Your kidneys filter approximately 180 liters of blood every single day (about 47 gallons). They do this through a network of roughly one million microscopic filters called glomeruli. These tiny knots of blood vessels are incredibly delicate. When subjected to sustained force, the link between high blood pressure and kidney damage becomes dangerously clear: the excess pressure gradually shreds these microscopic filters apart. And the terrifying part? You feel absolutely nothing while it happens.
By the time most patients notice symptoms — swollen ankles, fatigue, foamy urine — they have already lost 50% or more of their kidney function. That damage is permanent. I see this regularly in clinic: a man presents with a urological complaint, I check his labs, and his creatinine reveals chronic kidney disease that nobody has mentioned to him before. When I trace it back, the culprit is almost always the same — years of poorly controlled or completely undiagnosed hypertension.
Hypertension is the second leading cause of end-stage kidney disease worldwide, behind only diabetes [1]. Yet most patients with high blood pressure have no idea their kidneys are at risk. This article explains exactly how the damage happens, what tests detect it early, and what you can do right now to stop the progression — because once kidney tissue is scarred, it does not regenerate.
Key Takeaways
- Hypertension is the second leading cause of kidney failure — behind diabetes, it silently destroys the kidney’s filtration units (glomeruli) over years without symptoms [1]
- The relationship is bidirectional — high BP damages kidneys, and damaged kidneys raise BP further, creating a vicious cycle called nephrosclerosis
- The earliest warning sign is microalbuminuria (tiny amounts of protein leaking into urine) — detectable years before creatinine rises or symptoms appear
- eGFR below 60 for three or more months means chronic kidney disease — yet most patients with this result have never been told
- ACE inhibitors and ARBs are the first-line medications because they protect the kidney’s filtration barrier beyond just lowering BP [2]
- Keeping BP consistently below 130/80 mmHg slows kidney decline by up to 50% compared to less aggressive targets [3]
- Kidney damage from BP is irreversible once scarring occurs — early detection and aggressive treatment are the only strategies that work
In This Guide:
How High Blood Pressure Destroys Your Kidneys — The Mechanism
To understand why hypertension is so dangerous to your kidneys, you need to understand the glomerulus — the kidney’s microscopic filtration unit. Think of each glomerulus as a tiny coffee filter made of blood vessels. Blood enters under pressure, waste products and excess fluid pass through, and clean blood exits on the other side.
The key word here is pressure. These filters are designed to operate within a narrow pressure range. When your systemic blood pressure is chronically elevated — even moderately — the excess force is transmitted directly into these delicate capillary beds. Over months and years, this sustained pressure causes three specific types of damage:
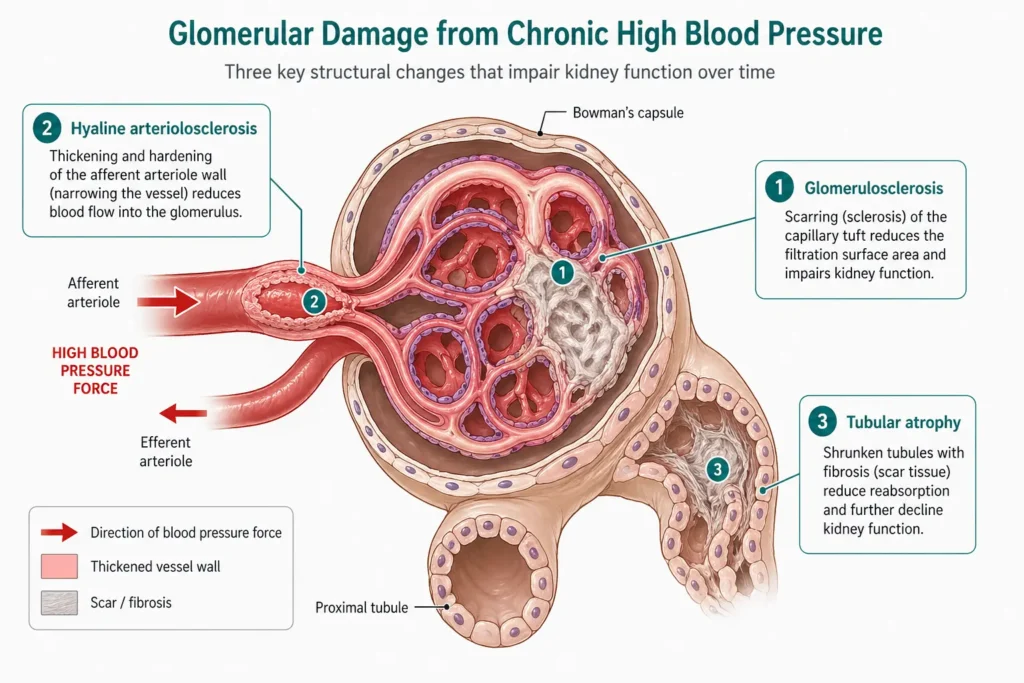
1. Glomerulosclerosis — scarring of the filters
The high-pressure blood flow physically damages the inner lining (endothelium) of the glomerular capillaries. The body responds with inflammation and scarring — a process called glomerulosclerosis. Once a glomerulus scars over, it stops filtering permanently. You cannot grow new ones. Each kidney starts with roughly 500,000 glomeruli, and you lose them progressively with uncontrolled hypertension [4].
