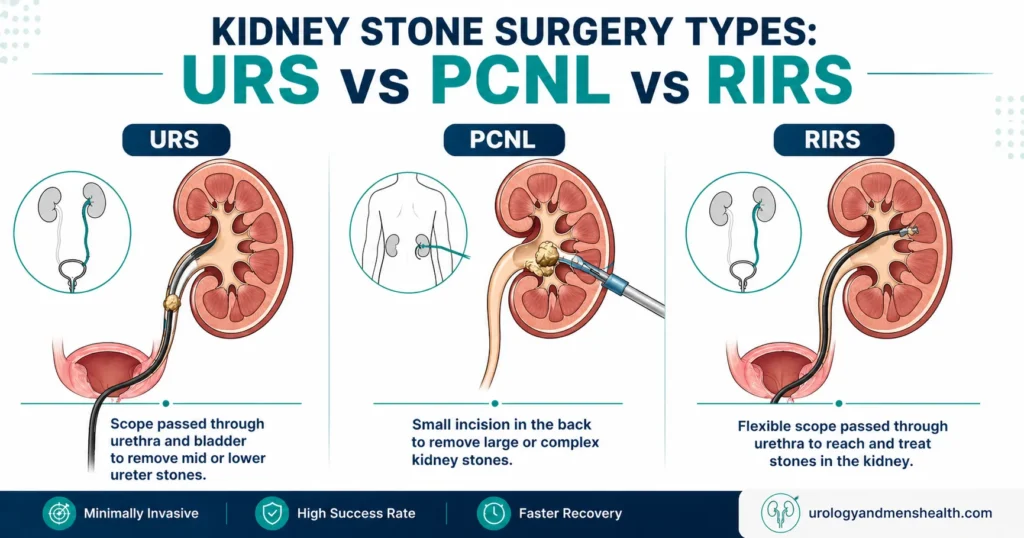
Kidney Stone Surgery Types: URS vs PCNL vs RIRS
Patients often assume that any kidney stone surgery will successfully clear their urinary tract, viewing the different procedures as totally interchangeable. The harsh clinical reality is that choosing the wrong operation—whether URS, PCNL, or RIRS—frequently leads to a painful second surgery or leftover fragments that guarantee another stone in 18 months. As a specialist urologist who performs all three, here is my unfiltered guide on how we match the exact procedure to your stone's size and location, and what your recovery will actually look like.

The three main kidney stone surgery types — URS, PCNL, and RIRS — are not interchangeable. The wrong choice can mean a longer recovery, an avoidable second procedure, or a stone fragment left behind that becomes the seed for the next stone in 18 months. I am Dr. Muhammad Khalid, a specialist urologist (MBBS, FCPS Urology, IMC #539472), and I perform all three of these procedures regularly. The surgery you are offered should match three things: the size of your stone, where it sits in your urinary tract, and your overall anatomy and health.
This guide walks you through how each operation works, what recovery actually looks like, and how I make this decision in clinic. By the end, you will know which questions to ask your surgeon — and roughly which procedure to expect based on your imaging.
Key Takeaways
- URS (ureteroscopy) is the first choice for stones in the lower or mid-ureter, especially under 10 mm.
- RIRS (flexible ureteroscopy) is best for stones inside the kidney itself — typically 1–2 cm — when there is no incision option needed.
