Why Viagra Stopped Working: A Urologist’s Next Steps
When a patient tells me Viagra has stopped working, I assume the drug is fine and something else has changed. Nine times out of ten, I'm right — and the fix isn't a stronger pill.

If your Viagra stopped working after months or years of doing exactly what you needed it to, the most likely explanation is not that the drug failed. In my clinic, when a man tells me sildenafil has stopped working, I assume the medication is doing its job and something else in his physiology has changed underneath it. That distinction matters because the wrong next step — usually a higher dose or a new prescription — fixes nothing if the real problem is a narrowing artery, falling testosterone, a new blood pressure medication, or a performance anxiety loop that the pill can no longer outrun. This guide walks through the six clinical reasons Viagra stops working, what to do about each one, and when the answer is not a pill at all. For the full overview of treatment pathways, see our complete Sexual Health Hub.
Key Takeaways
- Sildenafil rarely “stops working” — what usually changes is the underlying vascular, hormonal, or psychological state the pill was masking.
- The first check is always dose and technique: 100 mg taken on an empty stomach with adequate sexual stimulation is the real ceiling, and most men have never used it correctly.
- New-onset Viagra failure in a man under 60 is a cardiovascular warning sign until proven otherwise — vascular ED precedes a coronary event by an average of 3 to 5 years.
- If sildenafil truly fails at maximum dose, daily tadalafil 5 mg, intracavernosal injections, and penile prosthesis are the evidence-based step-up options — in that order for most men.
What “Viagra Stopped Working” Actually Means
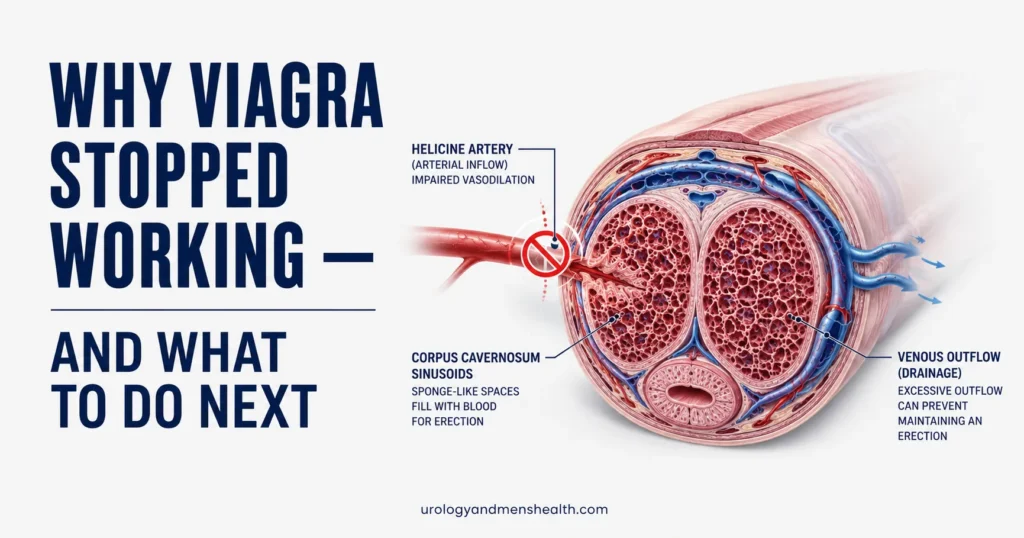
Sildenafil — the generic name for Viagra — does not produce an erection on its own. It is a PDE5 inhibitor, which means it blocks an enzyme called phosphodiesterase type 5. When you are sexually aroused, nerves in the penis release nitric oxide. Nitric oxide triggers the production of a signaling molecule called cGMP, which relaxes the smooth muscle in the penile arteries and lets blood fill the corpus cavernosum. PDE5 is the enzyme that breaks cGMP down. Sildenafil blocks that breakdown, so cGMP accumulates and the erection holds.
