tell patients to aim for 3-4 days — enough to give a reliable sample without inflating the result with stale sperm. If you are repeating an analysis, match the abstinence period to the first sample so the two are comparable (plug your numbers into the interpreter here).
Why are my semen analysis results different from my last one?
Substantial variation between two semen analyses from the same man is normal, not abnormal. Sperm production is a 74-day cycle and any illness, fever, medication, training stress, or heat exposure in the preceding 3 months affects today’s sample. Even in healthy fertile men, within-individual coefficient of variation for sperm concentration runs around 25-30% sample-to-sample. This is exactly why a single analysis cannot diagnose infertility — only two analyses, 10-12 weeks apart, showing the same pattern.
My morphology is 2% — does that mean I’m infertile?
Almost certainly not, in isolation. Strict Kruger morphology is a tight criterion where even highly fertile men commonly score 4-10%. A 2017 meta-analysis showed isolated low morphology with normal count and motility does not meaningfully reduce natural conception rates. AUA/ASRM 2021 guidelines no longer treat isolated low morphology as an indication for IVF. Calculate your total motile sperm count instead — it predicts conception much better. See the bigger fertility picture in our male infertility evaluation guide.
Can supplements improve my semen analysis results?
The evidence is mixed and the effect sizes are small. A 2019 Cochrane review of antioxidant supplements in subfertile men found low-certainty evidence of modest improvements in pregnancy and live birth rates, but inconsistent effects on individual semen parameters. Zinc, CoQ10, L-carnitine, vitamin E, and selenium are the most-studied compounds. I generally suggest a basic male fertility multivitamin during the 3-month optimization window before a repeat analysis, but I tell patients not to expect dramatic changes — lifestyle moves the numbers more than pills do.
How accurate is a home semen analysis test kit?
Home kits (the ones that check sperm concentration via a phone app or color-strip reading) are reasonably accurate for screening — they correctly identify men with concentrations above or below the threshold around 75-85% of the time in validation studies. What they cannot do is measure motility, morphology, or volume accurately. A home test is fine as a first step if you want a yes/no on concentration. A clinical-grade lab analysis is still required before any treatment decision.
If my semen analysis is normal, am I definitely fertile?
A normal semen analysis means a normal sample on one day — it does not guarantee fertility. Sperm function tests (DNA fragmentation, acrosome reaction, hyaluronan binding) are not part of a standard analysis and can be abnormal in men with completely normal counts. If a couple has 12 months of unprotected intercourse without conception and the man’s standard analysis is normal, the next step is female-factor evaluation plus possibly a sperm DNA fragmentation test, particularly if there is recurrent miscarriage.
References
- World Health Organization. WHO laboratory manual for the examination and processing of human semen, 6th edition. Geneva: WHO; 2021. WHO
- Kohn TP, Kohn JR, Lamb DJ. Role of sperm morphology in deciding between various assisted reproduction technologies. Eur Urol Focus. 2018;4(3):311-313. PubMed
- Schlegel PN, Sigman M, Collura B, et al. Diagnosis and treatment of infertility in men: AUA/ASRM guideline part I & II. J Urol. 2021;205(1):36-43, 44-51. AUA
- Sharma R, Harlev A, Agarwal A, Esteves SC. Cigarette smoking and semen quality: a new meta-analysis examining the effect of the 2010 World Health Organization laboratory methods for the examination of human semen. Eur Urol. 2016;70(4):635-645. PubMed
- Sermondade N, Faure C, Fezeu L, et al. BMI in relation to sperm count: an updated systematic review and collaborative meta-analysis. Hum Reprod Update. 2013;19(3):221-231. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.