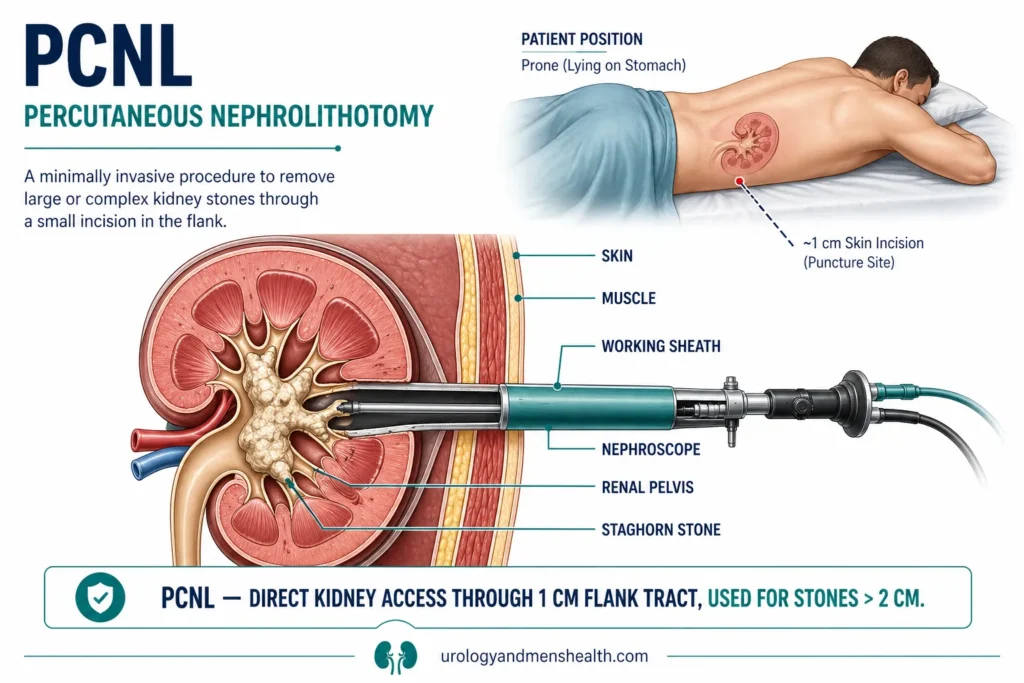
- PCNL (percutaneous nephrolithotomy) is the gold standard for large kidney stones over 2 cm or staghorn stones, and uses a 1 cm flank puncture.
- ESWL (shockwave lithotripsy) is a separate, non-surgical option for selected stones — covered in a different guide.
- A ureteral stent is placed in most cases for 1–2 weeks afterward; this is normal, not a complication.
- Stone-free rates vary: URS ~85–95%, RIRS ~80–90%, PCNL ~85–95% for the right patient.
Why Stone Size and Location Decide the Surgery
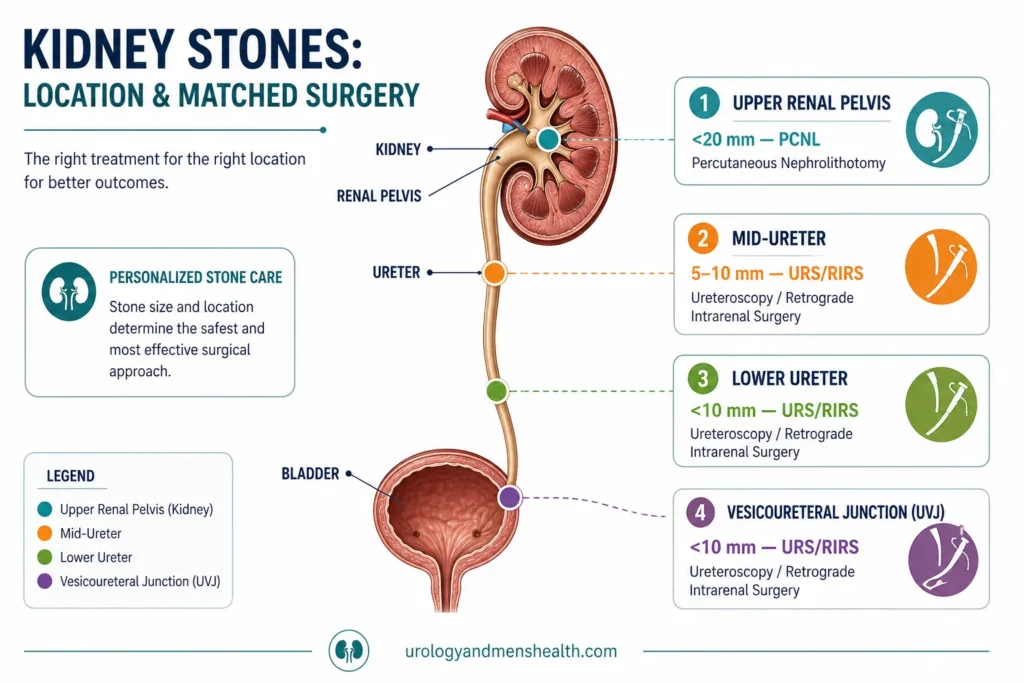
Two stones, both 12 mm, can need completely different operations depending on where they sit. A 12 mm stone in the lower ureter near the bladder is reachable with a rigid scope passed up through the urethra — a URS. The same 12 mm stone in the upper pole of the kidney needs a flexible scope that can curve around inside the renal collecting system — a RIRS. And if that stone is actually 25 mm and shaped like a stag’s antlers filling the renal pelvis, neither will clear it efficiently, and you need a small flank puncture — a PCNL [1].