2. Arteriolar thickening — narrowed supply pipes
The small arteries feeding each glomerulus (afferent arterioles) respond to chronic high pressure by thickening their walls — a protective adaptation called hyaline arteriolosclerosis. While this initially shields the downstream capillaries, it ultimately reduces blood flow to the kidney tissue, causing ischemic damage. The kidney slowly starves of oxygen and nutrients.
3. Tubular atrophy and interstitial fibrosis
As glomeruli fail and blood supply diminishes, the kidney tubules — the structures that fine-tune urine composition — atrophy and are replaced by scar tissue. This is the final, irreversible stage. On imaging, the kidney physically shrinks. On blood tests, creatinine rises and eGFR falls. By this point, the damage is extensive and permanent.
This entire process is called hypertensive nephrosclerosis, and it is responsible for approximately 25–30% of all cases of end-stage renal disease requiring dialysis or transplant in Western countries [1]. In South Asian populations, where hypertension prevalence exceeds 30% and awareness is lower, the proportion is likely even higher.
→ Related Read: Best Home Blood Pressure Monitors for Men — A Doctor’s Review 2026The Vicious Cycle: Why It Gets Worse Without Treatment
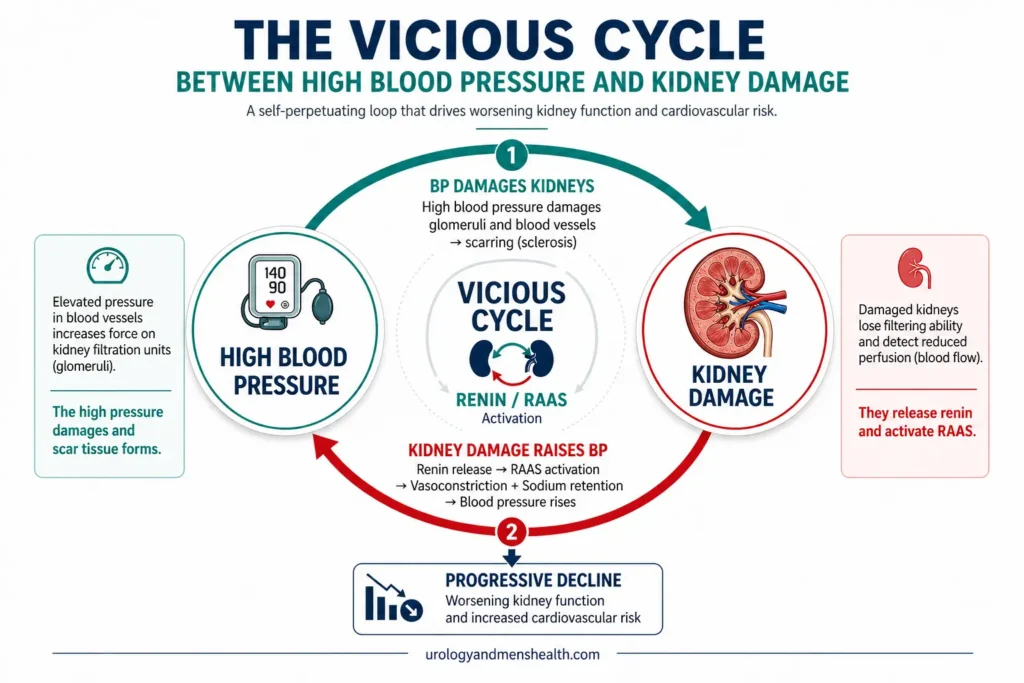
Here is the part that makes hypertensive kidney disease particularly dangerous: the relationship between high blood pressure and kidney damage is bidirectional. High BP damages kidneys — but damaged kidneys also raise blood pressure. This creates a self-amplifying feedback loop that accelerates decline on both fronts.
