Penile Cancer: Symptoms, Causes & Treatment | Urologist
Penile cancer is rare, but the men who delay coming to a urologist often lose options that early presenters keep. Here is what I look for, why HPV changed the conversation, and how modern surgery preserves the organ when we catch it in time.

Penile cancer is rare — fewer than 1 in 100,000 men in the United States are diagnosed each year — but the men who walk into my clinic with advanced disease almost always say the same thing: “I noticed it months ago, but I hoped it would go away.” It doesn’t. Penile cancer is one of the most treatable urological cancers when caught at Stage 0 or Stage I, and one of the hardest to control once it reaches the groin lymph nodes. For the full picture of related procedures and what to expect, see our Surgery & Recovery Hub. This article walks you through exactly what penile cancer looks like, why HPV has changed the conversation, how we stage it, and why modern surgery now preserves the organ in most early cases instead of removing it.
Key Takeaways
- Any penile lesion that does not heal within 4 weeks needs a urologist — biopsy is the only way to rule out cancer.
- HPV types 16 and 18 are found in around half of penile cancer cases; the HPV vaccine prevents the strains responsible.
- Phimosis (a foreskin that cannot retract) raises lifetime risk 5-10 fold; chronic inflammation underneath is the mechanism.
- Stage 0 and Stage I disease are cured in over 90% of cases with organ-sparing treatment — topical cream, laser, glans resurfacing, or wide local excision.
- Groin lymph node status is the single biggest predictor of survival. Once nodes are involved, 5-year survival drops sharply.
What Is Penile Cancer?
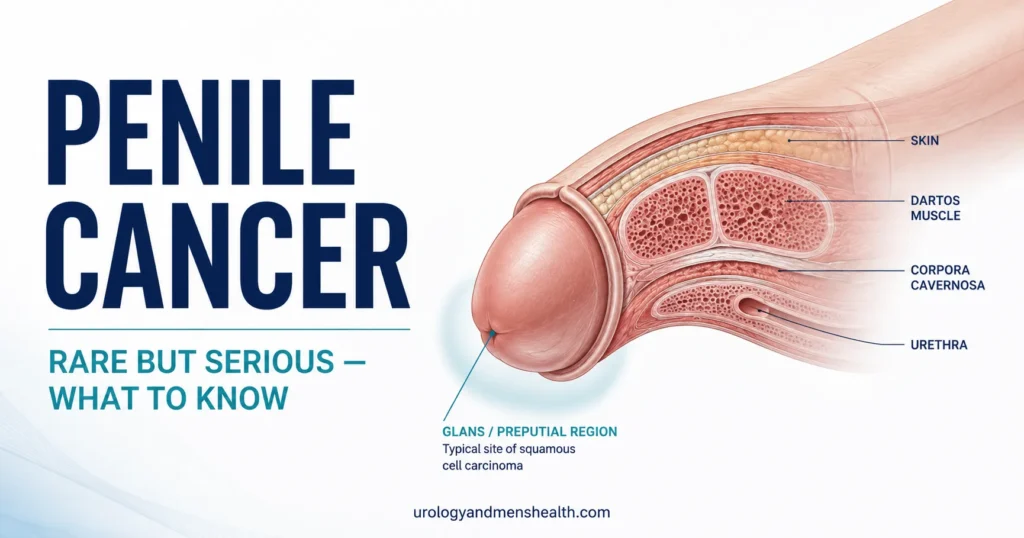
Penile cancer is a malignant growth that starts in the skin or tissues of the penis. More than 95% of cases are squamous cell carcinoma (SCC) — the same cell type as most skin cancers — arising from the flat epithelial cells covering the glans (head) and foreskin. Rarer types include melanoma, basal cell carcinoma, sarcoma, and adenocarcinoma of the urethra, but for practical purposes when I say “penile cancer” in clinic, I mean SCC.
The disease almost always begins on the surface. The glans (the head of the penis) is the most common starting point, accounting for around 48% of tumors. The foreskin accounts for about 21%, both glans and foreskin together another 15%, and the coronal sulcus (the groove just behind the head) about 6%. Shaft skin tumors are uncommon. This geographic pattern matters clinically — anything chronic, painless, and stubborn at one of these sites needs a urologist’s eye, not another tube of antifungal cream.
