Low Testosterone Symptoms Men Over 40: Signs Your Doctor Might Miss
Patients in their 40s who complain of fatigue and low drive are routinely handed antidepressants or told they are simply getting older. The truth is, while online clinics aggressively push testosterone for every tired guy, traditional doctors constantly miss severe, measurable hormonal deficiencies. This guide cuts through both extremes, showing you how to distinguish true hypogonadism from normal aging—and revealing what the TRT industry hides about the risks.

Low testosterone symptoms in men over 40 are simultaneously the most over-hyped and the most under-diagnosed problem I see in clinic. A 46-year-old man recently sat across from me. He’d been to his primary care doctor three times in two years — once for fatigue, once for low mood, once because his wife sent him about their “intimacy issues.” Each visit ended with a different answer: iron tablets, an antidepressant, a referral to a counselor. Nobody checked his testosterone. When I finally measured it, his total testosterone was 5.8 nmol/L (167 ng/dL) — less than half the lower limit of the reference range. He didn’t have depression. He had hypogonadism, and it had been missed for years.
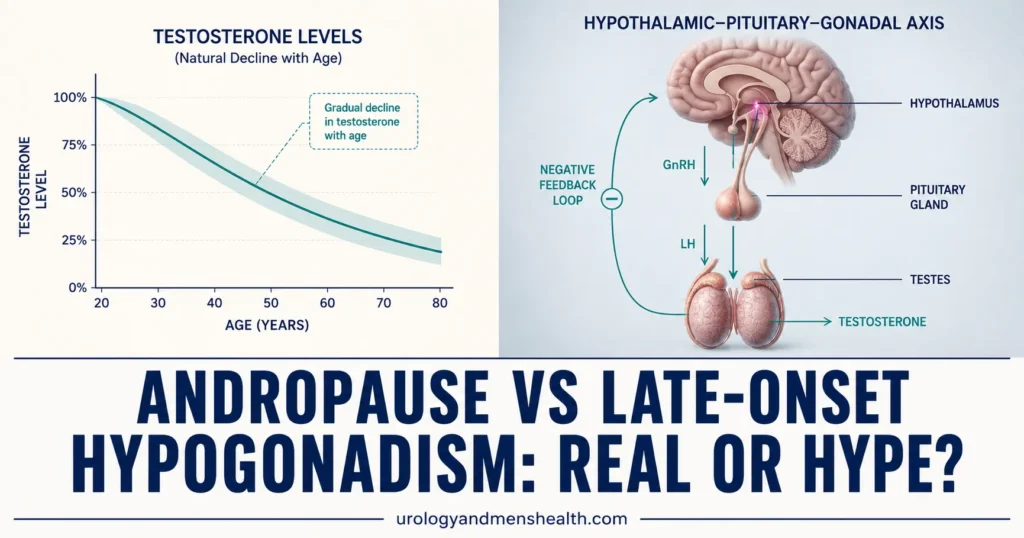
This story is not unusual. Online “TRT clinics” tell every tired 42-year-old he needs injections. Meanwhile, primary care doctors often dismiss textbook hypogonadal symptoms as “just aging.” The truth sits in between: testosterone levels do decline with age, most men adapt without issues, but a meaningful minority — estimated at 2–6% of men aged 40–79 — develop clinically significant deficiency that profoundly affects quality of life [1].
This article will help you distinguish real testosterone deficiency from normal aging, understand when testing is warranted, and weigh the evidence on treatment — including what the testosterone industry doesn’t want you to know about risks.