The mechanism works like this: as kidney function deteriorates, the kidneys lose their ability to excrete sodium and water efficiently. Fluid accumulates, blood volume increases, and blood pressure rises further. Simultaneously, the damaged kidney releases excess renin — an enzyme that activates the renin-angiotensin-aldosterone system (RAAS), causing vasoconstriction and even more sodium retention [5]. The result is a patient whose blood pressure becomes progressively harder to control, requiring more medications at higher doses, while kidney function continues to decline.
This is why I emphasize to patients that controlling blood pressure is not just about preventing heart attacks and strokes — although those are critical. It is about preserving the organ that regulates your blood pressure in the first place. Lose your kidneys, and your blood pressure becomes almost unmanageable.
→ Related Read: Renal Hypertension — When Your Kidneys Are Secretly Raising Your BPWho Is at Risk? The Patients I Worry About Most
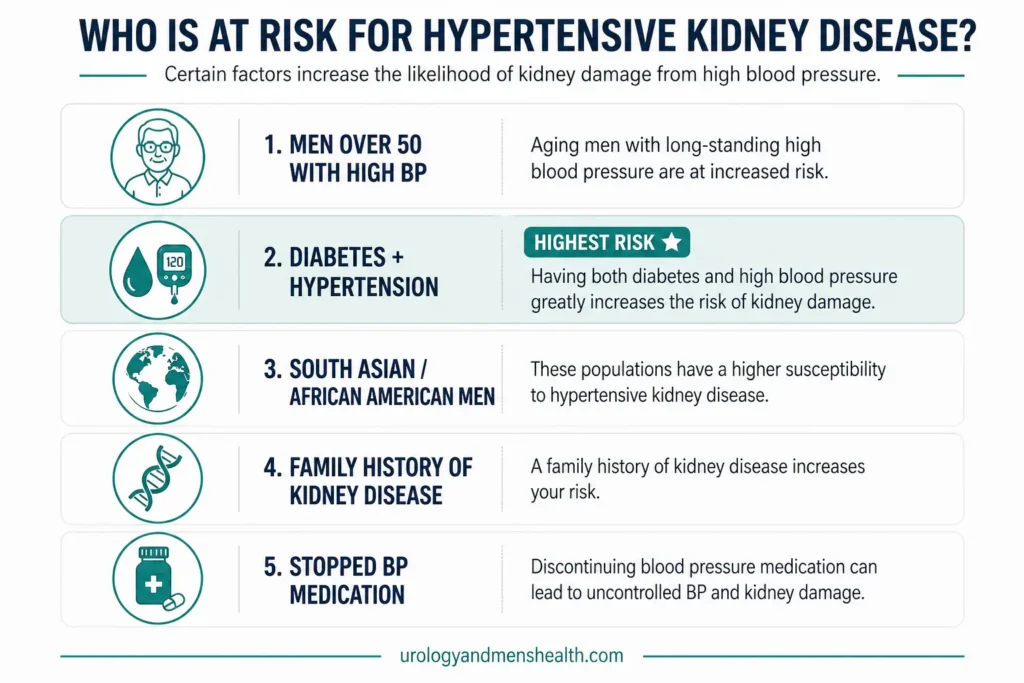
Every person with uncontrolled hypertension is at risk of kidney damage. But certain groups progress faster and need more aggressive monitoring:
- Men over 50 with BP above 140/90 — the combination of age-related nephron loss and hypertension accelerates decline. Men also tend to have lower rates of BP medication adherence than women [6]
- Patients with diabetes AND hypertension — this is the highest-risk combination. Approximately 40% of diabetic patients develop CKD, and the majority have coexisting hypertension [7]
- South Asian and African American men — both populations have higher rates of hypertension, earlier onset, and greater target-organ damage at equivalent BP levels [8]
- Patients with a family history of kidney disease — genetic susceptibility to hypertensive nephrosclerosis exists and is under-recognized
- Patients who have stopped their BP medication — they felt fine, so they stopped. By the time symptoms appear, years of damage have already occurred
The Warning Signs — What to Watch For (and What Your Doctor Should Be Testing)
The cruel reality of hypertensive kidney disease is that it is largely asymptomatic until late stages. You cannot feel your kidneys losing function. There is no pain signal. The damage accumulates silently, which is exactly why screening is critical.