Penile cancer typically grows slowly outward across the surface before it invades downward. That slow biology is both the good news and the trap. The good news: early disease is highly curable. The trap: men assume something that hasn’t dramatically changed in three months can’t be cancer. Painlessness is not reassurance — it’s one of the classic features.
Warning Signs: What Penile Cancer Looks Like
There is no single appearance. The earliest changes are easy to dismiss — a small patch of thickened skin, a velvet-red flat plaque, a tiny ulcer that crusts over and then comes back. Most early penile cancers are painless, which is the single biggest reason men delay coming in.
The features that should send you to a urologist within days, not months:
- A lump, wart-like growth, or thickened patch on the glans, foreskin, or coronal sulcus that has been there more than 4 weeks
- A non-healing sore or ulcer — even small, even painless
- White, thickened skin (leukoplakia) that does not respond to a steroid cream
- A flat, velvety red patch (erythroplasia of Queyrat) on the glans — this is carcinoma in situ until proven otherwise
- Bleeding, foul-smelling discharge, or skin breakdown under the foreskin in an uncircumcised man
- A palpable lump in the groin — this can be the first thing a man notices if the primary lesion is hidden under a tight foreskin
- A bluish or brown-black pigmented spot on the penis — could be melanoma
The differential matters because most of what comes through my door is benign — pearly penile papules, Fordyce spots, lichen sclerosus, balanitis, genital warts. For a fuller rundown of what’s normal versus what needs a doctor, see penile health: what’s normal and what needs a doctor. The rule I give every patient: any lesion that has not resolved in 4 weeks needs a biopsy, not another empirical course of cream.
In My Practice
The man who taught me the most about penile cancer was 52, married, and had a white thickened patch on his glans for eighteen months. He’d been treated by three doctors — antifungal cream, then steroid cream, then a stronger antifungal. Each course made him feel he was being looked after. When he finally reached me the lesion had become a 2 cm ulcer with palpable groin nodes — Stage III disease. He needed a partial penectomy and bilateral groin dissection. Earlier, he would have needed a glansectomy at most, possibly just a topical cream.
The lesson I take into every consultation: a penile lesion that does not heal in 4 weeks gets biopsied — not retreated empirically.
What Causes Penile Cancer: HPV, Phimosis, and Other Risks
Penile cancer is not one disease with one cause. Roughly half the cases worldwide are driven by human papillomavirus (HPV) — the same family of viruses that causes cervical, anal, and oropharyngeal cancer. The other half are driven by chronic inflammation — most often from phimosis (a non-retractile foreskin) trapping smegma and bacteria against the glans for decades.[1]
HPV: the most preventable risk factor
HPV 16 and HPV 18 are found in approximately 50% of penile squamous cell carcinomas, with HPV 16 alone responsible for the majority. The virus integrates into the DNA of epithelial cells, switches off the body’s normal tumor-suppressor proteins (p53 and Rb), and over years to decades drives the progression from normal skin to precancer to invasive cancer.[2]
The HPV vaccine (Gardasil 9 in the US, covering HPV types 6, 11, 16, 18, 31, 33, 45, 52, 58) prevents the strains responsible for most HPV-related penile cancer. CDC recommends routine vaccination at age 11-12 with catch-up through age 26, and shared-decision-making vaccination through age 45.[3] If you have sons, this is the single most effective penile cancer prevention strategy that exists.
Phimosis and chronic inflammation
Phimosis raises lifetime penile cancer risk roughly 5-10 fold. The mechanism is straightforward: a foreskin that cannot be retracted traps smegma (shed skin cells, oils, and bacteria) against the glans. Over years, this creates a chronic low-grade inflammatory environment — the same kind of cellular turnover and DNA damage that drives many epithelial cancers. Neonatal circumcision is associated with a near-zero risk of penile cancer; adult circumcision after the foreskin has been chronically inflamed reduces but does not eliminate risk. For the medical indications and the evidence around adult procedures, see when adult circumcision is medically indicated.
Other risk factors
- Smoking — current smokers have 3-4x the risk of never-smokers; the carcinogens are excreted in urine and concentrate at the meatus.
- Lichen sclerosus (balanitis xerotica obliterans) — chronic scarring skin condition that progresses to invasive cancer in around 5% of cases.
- PUVA therapy for psoriasis — the combination of psoralen and UV-A light raises penile cancer risk substantially; modern treatment protocols now shield the genitals.