Three numbers drive the decision in clinic:
- Stone size — measured on non-contrast CT, the gold standard. Anything under 10 mm has options; over 20 mm usually means PCNL.
- Location — lower ureter, mid-ureter, upper ureter, renal pelvis, lower pole calyx. Each is a different mechanical problem.
- Stone density (Hounsfield units) — denser stones (over 1,000 HU) are harder to fragment and often steer me toward direct contact lasering rather than shockwaves.
Body habitus matters too. A patient with severe obesity may have anatomy that makes flank puncture difficult; a patient on blood thinners may need a procedure that minimises bleeding risk. None of this is mysterious — it is just a checklist your surgeon runs in their head before recommending an option.
→ Related Read: Kidney Stones — The Complete Guide from a UrologistThe Three Main Kidney Stone Surgery Types: A Side-by-Side
Before going deep into each procedure, here is the comparison I draw on a whiteboard for patients in clinic. This is not a substitute for a surgical consultation — but it tells you what to expect and where the trade-offs sit.
URS (Ureteroscopy): A semi-rigid scope (about 3 mm wide / ⅛ inch) is passed up through the urethra and bladder into the ureter. Best for ureteral stones, especially in the lower two-thirds. No skin incision. Same-day or 1-night stay. Stent for 7–14 days.
RIRS (Retrograde Intrarenal Surgery): A thin flexible scope (about 2.5 mm / under ⅛ inch) follows the same route as URS but bends around inside the kidney to reach stones in the renal pelvis or calyces. Best for kidney stones 1–2 cm or stones in difficult-to-reach lower pole calyces. No skin incision. Same-day or 1-night stay. Stent for 7–14 days.
PCNL (Percutaneous Nephrolithotomy): A 1 cm puncture is made through the flank skin under imaging guidance, and a working sheath is dilated through the soft tissue directly into the kidney. A nephroscope and laser or ultrasound probe break and remove the stone. Best for stones over 2 cm (about ⅘ inch) and staghorn stones. 1–3 night hospital stay. A small drain may be left for 24 hours [2].
💡 In My Practice
A 42-year-old patient came in convinced he needed open surgery because his stone was “too big for keyhole” — that was the phrase a friend had given him. His CT showed a 14 mm stone in the renal pelvis. We did a single RIRS session, fragmented it with a holmium laser, and he was back at his desk job four days later with a stent in place that came out at his two-week appointment.
The lesson: the word “big” means different things to different specialties. A 14 mm renal pelvis stone is a textbook RIRS case, not an open-surgery case. If you have been told you need a major operation, get a second opinion from a urologist who does endoscopic stone surgery before you accept it.
URS (Ureteroscopy): The Workhorse for Mid-Tract Stones
URS is the most commonly performed kidney stone surgery worldwide. The reason is simple: most stones that fail to pass on their own are sitting somewhere in the ureter — the narrow tube between kidney and bladder — and a semi-rigid scope passed retrograde (upward, through the urinary tract) reaches them efficiently [3].
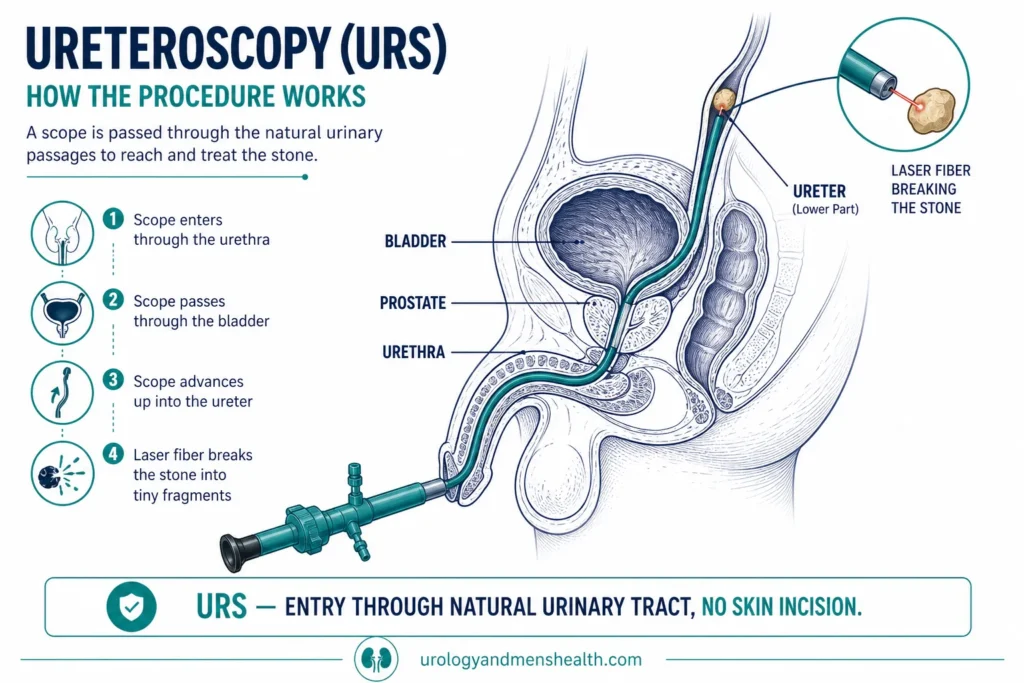
How URS Works