Early signs (often missed)
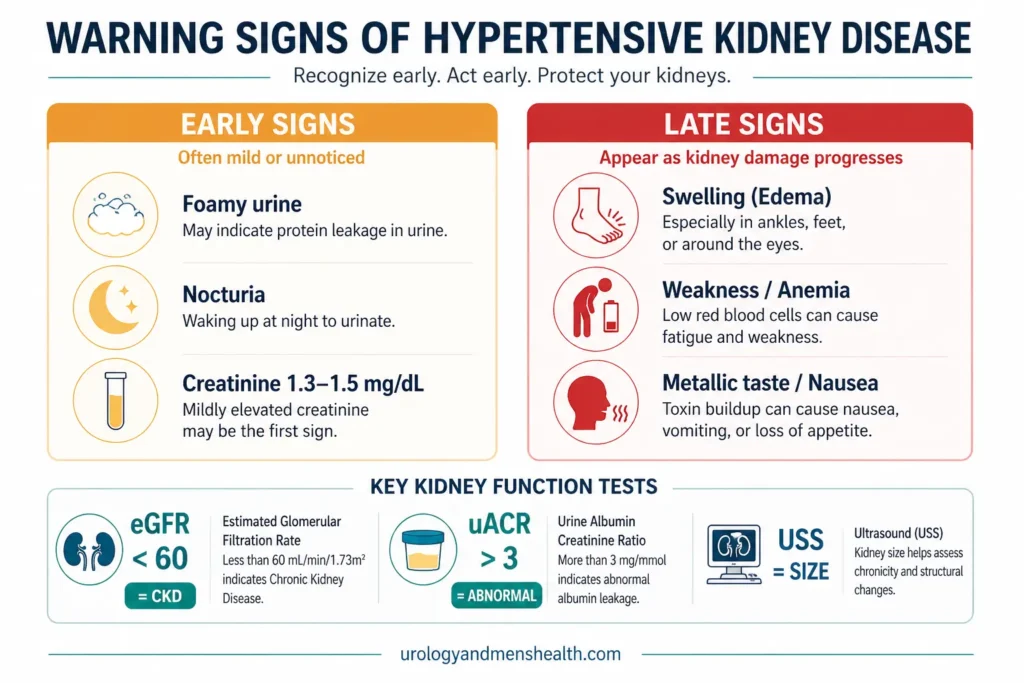
- Foamy or frothy urine — this suggests protein leaking through damaged glomeruli (proteinuria). If your urine consistently foams like beer when it hits the bowl, get it checked
- Nocturia — waking more than once at night to urinate can be an early sign of impaired kidney concentrating ability, not just an enlarged prostate
- Mildly elevated creatinine on routine labs — often flagged as “slightly high” and ignored. A creatinine of 1.3–1.5 mg/dL in a man who previously had 1.0 represents a significant decline
Late signs (damage already advanced)
- Ankle and facial swelling — fluid retention from failing kidneys
- Persistent fatigue and weakness — anemia from reduced erythropoietin production
- Nausea, poor appetite, metallic taste — uremic symptoms from waste accumulation
- Itching (pruritus) — phosphate accumulation in advanced CKD
- Breathlessness — fluid overload and metabolic acidosis
The three kidney function tests that detect damage early
Every patient with hypertension should have these three tests done at least annually:
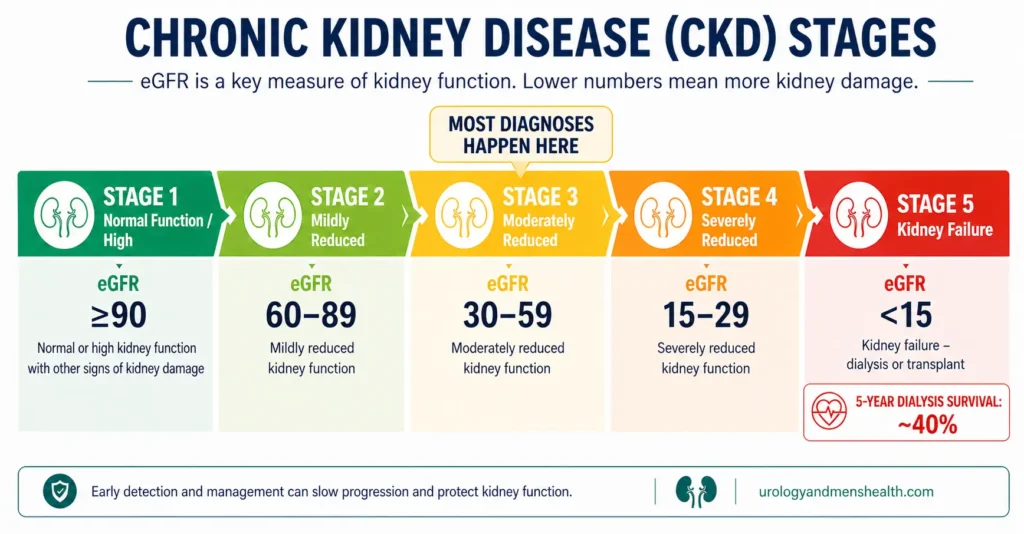
- Serum creatinine and eGFR — eGFR below 60 for three months or more means CKD. Below 15 means kidney failure. Your primary care doctor should track this over time, not just check if it’s “in range”