- Immunosuppression — HIV, organ transplant recipients, long-term corticosteroids.
- Age over 60 — most cases are diagnosed between 50 and 70.
- Poor genital hygiene — particularly under a tight foreskin.
How Penile Cancer Is Staged and Diagnosed
Diagnosis starts with a punch or excisional biopsy of the lesion under local anesthetic — this is a 15-minute procedure in clinic. Histology confirms squamous cell carcinoma and grades it (Grade 1 well-differentiated through Grade 3 poorly differentiated). HPV testing (p16 immunohistochemistry) is now standard because HPV-positive tumors tend to behave slightly differently from HPV-negative ones.[4]
Once cancer is confirmed, staging answers two questions: how deep, and has it spread? Penile cancer uses the TNM system (Tumor, Node, Metastasis):
- Stage 0 (carcinoma in situ, Tis) — abnormal cells confined to the surface layer; not yet invasive. 5-year survival approaches 100%.
- Stage I (T1a) — invades subepithelial connective tissue, no lymphovascular invasion, well or moderately differentiated. 5-year survival around 85-95%.
- Stage II (T2 or T3) — invades corpus spongiosum, urethra, or corpus cavernosum. 5-year survival 60-80%.
- Stage III — regional inguinal (groin) lymph node involvement. 5-year survival drops to 30-50% depending on number and laterality of nodes.
- Stage IV — pelvic nodes, fixed groin mass, or distant metastasis. 5-year survival under 20%.
Local staging in most modern centers uses penile MRI with artificial erection (induced with intracorporeal alprostadil) — it shows tumor depth and corpus cavernosum invasion better than any other modality. For groin staging, dynamic sentinel lymph node biopsy is now the standard of care for clinically node-negative patients with T1b or higher tumors, per the AUA 2023 update and EAU 2024 guidelines.[5] It has largely replaced empirical bilateral groin dissection — the old approach that left many men with severe, lifelong leg lymphedema.
For Stage III+ disease, a PET-CT is added to look for pelvic and distant disease. Useful tools while you’re working through staging questions include the Urology Surgery Comparison Tool, which lays out incision, recovery, and side-effect trade-offs across the procedures discussed below.
Treatment Options: From Cream to Glansectomy
The shift in penile cancer care over the last fifteen years has been dramatic. Where the standard answer used to be partial or total penectomy for almost any invasive tumor, the modern principle is organ-preservation wherever oncologically safe — because function, urinary stream, and psychological well-being matter, and because we can still re-operate if margins are positive.[6]
Stage 0 (carcinoma in situ)
First-line treatment is topical chemotherapy — 5-fluorouracil 5% cream or imiquimod 5% cream, applied for 4-8 weeks. Around 50-60% of patients clear completely with cream alone. For non-responders or recurrences, options are CO2 or Nd:YAG laser ablation, photodynamic therapy, or wide local excision. Penectomy is never appropriate at this stage.
Stage I (T1a — superficial, low-grade)
Organ-sparing options dominate: wide local excision with a 5 mm margin, glans resurfacing (the entire glans epithelium is removed and replaced with a split-thickness skin graft), Mohs micrographic surgery, or brachytherapy (radiation seeds placed temporarily in the lesion). All preserve the penile shaft, the ability to urinate standing, and erectile function. Local recurrence rates are 5-15%, but recurrences are caught early on surveillance and re-treated.
Stage II (T2/T3 — invades corpus spongiosum or cavernosum)
The workhorse operation is glansectomy with reconstruction. The glans is removed at the level of the corpora cavernosa, and a new “neoglans” is constructed using a split-thickness skin graft. Most men retain erectile function and urinate standing; sensation is reduced but not absent. For tumors that invade the corpora cavernosa themselves, partial penectomy (removal of the distal portion of the penis with a 1-2 cm clear margin) is needed — preserving as much length as oncologically possible. Total penectomy is reserved for tumors that involve the proximal shaft or perineum.