You receive a general or spinal anesthetic. A scope no thicker than a thin pencil is passed through the urethra (the urinary opening), across the bladder, and up the ureter to the stone. A holmium:YAG laser fiber is fed through a working channel inside the scope, and the stone is fragmented into dust or small pieces that can be flushed out or extracted with a basket. A ureteral stent — a soft plastic tube about 26 cm long — is then left in place, sitting between the kidney and bladder, to keep the ureter open while it heals.
Who URS Is For
- Stones in the lower or mid-ureter, any size up to about 15 mm (⅗ inch)
- Upper ureteral stones under 10 mm (⅖ inch) where flexible scope access is straightforward
- Patients who need a definitive answer in one session and cannot wait for repeated ESWL attempts
- Patients on blood thinners — URS bleeds far less than PCNL
URS Stone-Free Rates
For ureteral stones in the right size band, the stone-free rate after a single URS is around 85–95% depending on stone size, location, and density. Stones higher up in the ureter near the kidney drop slightly because access is harder. American Urological Association guidelines list URS as a first-line option for both upper and lower ureteral stones [4].
→ Related Read: How to Pass a Kidney Stone Fast — What I Tell My PatientsPCNL: When the Stone Is Too Big for the Pipes
PCNL stands for percutaneous nephrolithotomy — “through the skin, into the kidney, to remove a stone.” It is the procedure of choice when the stone is larger than 2 cm (about ⅘ inch), when there are multiple stones in the kidney, or when the stone has the branched, antler-like shape we call staghorn [5].
How PCNL Works
You are given a general anesthetic and positioned either prone (face down) or supine (on your back) depending on surgeon preference. Under fluoroscopy and ultrasound guidance, a needle is passed through the flank skin into the renal collecting system. The tract is then dilated up to 24–30 French (about 8–10 mm). A rigid nephroscope passes through this sheath directly into the kidney, and a powerful laser or ultrasonic lithotripter fragments the stone. Pieces are extracted through the working sheath. A nephrostomy drain may be left for 24 hours, and a stent or ureteral catheter is usually placed.
Who PCNL Is For
- Kidney stones larger than 20 mm (about ⅘ inch) — the AUA cut-off where PCNL beats RIRS for stone clearance
- Staghorn stones filling the renal pelvis and calyces
- Hard cystine or brushite stones that resist laser fragmentation by RIRS
- Failed RIRS or ESWL where the stone burden is still significant
Mini-PCNL and Micro-PCNL
The standard PCNL tract is around 24–30 French. Mini-PCNL uses a smaller tract (14–20 French) for moderate-sized stones, and micro-PCNL goes even smaller. Smaller tracts mean less bleeding and faster recovery, but slower stone clearance. For stones in the 1.5–2 cm range, mini-PCNL is increasingly an alternative to RIRS depending on stone position and density [6].
PCNL Stone-Free Rates
For large kidney stones, PCNL achieves stone-free rates of 85–95% in a single session, far higher than RIRS for the same stone burden. The trade-off is a small (around 4–8%) risk of bleeding requiring transfusion, a small risk of pleural injury for upper-pole punctures, and a 1–3 night hospital stay [7].