- Urine albumin-to-creatinine ratio (uACR) — detects microalbuminuria, the earliest marker of glomerular damage, years before creatinine rises [9]. A result above 3 mg/mmol is abnormal. This test is inexpensive and non-invasive
- Renal ultrasound — assesses kidney size and cortical thickness. A size difference between the two kidneys raises suspicion for renal artery stenosis
High blood pressure and worried about your kidneys? Download Dr. Khalid’s Blood Pressure & Kidney Protection Guide.
Enter your email below to receive Dr. Khalid’s complete Blood Pressure & Kidney Protection Guide as a free, printable PDF.
How to Protect Your Kidneys: The Evidence-Based Strategy
The good news is that hypertensive kidney damage is largely preventable — and if caught early, its progression can be dramatically slowed. The strategy involves two parallel approaches: aggressive blood pressure control and kidney-specific protective measures.
Blood pressure targets for kidney protection
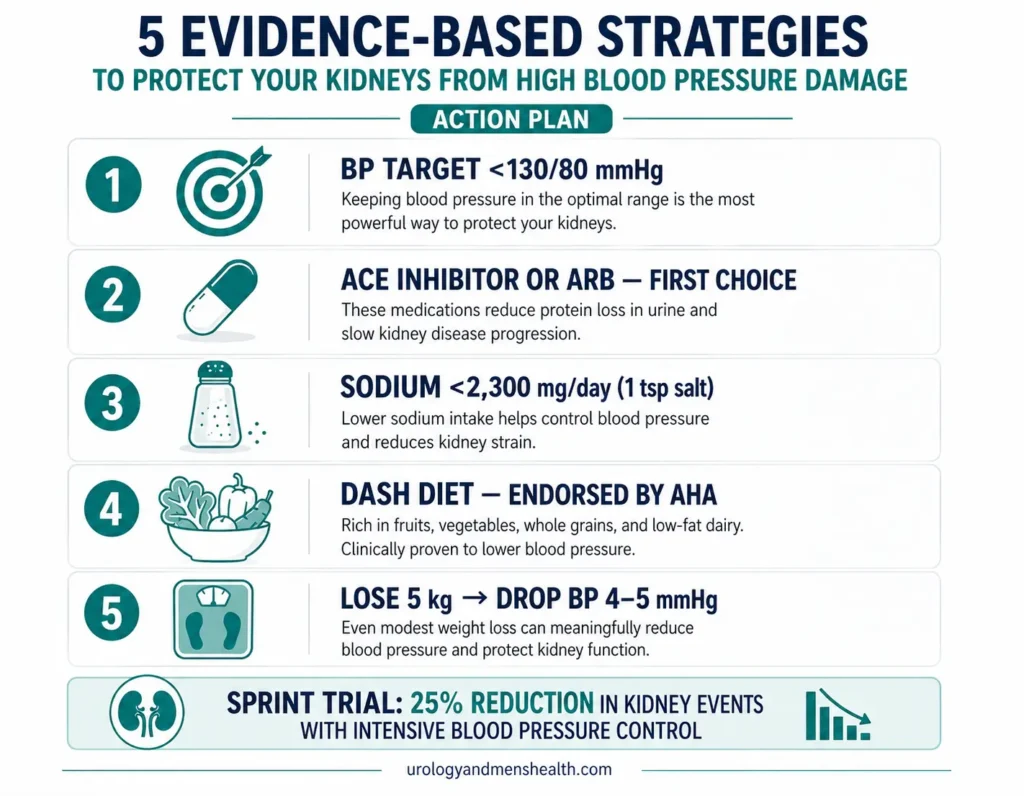
The current evidence — from the SPRINT trial and updated KDIGO 2021 guidelines — supports a target of below 130/80 mmHg for patients with CKD or high cardiovascular risk [3]. The SPRINT trial demonstrated that intensive BP lowering reduced the composite kidney outcome by approximately 25% compared to standard targets [10].