📋 Key Takeaways
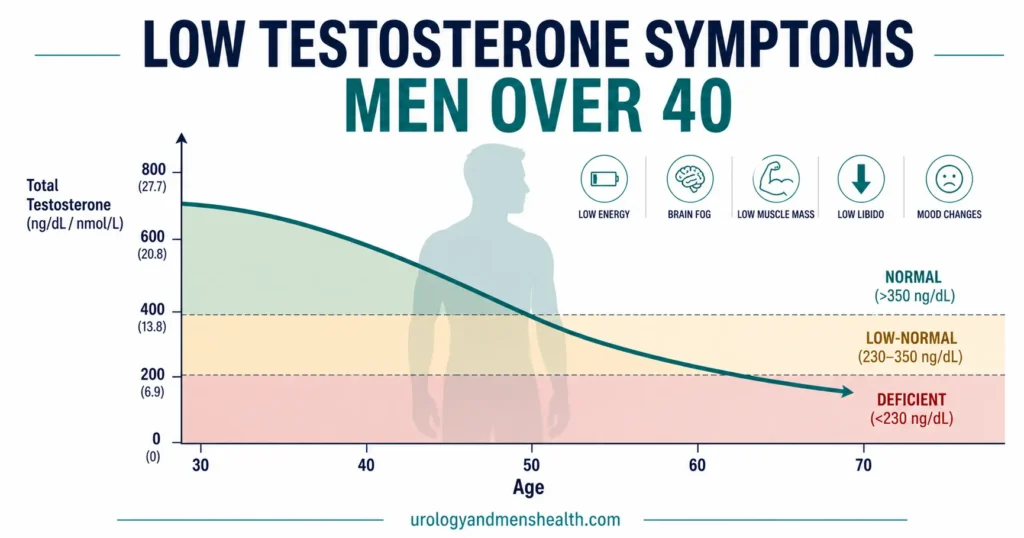
- Testosterone declines by roughly 1–2% per year after age 30. This is normal. Clinical deficiency only applies when levels are genuinely low AND symptoms are present.
- The most commonly missed signs are non-sexual: persistent fatigue, brain fog, loss of motivation, visceral fat gain, and reduced muscle recovery — not just low libido or ED.
- Testosterone must be measured from a fasting morning blood sample (before 10 AM). Afternoon levels can be 20–30% lower and produce false “low” results.
- A total testosterone below 8 nmol/L (230 ng/dL) with symptoms is clear deficiency. The 8–12 nmol/L (230–350 ng/dL) grey zone requires free testosterone and SHBG measurement to interpret [2].
- Testosterone replacement therapy (TRT) works when genuinely indicated — but it suppresses sperm production and is contraindicated in men trying to conceive [3].
- Obesity is the most reversible cause of low testosterone in men over 40. Losing 10% of body weight can raise testosterone by 2–3 nmol/L (60–90 ng/dL) without medication [4].
What Counts as “Low” Testosterone? The Numbers Explained
Testosterone circulates in three forms: tightly bound to sex hormone-binding globulin (SHBG) — roughly 60–70%; loosely bound to albumin — roughly 25–35%; and free (unbound) — approximately 1–3%. The albumin-bound and free fractions together make up bioavailable testosterone — the portion that actually enters cells and produces biological effects [5].
Most labs report total testosterone, which includes all three fractions. The problem is that SHBG rises with age. An older man can have a “normal” total testosterone but genuinely low free testosterone — and it’s the free fraction that drives symptoms. This is why the 8–12 nmol/L (230–350 ng/dL) grey zone exists: a total of 10 nmol/L might be adequate in a man with low SHBG (plenty of free testosterone) but genuinely deficient in a man with high SHBG (very little free testosterone reaching tissues).
The European Association of Urology (EAU) 2024 guidelines define the diagnostic framework as follows [2]:
Total testosterone below 8 nmol/L (230 ng/dL): Unequivocally low. If symptoms are present, treatment is indicated after ruling out secondary causes.
Total testosterone 8–12 nmol/L (230–350 ng/dL): Grey zone. Measure free testosterone and SHBG. If free testosterone is below the age-adjusted reference range, the clinical picture supports deficiency.
Total testosterone above 12 nmol/L (350 ng/dL): Normal range. Symptoms are unlikely to be testosterone-related. Look for other causes — depression, sleep apnea, thyroid dysfunction, chronic disease.
The Low Testosterone Symptoms Men Over 40 Most Often Miss
The symptoms of testosterone deficiency overlap heavily with normal aging, depression, poor sleep, and a sedentary lifestyle. That’s exactly why they’re so often dismissed. But there’s a pattern. When multiple symptoms cluster together in a man over 40, and they don’t respond to the usual interventions (better sleep, exercise, stress management), testosterone deficiency belongs on the differential.
Sexual Symptoms
Reduced libido — not just “less interested” but a genuine absence of spontaneous sexual desire. Men with hypogonadism often describe it as: “I don’t even think about sex anymore — it’s like the switch turned off.”
Erectile dysfunction — particularly loss of nocturnal and morning erections. Testosterone doesn’t control the erection mechanism directly, but it modulates the nitric oxide pathway and is essential for maintaining nocturnal penile tumescence (the automatic erections during REM sleep). When a man tells me he hasn’t had a morning erection in months, testosterone is one of the first things I check.