RIRS (Flexible Ureteroscopy): Going Up to the Kidney Without a Wound
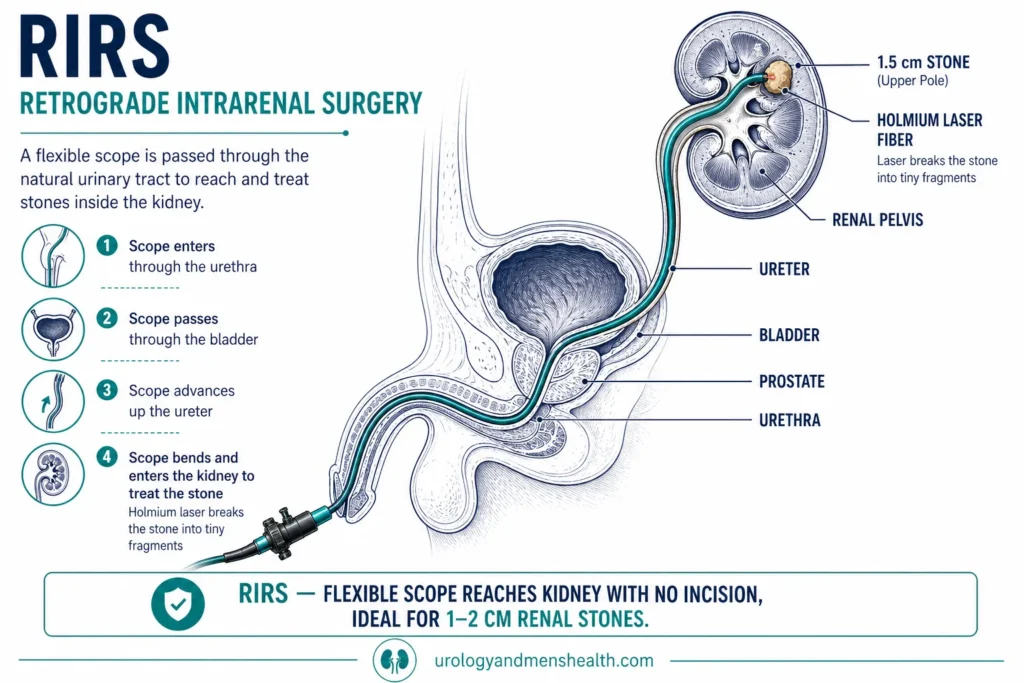
RIRS — retrograde intrarenal surgery — is what I reach for when the stone is inside the kidney itself, between 1 cm and 2 cm, and the patient wants to avoid an incision. The flexible ureteroscope is a feat of modern engineering: a 2.5 mm scope that can curve up to 270 degrees inside the renal collecting system, reaching every calyx of the kidney from below.
How RIRS Works
Under general anesthetic, a flexible ureteroscope is passed up through the urethra and bladder, through the ureter, and into the renal pelvis. Often a thin plastic sheath called a ureteral access sheath (UAS) is positioned in the upper ureter first to make scope passage easier and protect the ureter. The holmium laser fragments the stone into dust (“dusting” technique) or small pieces that can be removed with a basket. A stent is placed at the end [8].
Who RIRS Is For
- Kidney stones between 1 cm and 2 cm in any calyx
- Lower-pole calyx stones where ESWL fragments may not pass downhill against gravity
- Patients on blood thinners who cannot have a flank puncture
- Bilateral stones where both sides can be treated in one anesthetic in selected cases
- Stones in solitary kidneys where every gram of renal tissue matters and PCNL bleeding risk is unacceptable
RIRS Stone-Free Rates
For renal stones up to 2 cm, RIRS achieves around 80–90% stone-free rates after a single procedure. Some patients require a second-look RIRS to clear residual fragments — this is planned, not a failure. The trade-off versus PCNL is a slightly lower stone-free rate per session, balanced against zero skin incision and lower bleeding risk [9].
→ Related Read: Types of Kidney Stones — Which One Do You Have?ESWL Mentioned in Passing — Why It Didn’t Make This List
Patients often ask why I have not included ESWL — extracorporeal shockwave lithotripsy — alongside the three surgical procedures. The answer is that ESWL is not a surgery. It is a non-invasive treatment where focused shockwaves are aimed from outside the body at the stone, fragmenting it without any instrument entering the patient.
ESWL has its place — particularly for kidney stones under 1 cm in patients with normal anatomy and a stone in a favourable location (renal pelvis or upper calyx). But it has lower success rates than the three surgeries above, especially for lower-pole stones, dense stones, or larger stones, and it often needs to be repeated. I treat ESWL as a separate option that competes with RIRS for small kidney stones, not as a substitute for URS or PCNL [10].
Preparing for urological surgery? Download Dr. Khalid’s Urology Surgery Recovery Guide.
Enter your email below to receive Dr. Khalid’s complete Urology Surgery Recovery Guide as a free, printable PDF.