That mechanism has three failure points, and “the drug stopped working” is almost never one of them. Sildenafil itself does not lose effectiveness with repeated use — there is no tolerance phenomenon in pharmacology textbooks for PDE5 inhibitors. What can change is upstream: less nitric oxide release because the endothelium (the lining of blood vessels) is damaged; less arousal signal because testosterone has fallen or anxiety has taken over; or more arterial narrowing so that even with cGMP accumulating, not enough blood reaches the sinusoids. When men tell me Viagra has stopped working, they are usually describing one of these three upstream changes — not a failure of the pill.
Reason 1: You Were Never Taking It Correctly
This is the most common reason, and most men will not believe it applies to them. Sildenafil is fully effective only when three conditions are met: an adequate dose, an empty or near-empty stomach, and genuine sexual stimulation. The fact that you have used it before does not exempt you from these conditions — and the truth is most men have been getting away with a sloppy version of the protocol because their underlying physiology was forgiving. Once the physiology shifts, the technique starts to matter.
The dosing ceiling is 100 mg taken 60 minutes before sexual activity. A heavy or fatty meal can delay absorption by up to two hours and reduce peak plasma concentration by around 30 percent [1]. Alcohol — more than two standard drinks — blunts the response further. And sildenafil does not produce an erection without sexual stimulation; it is permissive, not generative. The pill clears the path; arousal still has to drive the car. Before assuming the drug has failed, the honest first step is to take a full 100 mg dose, on an empty stomach, with no more than one alcoholic drink, and with adequate partnered or solo sexual stimulation — and see what happens.
In My Practice
A 54-year-old patient came to me convinced his sildenafil had stopped working after three years. He was taking 50 mg with dinner, drinking two beers afterward, and trying to use the pill in bed an hour later while watching TV with his partner. We changed nothing about his prescription — only the protocol. 100 mg, empty stomach, no alcohol that evening, and a deliberate decision to engage rather than wait for the pill to do it for him. It worked on the first attempt. He did not have ED progression. He had drift in his technique that he had never noticed because his arteries had been compensating for him.
Before I escalate any man to a stronger drug or a more invasive treatment, I rule out the failure of basic protocol — because the cost of getting that wrong is years of unnecessary intervention.
Reason 2: Your Vascular Disease Has Progressed
This is the reason most men do not want to hear, and it is the one I look for hardest when sildenafil truly stops working. The penile arteries are small — roughly 1 to 2 mm in diameter, compared to 3 to 4 mm for coronary arteries and 5 to 7 mm for the carotids. Because they are smaller, atherosclerotic plaque narrows them sooner. A plaque deposit that would be invisible on a coronary scan can already be cutting penile blood flow in half.
The clinical implication is uncomfortable but well-established: vascular erectile dysfunction precedes a major cardiovascular event by an average of 3 to 5 years [2]. When a man in his 50s or 60s tells me his Viagra has stopped working, my first thought is not about his sex life — it is about his coronaries. The Princeton Consensus Panel, AUA, and EAU all now treat new-onset or worsening ED as a cardiovascular risk signal that requires evaluation, not just a quality-of-life complaint [3]. The questions I ask: any new chest tightness, breathlessness on stairs, leg cramps on walking, or unexplained fatigue? If the answer to any of these is yes, the workup is no longer a urology problem alone — it is a cardiology problem that happens to be presenting through the penis. To understand why morning erections are the cheapest vascular test you have, see why ED can be the earliest sign of heart disease.
If you want a structured estimate of your vascular ED risk before your appointment, run the ED Vascular Risk Screener and bring the printout to your urologist or primary care doctor. It does not replace a clinical exam, but it gives the conversation a starting point.
Reason 3: Your Testosterone Has Fallen
Sildenafil and testosterone work on different parts of the erectile pathway, and that is exactly why a man with falling testosterone often experiences his Viagra as “weaker.” Testosterone drives libido — the desire that initiates arousal and triggers nitric oxide release. Sildenafil only acts once that signal is already firing. If your testosterone has dropped, the signal upstream is quieter, less cGMP is being produced for the drug to protect, and the erection feels softer or harder to achieve even with the same dose.