→ Related Read: Is It ED or Heart Disease? Why Morning Wood Is a “Check Engine” LightNon-Sexual Symptoms — The Ones Most Often Missed
Persistent, unexplained fatigue — not the tiredness that follows a bad night’s sleep, but a deep, constant lack of energy that doesn’t improve with rest. Men describe it as “running on empty” or “the battery never charges.” This is the single most common presenting complaint I see in men later diagnosed with hypogonadism — and the symptom most often attributed to stress, depression, or “just being busy.”
Cognitive changes (“brain fog”) — difficulty concentrating, slowed processing speed, trouble finding words. The hippocampus and prefrontal cortex are rich in androgen receptors. Testosterone deficiency has been linked to reduced verbal memory and spatial cognition in controlled studies [6].
Increased visceral (belly) fat — testosterone regulates fat distribution. Hypogonadal men preferentially accumulate visceral adipose tissue (fat around the organs) rather than subcutaneous fat. This isn’t only cosmetic. Visceral fat is metabolically active and drives insulin resistance, creating a self-reinforcing cycle: low testosterone → more visceral fat → increased aromatization of testosterone to estradiol → even lower testosterone [7].
Loss of muscle mass and strength — testosterone is the primary anabolic hormone in men. Deficiency leads to sarcopenia (progressive muscle loss) that’s disproportionate to age and activity level. Men notice they can’t lift what they used to, recover more slowly from exercise, and lose definition despite maintained training.
Mood changes — irritability, low motivation, anhedonia (inability to enjoy things that used to give pleasure). These overlap almost completely with clinical depression, which is why testosterone deficiency is often misdiagnosed as a mood disorder. The distinction is subtle but real: in testosterone deficiency, mood improves dramatically with replacement therapy. In primary depression, it doesn’t [8].
Poor sleep quality — low testosterone is associated with disrupted sleep architecture, and testosterone itself is partially regulated by sleep. Sleep deprivation can reduce testosterone by 10–15% in just one week of restricted sleep (5 hours/night) [9]. This creates another vicious cycle: poor sleep → low testosterone → worse sleep.
When Should You Get Tested? The Clinical Triggers
Not every tired 40-year-old man needs a testosterone test. But certain symptom patterns and clinical scenarios make testing strongly justified:
Definite indications for testing: Unexplained ED with loss of morning erections. Unexplained infertility. Known pituitary disease, Klinefelter syndrome, or history of bilateral testicular injury or surgery. Chronic opioid use (opioids suppress the hypothalamic-pituitary-gonadal axis). Long-term corticosteroid use. HIV/AIDS.
Strong indications: A cluster of three or more symptoms listed above (fatigue + low libido + visceral fat gain, for example). Type 2 diabetes or metabolic syndrome (prevalence of hypogonadism is 25–40% in diabetic men [10]). Osteoporosis or low-trauma fracture in a man. Gynecomastia (breast enlargement).
Weaker indications (test only if symptoms are prominent): Isolated fatigue without other features. Isolated mood change. Obesity alone — obesity lowers testosterone, but the treatment is weight loss, not TRT.
If you’re unsure whether your own symptom pattern justifies testing, the validated Low Testosterone Symptom Quiz (AMS/ADAM scoring) on this site walks through the most evidence-based screening questions and gives you a result in under two minutes.
How to Get Tested Properly (Most Men Get This Wrong)
Testosterone has a strong circadian rhythm. Levels peak between 7–10 AM and decline by 20–30% by late afternoon [11]. If your blood is drawn at 3 PM after lunch, you may get a falsely low result — triggering unnecessary concern, or worse, unnecessary treatment.
The correct protocol:
1. Fasting morning sample, before 10 AM. Fasting matters because insulin spikes after eating can transiently suppress testosterone.
2. Repeat the test. A single low result is not a diagnosis. The EAU, AUA, and Endocrine Society all require at least two separate morning measurements showing low testosterone before diagnosing hypogonadism [2][12]. Day-to-day variability can be 15–20%.
3. Check more than just total testosterone. A full panel should include: total testosterone, free testosterone (calculated or measured), SHBG, LH (luteinizing hormone), FSH (follicle-stimulating hormone), prolactin, estradiol, and a complete blood count (CBC). LH and FSH determine whether the deficiency is primary (testicular failure — high LH/FSH) or secondary (pituitary or hypothalamic dysfunction — low or inappropriately normal LH/FSH). That distinction completely changes the treatment approach.