Recovery, Stents, and Time Off Work
Recovery is the part patients consistently underestimate. The procedure itself is a few hours; the stent that follows is the part that bothers people most.
Hospital Stay
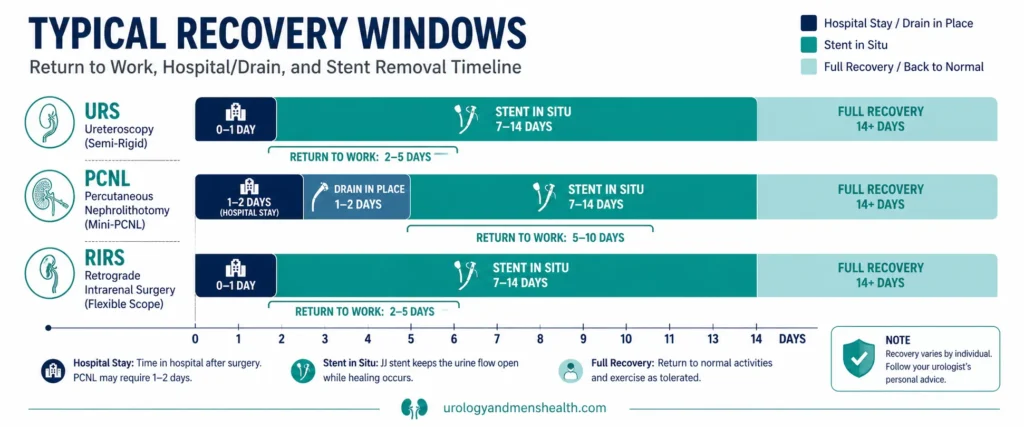
- URS: day-case or 1 night, depending on operating operating room time of day and how you wake from anesthesia
- RIRS: day-case or 1 night for similar reasons
- PCNL: 1–3 nights, with a nephrostomy drain in for the first 24 hours in many cases
Return to Work
- Office or sedentary work: URS and RIRS, 2–5 days. PCNL, 5–10 days.
- Manual or heavy-lifting work: URS and RIRS, 5–7 days. PCNL, 2–3 weeks.
- Driving: not until you can perform an emergency stop without pain — usually 48 hours after URS/RIRS, 5–7 days after PCNL.
The Stent
A double-J ureteral stent stays in for 7–14 days after most URS and RIRS, and after most PCNL cases. It is a soft tube with a curl at each end, sitting between kidney and bladder. About half of patients describe noticeable symptoms — urinary frequency, urgency, mild flank discomfort with a full bladder, and occasional pink urine. These symptoms vanish within 24 hours of stent removal. Stent removal itself takes 30 seconds in clinic with a flexible cystoscope.
→ Related Read: Ureteric Stent Removal — Pain, Process, and What to ExpectRisks, Complications, and What to Ask Your Surgeon
Every surgery has risks. The honest list for the three kidney stone surgery types is below. Most are uncommon; none are catastrophic in the hands of an experienced endourologist.
URS Risks
- Ureteric injury or perforation: 1–2%. Usually managed by leaving a stent and monitoring.
- Post-op urinary tract infection: 5–10%, reduced by pre-op urine culture and prophylactic antibiotics.
- Stent symptoms: 50% experience some discomfort while the stent is in.
- Failed access: 2–5% — the ureter is too narrow on the day, requiring a stent for 1–2 weeks then a second attempt.
PCNL Risks
- Bleeding requiring transfusion: 4–8%, higher in patients with multiple tracts or large stones.
- Post-op fever or sepsis: 5–10%, despite prophylactic antibiotics and pre-op urine clearance.
- Pleural injury (upper-pole punctures): 1–3%, may require a chest drain.
- Adjacent organ injury (colon, spleen, liver): under 1% with image guidance.
RIRS Risks
- Ureteric injury from access sheath: 1–4%. Most are minor abrasions that heal with stent in situ.
- Post-op infection: 5–10%.
- Stent symptoms: as for URS.
- Residual fragments needing second-look RIRS: 10–20%, depending on stone burden at the start.
Questions to Ask Your Surgeon
- How many of these procedures do you perform per year? (For PCNL specifically, look for 50+ per year as a quality marker.)
- What is your stone-free rate at one session for my stone size and location?
- Will I need a stent? For how long?
- What is the realistic chance of needing a second procedure?
- If complications occur, what is your team’s plan?