For patients who already have significant proteinuria (uACR above 30), some guidelines recommend even tighter systolic targets — below 120 mmHg — provided the patient tolerates it without postural hypotension.
Why ACE inhibitors and ARBs are the first choice
Not all blood pressure medications protect the kidneys equally. ACE inhibitors (ramipril, enalapril, lisinopril) and ARBs (losartan, valsartan, candesartan) are the gold standard because they reduce intraglomerular pressure — something no other antihypertensive class does [2].
Here is the analogy I use in clinic: imagine your glomerulus is a garden hose with a nozzle. Angiotensin II tightens the nozzle, raising the pressure inside the hose even if the tap pressure hasn’t changed. ACE inhibitors and ARBs relax that nozzle, protecting the delicate capillary walls from further damage.
The landmark RENAAL and IDNT trials showed that ARBs reduced the risk of doubling of serum creatinine by 25% and end-stage renal disease by 20% in diabetic nephropathy [11]. These drugs are not optional — they are the foundation of kidney-protective therapy.
Important caution: ACE inhibitors and ARBs can initially raise creatinine by 10–20% — this is expected and acceptable. A rise above 30% may indicate renal artery stenosis. Never stop these medications because of a small creatinine bump without discussing it with your doctor.
Lifestyle measures that genuinely matter
- Sodium restriction below 2,300 mg/day (about 1 teaspoon of salt) — high sodium raises BP and undermines ACE inhibitor/ARB effectiveness
- The DASH diet — reduces systolic BP by 8–14 mmHg, equivalent to a single medication [12]. Endorsed by the American Heart Association
- Weight loss — every 5 kg (about 11 lbs) lost reduces systolic BP by approximately 4–5 mmHg
- Regular exercise — 150 minutes per week of moderate aerobic activity reduces BP by 5–8 mmHg
- Moderate alcohol and no smoking — smoking accelerates renal artery atherosclerosis
What Happens When Treatment Is Too Late — The Renal Endgame
I include this section not to frighten you, but because understanding the consequences of inaction is one of the most powerful motivators for treatment adherence. I have seen too many patients who stopped their medication because they “felt fine” and returned years later in kidney failure.
When eGFR drops below 15 ml/min — Stage 5 CKD — you are in end-stage renal disease. Your options at that point are:
- Hemodialysis — three sessions per week, each lasting 3–4 hours, profoundly impacting quality of life, employment, travel, and relationships
- Peritoneal dialysis — can be done at home but requires daily exchanges and meticulous infection control
- Kidney transplant — the best long-term option, but limited by donor availability, surgical risk, and lifelong immunosuppression
The five-year survival rate on dialysis is approximately 40% [13] — worse than many cancers. Every year on dialysis costs healthcare systems tens of thousands of dollars. All of this is potentially preventable with a low-cost blood test and a daily tablet.