4. Rule out reversible causes first. Before starting TRT, investigate and address: obesity, obstructive sleep apnea, chronic opioid or corticosteroid use, alcohol excess, thyroid dysfunction, and iron overload (hemochromatosis). These are all treatable causes of low testosterone that don’t require lifelong hormone replacement.
What Causes Testosterone to Drop? Age Is Only Part of the Story
Age-related testosterone decline is real — roughly 1–2% per year after age 30 — but it’s gradual, and most men maintain levels well above the deficiency threshold into their 60s and 70s [1]. When a man in his 40s or 50s has genuinely low testosterone, there’s usually a contributing factor beyond age alone.
Obesity — The Number One Modifiable Cause
Adipose tissue contains the enzyme aromatase, which converts testosterone to estradiol. The more visceral fat a man carries, the more testosterone is aromatized — a self-reinforcing cycle. Studies show that BMI is a stronger predictor of low testosterone than age in men under 60 [4]. The good news: weight loss of 10–15% body weight can raise total testosterone by 2–3 nmol/L (60–90 ng/dL), sometimes normalizing levels entirely without any medication.
Sleep Deprivation
Testosterone is produced in pulses during deep (stage 3) sleep. Chronic sleep restriction — even to 5 hours per night for one week — has been shown to reduce daytime testosterone by 10–15% in young healthy men [9]. In older men already near the lower threshold, this sleep-mediated suppression can push levels into deficient range.
Chronic Illness and Medications
Type 2 diabetes, metabolic syndrome, chronic kidney disease, liver disease, and HIV all independently suppress testosterone. Opioid analgesics are a particularly common culprit — long-term opioid use suppresses the hypothalamic-pituitary-gonadal (HPG) axis and causes opioid-induced hypogonadism in up to 50% of men on chronic therapy [13]. Corticosteroids, anti-epileptics, and certain chemotherapy agents also suppress testosterone production.
Primary vs Secondary Hypogonadism
Understanding the level of the problem matters for treatment. In primary hypogonadism, the testes themselves are failing — LH and FSH will be elevated (the brain is shouting at the testes to produce more, but they can’t). Causes include Klinefelter syndrome, testicular trauma, mumps orchitis, or prior chemotherapy and radiotherapy.
In secondary (central) hypogonadism, the pituitary or hypothalamus is the problem — LH and FSH will be low or inappropriately normal. Causes include pituitary tumors (especially prolactinoma), chronic opioid use, obesity, head trauma, and idiopathic hypogonadotropic hypogonadism. This distinction matters because secondary hypogonadism may be reversible (remove the opioid, treat the prolactinoma, lose weight), while primary hypogonadism usually requires lifelong replacement.
Download Your Free Clinical Action Plan
Enter your email below to download Dr. Khalid’s complete Evidence-Based ED Action Plan as a free, printable PDF.
Treatment: When TRT Is Appropriate — and When It Isn’t
Testosterone replacement therapy (TRT) is effective for men with confirmed, symptomatic hypogonadism who have had reversible causes excluded. The TRAVERSE trial (2023) — the largest randomized controlled trial of TRT to date, enrolling over 5,200 men aged 45–80 — established that testosterone replacement does not increase cardiovascular risk in men with hypogonadism and pre-existing or high-risk cardiovascular disease, settling a debate that had persisted for over a decade [14].
Benefits demonstrated in trials include improved sexual function (libido, erectile function), increased lean mass and reduced fat mass, improved bone mineral density, and improved mood and energy in genuinely deficient men [15].
→ Related Read: TRT — What I Tell Patients Before StartingTRT Formulations Available
Topical gels (AndroGel, Testim, Testogel, Tostran) — applied daily to shoulders or upper arms. Maintain steady levels. Risk of transfer to partners or children through skin contact (must wash hands and cover the application site).
Intramuscular injections (testosterone cypionate, testosterone enanthate, Sustanon 250, testosterone undecanoate / Aveed in the US, Nebido in Europe) — short-acting cypionate and enanthate are typically given every 1–2 weeks (cause peaks and troughs). Long-acting undecanoate is given every 10–14 weeks and provides the most stable levels of any injectable formulation. It’s often the preferred option for long-term replacement.