⚠️ When to Go to the ER After Stone Surgery
- Fever above 38.5°C (101.3°F) — possible urosepsis, needs IV antibiotics urgently
- Heavy red blood in urine soaking through the sheets, not just pink
- Severe flank pain unresponsive to your prescribed pain medication
- Inability to pass urine for more than 6 hours
- Chest pain or shortness of breath after PCNL — possible pleural complication
How I Decide in Clinic: A Real Decision Framework
Here is the actual mental algorithm I run when a patient sits in front of me with a stone on their CT scan. It is not a substitute for a clinical consultation, but it tells you what your surgeon is thinking.
Step 1 — Where Is the Stone?
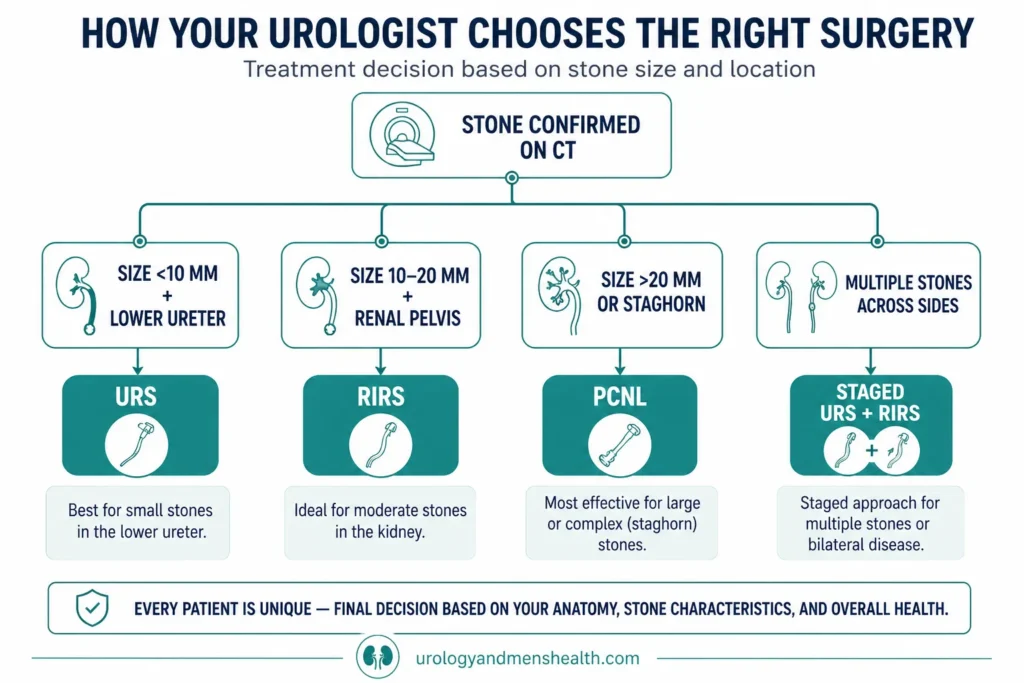
If the stone is in the ureter (the tube), the answer is almost always URS. If the stone is inside the kidney itself, I move to Step 2.
Step 2 — How Big Is the Stone?
- Under 10 mm (under ⅖ inch): ESWL or RIRS. I lean RIRS for lower-pole stones, ESWL for upper-pole stones in slim patients.
- 10–20 mm (⅖–⅘ inch): RIRS first-line, mini-PCNL alternative.
- Over 20 mm (⅘ inch): PCNL is the AUA-recommended first-line procedure.
- Staghorn: PCNL, often as a staged or multi-tract procedure.
Step 3 — Patient-Specific Factors
- Blood thinners that cannot be stopped → URS or RIRS over PCNL
- Solitary kidney → RIRS over PCNL where possible
- Severe obesity → PCNL approach may need to be modified, but is still feasible
- Pregnancy → temporising stent only; definitive surgery deferred unless emergency
- Concurrent infection → drain first (stent or nephrostomy), surgery later when urine is sterile
Step 4 — Patient Preference
When two procedures are clinically reasonable — for example, RIRS versus mini-PCNL for a 1.8 cm renal pelvis stone — I let the patient choose after explaining trade-offs. Some patients want the highest single-session stone-free rate and accept a flank puncture. Others want zero skin incision and accept a second procedure if needed. Both are valid.
→ Related Read: Kidney Stone Size Chart — When You Can Wait and When You Need SurgeryFrequently Asked Questions
Which kidney stone surgery type is the most painful afterwards?