The signs of falling testosterone in a man who was previously responding to sildenafil are specific: reduced morning erections (the most sensitive single sign), lower libido even when situational arousal is present, increased fatigue or low mood, loss of muscle mass despite unchanged activity, and reduced ejaculate volume. If three or more of these have shifted since your sildenafil started feeling less effective, total testosterone and free testosterone need to be measured — drawn before 10 a.m., on two separate occasions, per AUA guidelines [4]. Ask your doctor to include LH, FSH, and prolactin in the same panel; without those, you cannot tell whether the low testosterone is primary (testicular) or secondary (pituitary), and the treatment differs. The low testosterone signs urologists most often miss covers the diagnostic pathway in detail, and the Low Testosterone Symptom Quiz is a validated AMS-style instrument you can complete before your appointment.
Viagra not working the way it used to? Get the full clinical roadmap.
Enter your email below to receive Dr. Khalid’s complete Evidence-Based ED Action Plan as a free, printable PDF — the same step-by-step pathway I use in clinic when sildenafil starts to fail.
Reason 4: A New Medication Is Interfering
This is the easiest cause to miss because the timing connection is rarely obvious. A new blood pressure pill, an antidepressant, or a finasteride prescription starts in March; by July, sildenafil feels less effective; the man does not associate the two events because nothing changed on the day his Viagra stopped working. The pharmacology, however, is well documented.
The worst offenders in my clinic experience: beta-blockers (especially older ones like atenolol and metoprolol) blunt the sympathetic arousal pathway; thiazide diuretics like hydrochlorothiazide reduce penile blood flow at standard doses; SSRIs (sertraline, paroxetine, fluoxetine) reduce libido and ejaculatory function in 30 to 70 percent of men depending on the agent [5]; finasteride reduces dihydrotestosterone and is associated with persistent sexual dysfunction in a small but real subgroup. The fix is not always to stop the offending drug — sometimes the underlying condition matters more — but it is always worth asking your prescriber whether a same-class swap exists. ARBs like losartan and CCBs like amlodipine are usually neutral or even mildly protective for erectile function compared to beta-blockers and thiazides. Which BP medications cause ED and which are safer covers the specific swaps worth discussing with your doctor.
Reason 5: The Anxiety Loop Has Closed
The first time sildenafil produces a weaker erection than expected, something subtle happens. The next time, you are no longer thinking about your partner — you are watching your erection, waiting to see if the pill is going to work. That watchful self-monitoring is the single most reliable way to abolish an erection in a man with otherwise normal vascular function. It activates sympathetic outflow, which is the opposite of what an erection requires. Sildenafil cannot overcome it.
I see this most often in men in their 40s and 50s who had one bad experience — alcohol, stress, fatigue — and then unconsciously braced for failure on every subsequent attempt. The pill works fine pharmacologically; the brain is sabotaging the signal. The way out is not a stronger dose. It is to shift the prescription to a daily low-dose tadalafil regimen — typically 5 mg every morning. Daily tadalafil decouples the pill from the sexual encounter, removes the “did I time it right” anxiety, and provides a baseline level of PDE5 inhibition that lets spontaneous erections re-emerge. Within six to eight weeks, many men report not just better erections but a return of spontaneous morning erections — which is the clinical sign the loop has been broken.
Reason 6: There Is a Structural or Neurological Cause
A small group of men have a Viagra failure that is neither vascular, hormonal, nor psychological — it is anatomical. The two most common scenarios: prior pelvic surgery (radical prostatectomy, radical cystectomy, or extensive pelvic floor procedures) that damaged the cavernosal nerves; and Peyronie’s disease, where fibrous plaque in the tunica albuginea prevents the corpus cavernosum from expanding properly even when blood flow is normal. In these patients, sildenafil cannot rescue the erection because the downstream tissue is no longer capable of holding the response — the plumbing has changed.