Special Considerations: NSAIDs, Supplements, and Nephrotoxins
If you have hypertension — controlled or not — these common substances are particularly dangerous to your kidneys:
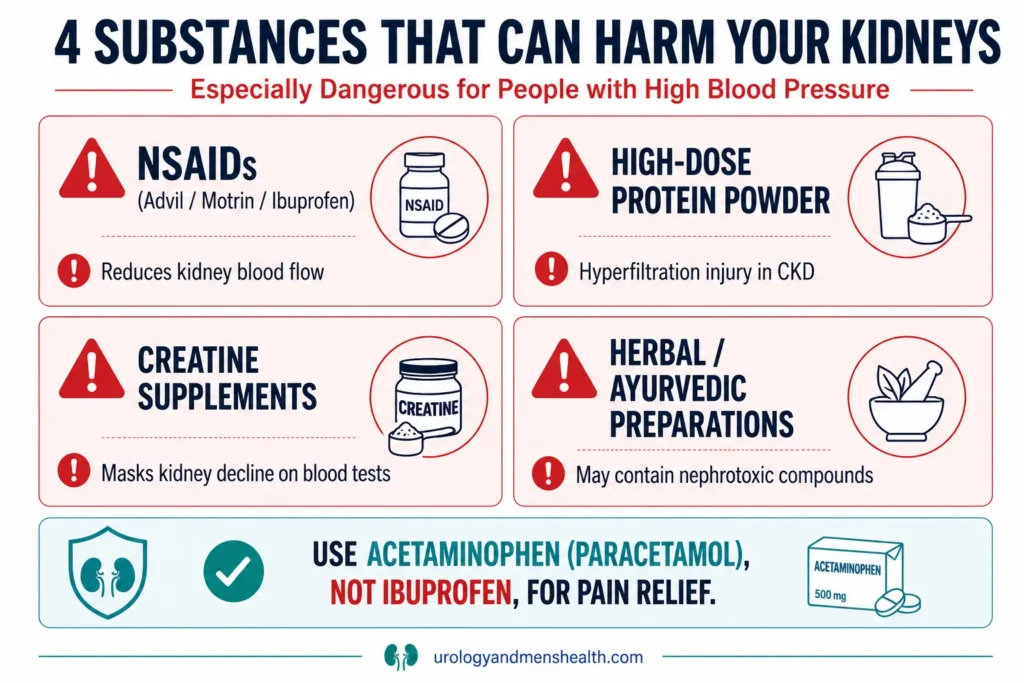
- NSAIDs (ibuprofen [sold in the US as Advil, Motrin], diclofenac, naproxen) — reduce blood flow to the kidneys by inhibiting prostaglandin-mediated vasodilation. Chronic use in a hypertensive patient accelerates kidney damage. Use acetaminophen (paracetamol) instead whenever possible
- High-dose protein supplements — if you already have reduced eGFR, excessive protein intake causes hyperfiltration injury. Keep intake to 0.8 g/kg/day in CKD stages 3–5
- Creatine supplements — raises serum creatinine and can mask kidney function decline on blood tests, creating diagnostic confusion in borderline patients
- Herbal and ayurvedic preparations — some contain heavy metals or nephrotoxic compounds. Always disclose all supplements to your doctor
💡 In My Practice
The scenario I encounter most frequently is a man presenting with a urological complaint — BPH symptoms, a kidney stone, or hematuria — in whom routine blood work reveals a creatinine of 1.6 or 1.8 mg/dL and an eGFR in the low 40s. When I ask about his blood pressure history, he invariably tells me it was “a little high” several years ago, he was given a tablet, he felt fine and stopped it. That gap — sometimes five years, sometimes a decade — is where the damage happened silently. By the time I see him, no intervention I can offer will restore what has been lost. The stone or the prostate is almost secondary at that point.
I have also found that telling patients their blood pressure is high rarely motivates sustained behavior change. What does motivate them is framing kidney failure concretely: “If your kidneys fail, you will spend three mornings every week for the rest of your life connected to a dialysis machine — unable to travel freely, unable to work normally, and with a survival rate worse than most cancers.” When I explain it that way, most patients leave the consultation with a very different relationship to their antihypertensive tablet.
In Pakistan, I saw a significant number of patients with end-stage renal disease who had had detectable hypertension for years — often managed intermittently, with medication started and stopped as their symptoms fluctuated. Many patients associated medications with permanent illness and stopped them once their blood pressure “normalized” on treatment, not understanding that the normalization was caused by the medication itself. I spend considerable time on this point in clinic because it is not a failure of intelligence — it is a failure of explanation.
On lab interpretation: I never just tell patients their eGFR is “borderline.” I explain it as a percentage of kidney function remaining. An eGFR of 45 means roughly 45% of normal kidney function. That framing makes the number real and urgent in a way that “stage 3a CKD” simply does not.
Regarding uACR: in my practice I now routinely check it in hypertensive patients presenting for any urological complaint. In perhaps one in four of these patients, I find a result above 3 mg/mmol that their primary care doctor has never checked. In several cases, this has led to earlier introduction of an ACE inhibitor and a nephrology referral delayed by years. It is a three-minute, low-cost test that changes management.