Stage III (groin nodes involved)
Once nodes are positive, treatment is multimodal: inguinal lymph node dissection (on the affected side, often bilateral if multiple nodes are involved), often combined with neoadjuvant or adjuvant chemotherapy (cisplatin-based regimens — TIP: paclitaxel, ifosfamide, cisplatin) and sometimes radiation. The aim shifts from organ preservation to disease control. Survival at 5 years ranges from 30% to 50% depending on how many nodes are involved, whether disease has broken through the lymph node capsule (extranodal extension), and whether pelvic nodes are positive.[7]
Stage IV (distant spread)
Treatment is palliative and systemic — cisplatin-based chemotherapy, sometimes radiation for symptomatic local disease, and increasingly clinical trials of immunotherapy (anti-PD-1 agents like pembrolizumab show some activity in HPV-associated tumors). Five-year survival is under 20%, which is why every effort goes into early diagnosis. For a broader sense of how surgical decision-making works across urology — the trade-offs we weigh between preserving function and clearing disease — the principles behind kidney stone surgery selection reflect the same surgeon’s logic applied to a different organ.
When to Go to the ER (Not Wait for a Clinic Appointment)
Most penile lesions are not emergencies — they need a urology appointment within days to weeks, not a 3 AM hospital visit. But these symptoms need immediate emergency care:
- Heavy, uncontrolled bleeding from a penile lesion that does not stop with firm pressure for 10 minutes
- Acute urinary retention — being unable to pass urine at all because a tumor is obstructing the urethra
- Rapidly expanding groin mass with skin breakdown, fever, or signs of infection
- Severe acute scrotal or penile pain with a hard, fixed mass
Life After Treatment: Function, Sex, and Surveillance
The conversations I have after surgery are often harder than the ones before. Men want to know two things: will I urinate normally, and will I have sex again? The honest answer depends on what was done.
After topical cream, laser, or wide local excision, function is essentially unchanged. After glans resurfacing or glansectomy with reconstruction, most men retain the ability to urinate standing and to achieve erections suitable for penetration; sensation in the reconstructed glans is reduced but returns partially over 6-12 months. PDE-5 inhibitors (sildenafil, tadalafil) and vacuum erection devices are often useful adjuncts.
After partial penectomy, the residual penis usually retains enough length for sitting urination and, in many cases, penetrative sex; some men opt for phalloplasty reconstruction later. After total penectomy, a perineal urethrostomy is created (men urinate sitting); reconstructive options including phalloplasty exist but are major undertakings.
After inguinal lymphadenectomy, the main long-term issue is lower-limb lymphedema — chronic swelling of the leg from disrupted lymph drainage. Modern video-endoscopic and robotic-assisted inguinal dissection has reduced this complication substantially compared with the open approach. Compression stockings, weight management, and early physical therapy referral all help. Yearly checks with your urologist alongside the wider screening framework in our men’s health checklist over 40 keep you on top of both recurrence and the comorbidities that often co-travel.
One issue men rarely raise but always struggle with: psychological impact. Penile cancer treatment touches identity, masculinity, and intimacy in ways that other urological surgery does not. Referral to a psychosexual counselor or specialist nurse should be routine, not optional. Don’t wait to be offered it — ask.
Surveillance schedule
Around 75% of recurrences happen within the first 2 years. Per AUA 2023 and EAU 2024 guidelines, the standard schedule is:
- Years 1-2: physical exam and groin palpation every 3 months. Monthly self-exam between visits. Groin ultrasound every 6 months for high-risk patients (T1b or higher, lymphovascular invasion, high-grade).
- Years 3-5: physical exam every 6 months. Annual imaging if high-risk.
- Beyond 5 years: annual urology follow-up plus monthly self-exam. The risk of late recurrence is low but not zero.
The single most important component is the monthly self-exam — and this is something every man should learn how to do whether or not he has had cancer. The Men’s Health Screening tool runs through the broader self-check framework and shows where penile self-exam sits inside it — see the Men’s Health Screening Checklist tool.
Because erectile function and cardiovascular risk are often entwined — and because PDE-5 inhibitors are a mainstay of post-surgical sexual rehabilitation — the workup for vascular-cause ED detailed in ED and heart disease: why morning wood matters applies to penile cancer survivors too. Many men assume their post-surgery ED is purely anatomical; in their 60s and 70s it is often half anatomy and half undiagnosed vascular disease.
Frequently Asked Questions About Penile Cancer
Can penile cancer be cured if I catch it early?
Yes — early penile cancer has one of the highest cure rates in urological oncology. Stage 0 (carcinoma in situ) is cured in essentially 100% of patients with topical cream, laser, or wide local excision. Stage I is cured in 85-95% with organ-sparing surgery. The cure rate falls sharply once lymph nodes are involved, which is why any lesion that has not healed in 4 weeks needs a biopsy, not another empirical cream. See penile health: when to see a doctor for the full warning-sign list.