The clues that point this way: ED that began abruptly after a specific surgery or injury, a palpable plaque or a new bend in the erect penis, or a complete absence of morning erections combined with absent response even to maximum-dose PDE5. This is the patient who needs to bypass the oral medication pathway entirely and move to intracavernosal injections, a vacuum erection device, or — if those fail — a penile prosthesis. The full ED treatment protocol walks through how each option is matched to the specific cause.
What Actually Comes Next: The Step-Up Pathway
Once the six reasons above have been worked through honestly and sildenafil truly does not produce an adequate erection at 100 mg with optimal conditions, there is a standard escalation pathway. It is not a guess. It is structured by AUA and EAU guidelines, and most men respond at one of the first two steps.
- Step 1 — Switch PDE5 inhibitor. Tadalafil at 20 mg on demand or 5 mg daily often works in men for whom sildenafil has failed. The pharmacokinetics differ: tadalafil has a 17.5-hour half-life versus sildenafil’s 4 hours, and it is less food-dependent. A side comparison of how Viagra, Cialis, and generic sildenafil differ helps choose the right one for your situation.
- Step 2 — Add vacuum erection device or behavioral therapy. If the cause has a psychological component, sex therapy combined with daily tadalafil has high success rates. The vacuum erection device is mechanical, drug-free, and works regardless of vascular status.
- Step 3 — Intracavernosal injections. Alprostadil or Trimix injected directly into the corpus cavernosum bypasses the entire upstream pathway. Success rates exceed 85 percent [6]. Most men who try injections after pills failed wish they had not waited.
- Step 4 — Penile prosthesis. A surgically implanted device, considered the definitive treatment for severe refractory ED. Patient satisfaction rates are among the highest of any urological procedure — around 90 percent [7].
When to Get Urgent Help
Some symptoms around Viagra use are not “treatment failure” — they are emergencies. Seek care immediately if you experience:
- An erection lasting more than 4 hours (priapism) — this is a urological emergency and can cause permanent tissue damage.
- Chest pain, severe shortness of breath, or fainting after a sildenafil dose.
- Sudden vision loss or a dark spot in your visual field — this can signal NAION, a rare but serious complication.
- Sudden hearing loss after a recent dose.
- New ED in a man under 40 with no clear cause — this needs a vascular workup, not just a stronger prescription.
How to Make the Next Appointment Count
The single most useful thing you can do before seeing a urologist about Viagra failure is to bring data. Three numbers shorten the consultation by half:
- An IIEF-5 score. This is a five-question validated instrument that quantifies your erectile function on a 5-to-25 scale. Complete the IIEF-5 ED self-assessment the morning of your appointment and bring the result. A score of 21 or below confirms ED; below 11 indicates severe ED.
- A morning erection log. For two weeks, note whether you woke with an erection. Frequency of morning erections is the cheapest test of vascular and neurological function we have.
- A current medication list. Every prescription started or changed in the past 12 months, with the start date. This catches the medication-interference cause faster than any test we can order.
Ask your urologist three specific questions: whether daily tadalafil 5 mg is appropriate as a next step before higher-tier treatments; whether a fasting lipid panel, HbA1c, and morning testosterone (with LH and prolactin) should be ordered; and whether any of your current prescriptions have a known erectile side effect that could be swapped for a same-class alternative. Those three questions, asked in that order, address the four highest-yield diagnostic and therapeutic decisions in this conversation.
Frequently Asked Questions
Can you build a tolerance to Viagra so it stops working?
No. There is no pharmacological tolerance mechanism documented for sildenafil or any other PDE5 inhibitor — the drug does not lose effectiveness with repeated use. When a man says his Viagra stopped working, what has almost always changed is the underlying condition the pill was treating: progressing vascular disease, falling testosterone, a new interacting medication, or a closed performance anxiety loop. The drug is doing the same job it did on day one; the physiology around it has shifted. Before assuming the medication has failed, confirm you are taking 100 mg on an empty stomach with adequate stimulation, then look upstream. The step-by-step ED treatment protocol covers what to check next.