Transdermal patches (Androderm) — applied daily, less commonly used due to skin irritation in up to 30% of men.
Oral testosterone undecanoate (Andriol, Jatenzo, Tlando) — taken twice daily with food. Requires fat for absorption. Variable bioavailability makes it less reliable than other formulations.
Critical Warning: TRT and Fertility
This is the single most important thing any man considering TRT must understand: exogenous testosterone suppresses sperm production. When you introduce testosterone from outside the body, the pituitary stops producing LH and FSH — the hormones that drive spermatogenesis. Within 3–6 months of starting TRT, most men become azoospermic (zero sperm count) [3]. In many cases this is reversible after stopping TRT, but not always, and recovery can take 6–12 months or longer.
If you are trying to conceive — or might want to in the future — TRT is not appropriate. Alternative treatments that raise testosterone while preserving fertility exist, including clomiphene citrate (off-label) and human chorionic gonadotropin (hCG), both of which stimulate endogenous testosterone production without shutting down the HPG axis [16].
→ Related Read: Male Infertility — The Conversation Most Urologists Don’t Have With YouThe Testosterone Industry: What They Don’t Tell You
The online testosterone industry has exploded. Direct-to-consumer TRT clinics offer blood tests by mail, video consultations lasting 15 minutes, and monthly subscription injections — sometimes to men whose testosterone is in the normal range. The marketing is aggressive: “Feel 25 again,” “Restore your edge,” “Reclaim your peak.”
There are legitimate concerns with this model:
Treating a number, not a patient. A total testosterone of 11 nmol/L (317 ng/dL) with no symptoms does not warrant treatment. Some clinics use aggressively low thresholds — defining anything below 15 nmol/L (432 ng/dL) as “suboptimal” and prescribing accordingly. The EAU and Endocrine Society are clear: both low levels AND symptoms must be present to diagnose hypogonadism [2][12].
Skipping the work-up. Proper evaluation requires LH, FSH, prolactin, thyroid function, and a clinical history. Some online clinics skip these entirely, meaning secondary causes (pituitary tumor, sleep apnea) go undiagnosed while the patient receives testosterone that masks the underlying problem.
Ignoring fertility implications. I’ve seen men in their late 30s started on TRT by online clinics without being told it would shut down their sperm production. They come to me two years later trying to conceive, azoospermic, wondering why nobody mentioned this.
No exit strategy. TRT suppresses the HPG axis. If you’ve been on exogenous testosterone for years, stopping can leave you with lower testosterone than you started with while your axis recovers — a process that may take months and may be incomplete. This effectively locks patients into lifelong treatment.
Lifestyle Interventions That Actually Raise Testosterone
Before reaching for medication, there are evidence-based interventions that can meaningfully raise testosterone — particularly in men whose levels are suppressed by modifiable factors.
Weight loss: Losing 10% of body weight can increase testosterone by 2–3 nmol/L (60–90 ng/dL). Bariatric surgery in men with severe obesity has been shown to normalize testosterone in up to 50% of cases [4].
→ Related Read: How GLP-1 weight-loss drugs affect testosterone LightResistance training: Heavy compound exercises (squats, deadlifts, bench press) produce acute testosterone spikes and chronic adaptation. Regular resistance training 3–4 times per week has been shown to raise baseline testosterone in sedentary men [17].
Sleep optimization: Aim for 7–9 hours of uninterrupted sleep. Treat obstructive sleep apnea if present — CPAP therapy has been shown to raise testosterone in apneic men.
Stress reduction: Chronic cortisol elevation from psychological stress directly suppresses GnRH (gonadotropin-releasing hormone) at the hypothalamic level, reducing downstream testosterone production.
Moderate alcohol: Heavy alcohol consumption is directly toxic to Leydig cells (the testosterone-producing cells in the testes). Even moderate consumption (3–4 drinks per day) can reduce testosterone by 6–10%.
→ Related Read: Top 3 Prostate Supplements — What the Evidence Actually Says💡 In My Practice
The pattern I see most often is a man in his mid-40s who turns up already taking a PDE5 inhibitor (sildenafil or tadalafil) prescribed by his primary care doctor. The medication “half works” — he can get an erection with it, but his desire is absent and his morning erections have vanished. When I check his testosterone, it’s 7 or 8 nmol/L (200–230 ng/dL). The PDE5 inhibitor was treating the plumbing, but nobody addressed the hormonal driver. Once testosterone is corrected, the PDE5 inhibitor often becomes unnecessary.