PCNL has more flank discomfort for the first 48–72 hours because of the small puncture wound and the muscle the sheath passed through. URS and RIRS have less wound pain — most discomfort comes from the ureteral stent rather than the surgery itself. Across all three procedures, the stent is what patients complain about most, not the operation. Read more about stent pain and what helps.
How long does a kidney stone surgery take?
URS for a single stone takes 30–60 minutes of operating room time. RIRS is usually 60–90 minutes. PCNL is 90–180 minutes depending on stone burden, with multi-tract or staghorn cases sometimes longer. These are operating times — total time in hospital for day-case URS and RIRS is around 4–6 hours including anesthetic recovery. PCNL involves an overnight stay or longer.
Will I be stone-free after one operation?
For ureteral stones treated by URS, yes in 85–95% of cases. For renal stones treated by RIRS, single-session stone-free rates are around 80–90% and a planned second-look procedure may be needed for residual fragments. For large kidney stones over 2 cm treated by PCNL, single-session stone-free rates are 85–95%. Your surgeon should give you a realistic estimate based on your specific imaging.
Can I avoid surgery and just pass the stone naturally?
Stones under 5 mm pass spontaneously about 70–80% of the time. Stones between 5 and 10 mm pass about 40–50% of the time, often with help from medical expulsive therapy (tamsulosin). Stones over 10 mm rarely pass without intervention and are likely to need one of these kidney stone surgery types. The decision depends on size, location, your pain, kidney function, and how long the stone has been stuck.
Is PCNL considered open surgery?
No. PCNL is minimally invasive — the only incision is a 1 cm puncture in the flank, which heals with a small scar. Open kidney stone surgery (open pyelolithotomy or open nephrolithotomy) is now rare and reserved for very unusual anatomy or failed endoscopic procedures. If you have been told you need open surgery for a stone, get a second opinion from a urologist who performs PCNL and RIRS regularly.
How soon after stone surgery can I fly?
For URS and RIRS, short-haul flights are usually safe after 48–72 hours and long-haul after 1 week, provided you are off opioid pain relief and the stent is comfortable. For PCNL, wait 1–2 weeks for short-haul and 2 weeks for long-haul. Always check with your surgeon, especially if you are still on a stent — read our full flying after kidney stone surgery guide.
📚 References
- Assimos D, Krambeck A, Miller NL, et al. Surgical Management of Stones: American Urological Association/Endourological Society Guideline. J Urol. 2016;196(4):1153-1160. AUA Guidelines
- Türk C, Petřík A, Sarica K, et al. EAU Guidelines on Interventional Treatment for Urolithiasis. Eur Urol. 2016;69(3):475-482. EAU Guidelines
- Geraghty RM, Jones P, Somani BK. Worldwide trends of urinary stone disease treatment over the last two decades: a systematic review. J Endourol. 2017;31(6):547-556. PubMed
- American Urological Association. Surgical Management of Stones — AUA/Endourological Society Guideline (2016, amended 2023). AUA. AUA Guidelines
- Ghani KR, Andonian S, Bultitude M, et al. Percutaneous Nephrolithotomy: Update, Trends, and Future Directions. Eur Urol. 2016;70(2):382-396. PubMed
- Ruhayel Y, Tepeler A, Dabestani S, et al. Tract Sizes in Miniaturized Percutaneous Nephrolithotomy: A Systematic Review from the EAU Urolithiasis Guidelines Panel. Eur Urol. 2017;72(2):220-235. PubMed
- Seitz C, Desai M, Häcker A, et al. Incidence, Prevention, and Management of Complications Following Percutaneous Nephrolitholapaxy. Eur Urol. 2012;61(1):146-158. PubMed
- De S, Autorino R, Kim FJ, et al. Percutaneous Nephrolithotomy Versus Retrograde Intrarenal Surgery: A Systematic Review and Meta-analysis. Eur Urol. 2015;67(1):125-137. PubMed
- Aboumarzouk OM, Monga M, Kata SG, Traxer O, Somani BK. Flexible ureteroscopy and laser lithotripsy for stones >2 cm: a systematic review and meta-analysis. J Endourol. 2012;26(10):1257-1263. PubMed
- Srisubat A, Potisat S, Lojanapiwat B, Setthawong V, Laopaiboon M. Extracorporeal shock wave lithotripsy (ESWL) versus percutaneous nephrolithotomy (PCNL) or retrograde intrarenal surgery (RIRS) for kidney stones. Cochrane Database Syst Rev. 2014;(11):CD007044. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.