If Viagra stopped working, will Cialis work better?
For many men, yes — and not because tadalafil is intrinsically stronger, but because its pharmacokinetics suit a different use pattern. Tadalafil has a 17.5-hour half-life versus sildenafil’s 4 hours, is less affected by food, and can be dosed daily at 5 mg to provide continuous low-level PDE5 inhibition. Daily tadalafil is particularly useful when performance anxiety is part of the failure, because it removes the timing pressure that comes with on-demand dosing. About 50 percent of men who failed sildenafil respond to tadalafil. The full side-by-side comparison is in Viagra, Cialis, and generic sildenafil compared.
Does Viagra failure mean I am going to have a heart attack?
It means your cardiovascular system deserves a closer look — not that an event is imminent. The penile arteries are smaller than coronary arteries, which is why vascular ED often appears 3 to 5 years before clinically significant coronary disease. That window is an opportunity, not a verdict. Men who address ED as a vascular warning — through blood pressure, lipid, glucose, and lifestyle optimization — substantially reduce their cardiovascular risk. Skipping the workup and only treating the ED is the costly mistake. If your sildenafil has weakened and you are over 40, ask your doctor for a fasting lipid panel, HbA1c, and a blood pressure check at minimum.
Is it safe to take a higher dose than 100 mg of Viagra?
No. 100 mg is the licensed maximum single dose for sildenafil, and doses above it do not improve erectile response — they only increase side effects, particularly headache, flushing, visual changes, and the risk of hypotension if combined with nitrates or alpha-blockers. If 100 mg is not producing an adequate erection under optimal conditions, the answer is not more sildenafil; the answer is a different mechanism. That usually means switching to tadalafil, adding behavioral or vascular treatment, or moving to second-line options like intracavernosal injections. The ED Vascular Risk Screener helps frame which pathway is most likely to succeed for your specific picture.
How long after Viagra fails should I wait before seeing a urologist?
If sildenafil has failed on three or more occasions despite correct use — 100 mg, empty stomach, no significant alcohol, adequate stimulation — book the appointment. Do not let it drift. Two things are happening when Viagra failure is left uninvestigated: the underlying cause (often vascular or hormonal) is progressing without treatment, and the performance anxiety loop is deepening. Both get harder to fix the longer they run. A urology appointment in the first three months after consistent failure usually resolves the situation with a medication change or a simple workup. Waiting twelve months frequently requires more invasive treatment.
References
- Nichols DJ, Muirhead GJ, Harness JA. Pharmacokinetics of sildenafil after single oral doses in healthy male subjects: absolute bioavailability, food effects and dose proportionality. Br J Clin Pharmacol. 2002;53 Suppl 1:5S-12S. PubMed
- Montorsi P, Ravagnani PM, Galli S, et al. Association between erectile dysfunction and coronary artery disease: matching the right target with the right test in the right patient. Eur Urol. 2006;50(4):721-731. PubMed
- Burnett AL, Nehra A, Breau RH, et al. Erectile Dysfunction: AUA Guideline. J Urol. 2018;200(3):633-641 (amended 2024). AUA Guideline
- Mulhall JP, Trost LW, Brannigan RE, et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J Urol. 2018;200(2):423-432. AUA Guideline
- Higgins A, Nash M, Lynch AM. Antidepressant-associated sexual dysfunction: impact, effects, and treatment. Drug Healthc Patient Saf. 2010;2:141-150. PubMed
- Belew D, Klaassen Z, Lewis RW. Intracavernosal injection for the diagnosis, evaluation, and treatment of erectile dysfunction: A review. Sex Med Rev. 2015;3(1):11-23. PubMed
- Bernal RM, Henry GD. Contemporary patient satisfaction rates for three-piece inflatable penile prostheses. Adv Urol. 2012;2012:707321. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.