I also see the opposite problem just as often — and it worries me more. A 38-year-old, otherwise healthy, comes in already six months into self-funded injections from an online clinic. His testosterone before treatment was 14 nmol/L (404 ng/dL) — comfortably in the normal range. He was told this was “suboptimal.” His symptoms were vague: a bit tired, a bit flat. He felt better on TRT initially (everyone does, briefly). Now his hematocrit is 53%, his testicles have shrunk noticeably, his sperm count is zero, and he and his wife have just started trying for a baby. None of this was explained to him. Unwinding it will take 12 to 18 months, if it unwinds at all.
The lesson from both cases is the same: testosterone is a powerful hormone with real benefits in real deficiency and real harms when prescribed without indication. The work-up matters more than the prescription.
⚠️ When to See a Doctor — Urgently
- Sudden loss of all sexual function plus severe headaches or visual disturbance — this combination suggests a pituitary tumor or apoplexy (pituitary bleeding) and requires urgent MRI and endocrine assessment.
- Breast enlargement (gynecomastia) that is new, rapid, or painful — while often benign, rapid-onset gynecomastia can indicate a hormone-producing tumor (testicular or adrenal) and needs investigation.
- Testicular shrinkage, pain, or a new lump — testicular atrophy can signal primary hypogonadism, but a new lump must always be investigated urgently to exclude testicular cancer.
- Mood deterioration with thoughts of self-harm — while low testosterone can cause mood changes, this requires immediate mental health assessment regardless of the underlying cause.
- Already on TRT and developing polycythemia symptoms (headache, flushing, dizziness, visual changes) — TRT stimulates red cell production. A hematocrit above 54% increases stroke and venous thromboembolism risk and requires urgent dose adjustment or therapeutic phlebotomy.
Frequently Asked Questions
Does low testosterone cause erectile dysfunction in men over 40?
It can contribute, but it’s rarely the sole cause. Testosterone modulates the nitric oxide pathway that initiates erections, and it drives nocturnal penile tumescence (the automatic erections during REM sleep). When testosterone is genuinely deficient, men typically lose morning erections first, then develop reduced spontaneous erections, and finally difficulty achieving erections even with stimulation. However, most ED in men over 40 is vascular — caused by endothelial dysfunction from hypertension, diabetes, or smoking. The clinical clue is morning erections: if they’re absent, testosterone should be checked. If they’re present, the problem is more likely vascular, neurological, or psychological.
Can I boost testosterone naturally without medication?
Yes — if your levels are in the low-normal range and suppressed by modifiable factors. Weight loss is the most powerful natural intervention: losing 10% of body weight can raise testosterone by 2–3 nmol/L (60–90 ng/dL). Regular resistance training (3–4 sessions per week, compound movements), 7–9 hours of quality sleep, stress reduction, and moderate alcohol intake all have evidence supporting modest testosterone increases. However, if your total testosterone is below 8 nmol/L (230 ng/dL), lifestyle changes alone are unlikely to normalize levels — you’ll likely need medical treatment. Beware of “testosterone booster” supplements: most (ashwagandha, tribulus, D-aspartic acid) have weak or no evidence supporting clinically meaningful testosterone increases in hypogonadal men [18].
Will testosterone replacement therapy make me infertile?
Yes, in the vast majority of cases. Exogenous testosterone tells your pituitary gland to stop producing LH and FSH — the hormones that stimulate the testes to produce sperm. Within 3–6 months, most men on TRT become azoospermic (zero sperm count). This is usually reversible after stopping TRT, but recovery takes 6–12 months and is not guaranteed — some men have persistent oligospermia. If you want children now or in the future, do not start TRT without first discussing fertility-preserving alternatives such as clomiphene or hCG with a urologist or reproductive endocrinologist. See male infertility causes for the full picture.
Is testosterone replacement therapy safe for the heart?
The TRAVERSE trial (2023) — the largest cardiovascular safety trial of TRT — enrolled over 5,200 men aged 45–80 with hypogonadism and pre-existing or high-risk cardiovascular disease. It demonstrated that testosterone replacement did not increase the rate of major cardiovascular events (heart attack, stroke, cardiovascular death) compared to placebo over a median follow-up of 33 months. This largely resolved the safety concern raised by earlier, smaller, and methodologically flawed studies. That said, TRT does increase hematocrit (red blood cell concentration), which raises blood viscosity and thrombosis risk if unchecked. Regular blood monitoring every 3–6 months is mandatory during treatment.
