Enlarged Prostate Treatment Options: BPH Meds vs Surgery
Patients usually endure waking up all night and struggling to pee, writing it off as just an unavoidable part of getting older. The truth is, ignoring an enlarged prostate or staying on failing pills doesn't just ruin your sleep—it can permanently damage your bladder. Here is the complete clinical pathway, explaining exactly when to step away from medication and what your surgical options actually look like today.

If you are looking at enlarged prostate treatment options, you have probably already crossed the line where this stopped being a minor annoyance. Maybe you are getting up twice a night to urinate, waiting at the toilet for the stream to start, and finishing with a dribble that needs an extra minute of patience. Maybe you have been on a tablet for months and things are not improving — or worse, they have started slipping back.
Benign prostatic hyperplasia (BPH) — overgrowth of the prostate gland that is not cancer — affects roughly 50% of men by age 60 and up to 90% by age 85 [1]. It can degrade quality of life, disrupt sleep, and in severe cases damage the bladder and kidneys. The progression from “mild annoyance” to “I need something done about this” is gradual, which is exactly why many men wait too long.
As a urologist who manages BPH daily — from first prescriptions to operating room — I am going to walk you through the complete treatment pathway: what medications do, when they stop working, and what your surgical options actually look like in 2026.
📋 Key Takeaways
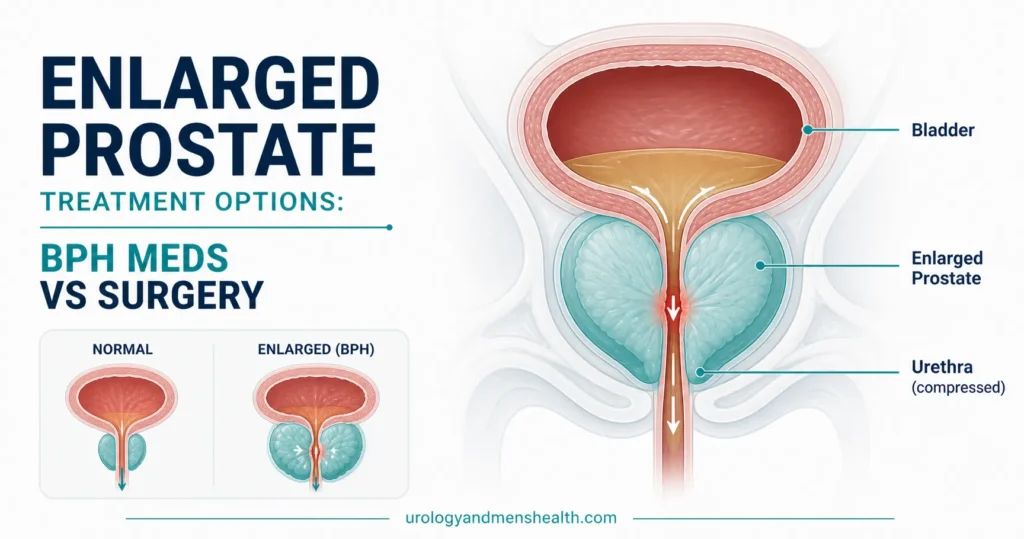
- BPH is NOT cancer — it is benign overgrowth of prostate tissue that squeezes the urethra and obstructs urine flow.
- Alpha-blockers (tamsulosin) work within days and are first-line, but they do not shrink the prostate — they only relax the surrounding muscle.
- 5-alpha reductase inhibitors (finasteride/dutasteride) actually shrink the prostate by 20–30% but take 6–12 months and can cause sexual side effects.
- Surgery becomes the answer when medications fail, symptoms worsen, or complications develop (retention, recurrent UTIs, bladder stones, kidney damage).
- TURP remains the reference standard, but laser procedures (HoLEP, GreenLight) offer lower bleeding risk and shorter hospital stays.
- Retrograde ejaculation (semen entering the bladder at orgasm) occurs in 65–75% after TURP — this must be discussed honestly before surgery.
In This Guide:
Understanding BPH: What’s Actually Happening Inside
Your prostate sits just below your bladder, wrapped around the urethra like a ring around a pipe. Starting in your 40s, the central zone of the prostate begins to grow — slowly, silently, and in virtually all men. This growth is driven by dihydrotestosterone (DHT), a potent derivative of testosterone produced by the enzyme 5-alpha reductase within the prostate.
As the prostate enlarges, it compresses the urethra from the outside, creating resistance to urine flow. Your bladder compensates by working harder — the muscle wall thickens (detrusor hypertrophy), generating higher pressures to push urine through the narrowing channel. This compensation works for a while, which is why symptoms develop gradually rather than suddenly.
Eventually, the bladder muscle becomes overworked and begins to fail. That is when incomplete emptying, overflow incontinence, and in the worst cases, bilateral hydronephrosis (backpressure damaging both kidneys) develop. This cascade — from minor nuisance to organ damage — can take years or decades, but it is progressive in a significant proportion of men [2].
The symptoms — what men actually experience
Urologists categorize BPH symptoms into two groups:
Storage symptoms (irritative — the ones that bother men most):
- Nocturia — waking 2+ times per night to urinate. Usually the symptom that finally drives men to seek help, because it destroys sleep quality.
- Urgency — a sudden, compelling need to urinate that is difficult to defer.
- Frequency — urinating more than 8 times during the day.