Does HPV cause penile cancer in all men with the virus?
No. Most men who acquire HPV clear the virus within 2 years without consequence. Only a small minority develop persistent infection with high-risk strains (mainly HPV 16 and 18), and only a fraction of those progress to penile cancer over decades. HPV is found in around 50% of penile cancer cases globally. The HPV vaccine is highly effective at preventing the strains responsible and is recommended for boys at age 11-12 with catch-up through age 26.
Does circumcision prevent penile cancer?
Neonatal circumcision is associated with a near-zero lifetime risk of penile cancer — the strongest single piece of evidence in this whole field. Adult circumcision performed before chronic inflammation has set in also reduces risk, though not to neonatal levels. Adult circumcision performed after years of phimosis and chronic balanitis reduces risk but does not eliminate it. Medical indications for adult circumcision covers the specifics.
What does early penile cancer look like compared with normal skin conditions?
The classic early appearances of penile cancer are a velvet-red flat plaque on the glans (erythroplasia of Queyrat), a thickened white patch (leukoplakia), or a small painless ulcer or lump that does not heal. Common benign mimics include pearly penile papules (tiny dome-shaped bumps around the corona — entirely normal), Fordyce spots (yellowish sebaceous spots — normal), lichen sclerosus (white scarring change — needs treatment but rarely malignant), and genital warts. The defining test is time: anything that has not resolved in 4 weeks needs a biopsy.
Will I still be able to have sex after penile cancer treatment?
For most early-stage patients, yes. After topical cream, laser, or wide local excision, sexual function is essentially unchanged. After glansectomy with reconstruction or partial penectomy, most men retain the ability to achieve erections suitable for penetration, though sensation is reduced. PDE-5 inhibitors and vacuum devices are often useful. Total penectomy changes sexual function significantly; phalloplasty reconstruction is an option. Psychosexual counseling should be offered routinely — ask if you are not offered it.
How often does penile cancer come back after treatment?
About 75% of recurrences happen in the first 2 years, which is why follow-up is intense in that window — physical exam and groin palpation every 3 months, with groin ultrasound every 6 months for higher-risk tumors. Organ-sparing treatments (cream, laser, glans resurfacing) have higher local recurrence rates (5-15%) than penectomy, but recurrences are usually caught early on surveillance and re-treated successfully. Late recurrences beyond 5 years are uncommon but possible, so annual urology follow-up and monthly self-exam remain important long-term.
References
- Hakenberg OW, Compérat EM, Minhas S, et al. EAU Guidelines on Penile Cancer. European Association of Urology. 2024 edition. EAU Guidelines
- Olesen TB, Sand FL, Rasmussen CL, et al. Prevalence of human papillomavirus DNA and p16INK4a in penile cancer and penile intraepithelial neoplasia: a systematic review and meta-analysis. Lancet Oncology. 2019;20(1):145-158. PubMed
- Meites E, Szilagyi PG, Chesson HW, et al. Human Papillomavirus Vaccination for Adults: Updated Recommendations of the Advisory Committee on Immunization Practices. MMWR Morbidity and Mortality Weekly Report. 2019;68(32):698-702. CDC MMWR
- Clark PE, Spiess PE, Agarwal N, et al. Penile cancer: clinical practice guidelines in oncology. Journal of the National Comprehensive Cancer Network. 2013;11(5):594-615. AUA Guideline
- Spiess PE, Dhillon J, Baumgarten AS, et al. Pathophysiological basis of human papillomavirus in penile cancer: Key to prevention and delivery of more effective therapies. CA: A Cancer Journal for Clinicians. 2016;66(6):481-495. PubMed
- Sakalis VI, Campi R, Barreto L, et al. What is the most effective management of the primary tumor in patients with invasive penile cancer: A systematic review of the available treatment options and their outcomes. European Urology Open Science. 2022;40:58-94. PubMed
- Pagliaro LC, Williams DL, Daliani D, et al. Neoadjuvant paclitaxel, ifosfamide, and cisplatin chemotherapy for metastatic penile cancer: a phase II study. Journal of Clinical Oncology. 2010;28(24):3851-3857. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.