What’s the difference between a testosterone “booster” supplement and actual TRT?
They are fundamentally different things. “Testosterone boosters” are unregulated dietary supplements (ashwagandha, fenugreek, tribulus terrestris, zinc, D-aspartic acid) marketed to raise testosterone naturally. Most have no rigorous evidence showing clinically meaningful increases in total testosterone in hypogonadal men. Some may produce small, statistically significant increases in studies — but a 0.5 nmol/L bump is not going to change how you feel or function. TRT is pharmaceutical-grade testosterone (gel, injection, or patch) prescribed after a confirmed diagnosis, which raises levels into the normal physiological range. It’s the difference between a food supplement and actual medicine — and the regulatory, evidence, and monitoring standards reflect that.
📚 References
- Wu FC, Tajar A, Beynon JM, et al. Identification of late-onset hypogonadism in middle-aged and elderly men. N Engl J Med. 2010;363(2):123-135. PubMed
- Salonia A, Bettocchi C, Boeri L, et al. EAU Guidelines on Sexual and Reproductive Health. European Association of Urology, 2024. EAU Guidelines
- Patel AS, Leong JY, Ramasamy R. Prediction of male infertility by the World Health Organization laboratory manual. J Urol. 2018;199(4):1007-1012. PubMed
- Corona G, Rastrelli G, Monami M, et al. Body weight loss reverts obesity-associated hypogonadotropic hypogonadism: a systematic review and meta-analysis. Eur J Endocrinol. 2013;168(6):829-843. PubMed
- Vermeulen A, Verdonck L, Kaufman JM. A critical evaluation of simple methods for the estimation of free testosterone in serum. J Clin Endocrinol Metab. 1999;84(10):3666-3672. PubMed
- Holland J, Bandelow S, Hogervorst E. Testosterone levels and cognition in elderly men: a review. Maturitas. 2011;69(4):322-337. PubMed
- Kelly DM, Jones TH. Testosterone and obesity. Obes Rev. 2015;16(7):581-606. PubMed
- Zarrouf FA, Artz S, Griffith J, et al. Testosterone and depression: systematic review and meta-analysis. J Psychiatr Pract. 2009;15(4):289-305. PubMed
- Leproult R, Van Cauter E. Effect of 1 week of sleep restriction on testosterone levels in young healthy men. JAMA. 2011;305(21):2173-2174. PubMed
- Dhindsa S, Prabhakar S, Sethi M, et al. Frequent occurrence of hypogonadotropic hypogonadism in type 2 diabetes. J Clin Endocrinol Metab. 2004;89(11):5462-5468. PubMed
- Brambilla DJ, Matsumoto AM, Araujo AB, McKinlay JB. The effect of diurnal variation on clinical measurement of serum testosterone and other sex hormone levels in men. J Clin Endocrinol Metab. 2009;94(3):907-913. PubMed
- Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744. PubMed
- Rubinstein AL, Carpenter DM. Association between commonly prescribed opioids and androgen deficiency in men. J Pain Palliat Care Pharmacother. 2017;31(1):3-13. PubMed
- Lincoff AM, Bhasin S, Flevaris P, et al. Cardiovascular safety of testosterone-replacement therapy. N Engl J Med. 2023;389(2):107-117. PubMed
- Snyder PJ, Bhasin S, Cunningham GR, et al. Effects of testosterone treatment in older men. N Engl J Med. 2016;374(7):611-624. PubMed
- Wheeler KM, Sharma D, Kavoussi PK, et al. Clomiphene citrate for the treatment of hypogonadism. Sex Med Rev. 2019;7(2):272-276. PubMed
- Kumagai H, Zempo-Miyaki A, Yoshikawa T, et al. Increased physical activity has a greater effect than reduced energy intake on lifestyle modification-induced increases in testosterone. J Clin Biochem Nutr. 2016;58(1):84-89. PubMed
- Clemesha CG, Thaker H, Samplaski MK. ‘Testosterone boosting’ supplements composition and claims are not supported by the academic literature. World J Mens Health. 2020;38(1):115-122. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.