⚠️ When to See a Doctor — Urgently
- Sudden severe headache with BP above 180/120 — hypertensive emergency. Go to the emergency room (ER) immediately. Malignant hypertension can cause acute kidney injury within hours
- Foamy urine persisting for more than a few days — suggests significant proteinuria, warrants urgent uACR testing
- New ankle or facial swelling — may indicate fluid retention from declining kidney function
- Rising creatinine on blood tests — any upward trend should be investigated, not dismissed as “borderline”
- BP requiring 3+ medications and still above target — resistant hypertension may indicate renal artery stenosis
- Sudden reduction in urine output below 500 ml/day (about 17 fl oz) — medical emergency suggesting acute kidney injury
Frequently Asked Questions
Can kidney damage from high blood pressure be reversed?
Unfortunately, no — once kidney tissue is scarred (fibrosed), it cannot regenerate. However, the damage can be stabilized and its progression dramatically slowed with aggressive blood pressure control, ACE inhibitors or ARBs, and lifestyle modification. The critical point is catching it early — before eGFR drops below 30. See our CKD stages guide for what each eGFR range means in practice.
What blood pressure level starts damaging kidneys?
There is no precise threshold — damage exists on a continuum. Sustained readings above 140/90 mmHg are clearly associated with progressive kidney decline. The 2021 KDIGO guidelines recommend treating to below 130/80 mmHg for kidney protection [10]. Occasional spikes during exercise or stress are normal and do not cause chronic damage. Use the BP & Kidney Risk Assessment to see where your numbers put you.
I have high blood pressure but normal creatinine — are my kidneys safe?
Not necessarily. Creatinine is a late marker — it does not rise significantly until roughly 50% of kidney function is already lost. The earlier marker is urine albumin-to-creatinine ratio (uACR), which can detect glomerular damage years before creatinine changes. Ask your primary care doctor to check uACR as part of your annual hypertension review. Read more in our guide to kidney function tests explained.
Can I take ibuprofen if I have high blood pressure?
You should avoid it whenever possible. NSAIDs like ibuprofen (Advil, Motrin) reduce blood flow to the kidneys and can raise blood pressure by 3–5 mmHg. In patients already taking ACE inhibitors or ARBs, adding an NSAID creates a “triple whammy” with increased risk of acute kidney injury — especially if a diuretic is also involved [14]. Use acetaminophen (paracetamol) as your first-line pain reliever instead.
Does drinking more water help protect kidneys from blood pressure damage?
Adequate hydration matters for general kidney health, but water intake alone does not prevent hypertensive nephrosclerosis. The damage is caused by mechanical pressure on the glomerular capillaries, not by insufficient fluid. Aim for 2–2.5 liters of fluid daily (68–85 fl oz, roughly 8–10 cups), but understand that blood pressure control is far more impactful than hydration for this specific problem. Track your daily intake with the Hydration Calculator.
📚 References
- Udani S, Lazich I, Bakris GL. Epidemiology of hypertensive kidney disease. Nat Rev Nephrol. 2011;7(1):11–21. PubMed
- Lewis EJ, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345(12):851–860. PubMed
- KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney Int. 2021;99(3S):S1–S87. KDIGO Guidelines
- Hughson MD, et al. Hypertension, glomerular number, and birth weight in African Americans and white subjects in the southeastern United States. Kidney Int. 2006;69(4):671–678. PubMed
- Taal MW, Brenner BM. Renoprotective benefits of RAS inhibition: from ACEI to angiotensin II antagonists. Kidney Int. 2000;57(5):1803–1817. PubMed
- Corrao G, et al. Gender and age differences in the persistence with antihypertensive medication. J Hum Hypertens. 2011;25(8):484–491. PubMed
- Afkarian M, et al. Kidney disease and increased mortality risk in type 2 diabetes. J Am Soc Nephrol. 2013;24(2):302–308. PubMed
- Agyemang C, et al. Ethnic disparities in hypertension in Europe. J Hypertens. 2019;37(5):909–920. PubMed
- Lamb EJ, et al. Kidney function tests and interpretation. BMJ. 2006;333(7572):733–737. PubMed
- SPRINT Research Group. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103–2116. PubMed
- Brenner BM, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy (RENAAL). N Engl J Med. 2001;345(12):861–869. PubMed
- Sacks FM, et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. N Engl J Med. 2001;344(1):3–10. PubMed
- UK Renal Registry 25th Annual Report. 2023. UK Kidney Association. UK Kidney Association
- Dreischulte T, et al. Combined use of nonsteroidal anti-inflammatory drugs with diuretics and/or renin-angiotensin system inhibitors and risk of acute kidney injury. BMJ. 2015;350:h785. PubMed

Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.