- Urge incontinence — leaking before reaching the toilet.
Voiding symptoms (obstructive — the classic BPH signs):
- Weak stream — reduced force and caliber of the urinary stream.
- Hesitancy — waiting or straining to start urination.
- Intermittency — stream stops and starts during voiding.
- Terminal dribbling — a slow trickle at the end.
- Incomplete emptying — feeling like the bladder did not fully empty.
- Straining — using abdominal pressure to push urine out.
We quantify symptom severity using the International Prostate Symptom Score (IPSS) — a standardized 7-question tool scored 0–35. Mild: 0–7. Moderate: 8–19. Severe: 20–35. This score is tracked over time and is one of the main factors in deciding when to escalate treatment [3].
→ Take the IPSS Quiz: 5 Minutes to Score Your BPH SeverityStage 1: Medication — Your First Enlarged Prostate Treatment Options
Most men with moderate BPH symptoms start with medication. There are two main drug classes, and understanding what each one actually does — and does not do — is critical for setting realistic expectations.
Alpha-blockers: the quick relief option
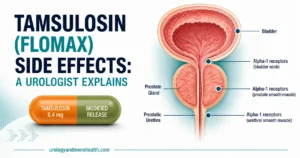
Drugs: Tamsulosin (Flomax), alfuzosin, silodosin, doxazosin, terazosin.
How they work: The prostate and bladder neck contain smooth muscle with alpha-1 adrenergic receptors. Alpha-blockers relax this muscle, reducing the dynamic (muscular) component of obstruction. They widen the channel without shrinking the prostate itself.
Onset: Symptom improvement within 48 hours to 2 weeks — the fastest-acting BPH treatment.
Effectiveness: Improve IPSS by 4–6 points on average. Increase peak flow rate by 2–3 mL/sec [4]. Very effective for mild-to-moderate symptoms.
Side effects to know about:
- Dizziness and orthostatic hypotension — especially with doxazosin and terazosin (non-selective). Tamsulosin is more prostate-selective and causes less blood pressure drop.
- Retrograde ejaculation — semen goes backward into the bladder instead of forward. Occurs in about 10% with tamsulosin. Harmless but surprising if not warned.
- Intraoperative floppy iris syndrome (IFIS) — if you need cataract surgery while on tamsulosin, tell your ophthalmologist. This is important and frequently missed.
- Nasal congestion — minor but common.
If you are already on tamsulosin and want a side-by-side breakdown of every common side effect — including the cataract issue — read my dedicated piece on tamsulosin side effects in men, or use the BPH medication side-effect checker to map your symptoms against your prescription.
The limitation: Alpha-blockers do not stop prostate growth. They treat the symptom (obstruction) but not the disease (enlargement). Over time, as the prostate continues to grow, alpha-blockers become insufficient. They also do not reduce the risk of acute urinary retention or the need for future surgery.
5-alpha reductase inhibitors (5-ARIs): the slow shrinkage option
Drugs: Finasteride (Proscar) and dutasteride (Avodart).
How they work: Block the conversion of testosterone to DHT — the hormone that drives prostate growth. Over 6–12 months, this actually shrinks the prostate by 20–30% [5].
Onset: Slow. Meaningful symptom improvement takes 3–6 months. Maximum effect at 12 months. This is the main reason patients abandon them — they expect the speed of tamsulosin and get frustrated.
Effectiveness: Reduce IPSS by 3–4 points. Reduce prostate volume by 20–30%. Crucially, reduce the risk of acute urinary retention by 57% and the need for surgery by 55% over 4 years — something alpha-blockers cannot do [5].
Side effects — the honest conversation:
- Erectile dysfunction — reported in 5–8% of men. Usually reversible on stopping the drug, though rare cases of persistent sexual dysfunction after discontinuation have been reported.
- Decreased libido — 3–6%.
- Reduced ejaculate volume — common.
- Gynecomastia (breast enlargement/tenderness) — rare but documented.
- PSA reduction — finasteride/dutasteride halve your PSA value. Your doctor must know you are taking these, otherwise a “normal” PSA could mask an elevated true value. Rule of thumb: multiply your PSA by 2 if you are on a 5-ARI.
These sexual side effects are real, and they must be discussed honestly before prescribing. Most men tolerate 5-ARIs well, but the minority who develop ED or loss of libido are understandably distressed — especially if they were not warned.
Combination therapy: when one drug isn’t enough
For men with moderate-to-severe symptoms AND a significantly enlarged prostate (over 40 grams on ultrasound — roughly the size of a walnut crossed with a small plum), combination therapy with an alpha-blocker plus a 5-ARI is more effective than either alone. The landmark CombAT trial demonstrated that combination therapy reduced the risk of symptom progression by 41% compared to tamsulosin alone over 4 years [6].
If you do not know your prostate size yet, the prostate volume calculator turns the three measurements on your ultrasound report into a single grams figure — useful for understanding whether combination therapy is even on the table for you.
The trade-off is a higher side effect burden — you get the side effects of both drug classes. For this reason, combination therapy is reserved for men with genuinely large prostates who are at high risk of progression, not for mild symptoms.
→ Related Read: My PSA is 4.5 — Do I Have Cancer? Understanding Grey Zone ResultsWhen Medication Fails: The 7 Signs It’s Time for Surgery
This is the question I get asked most often, and there is no single universal answer — it depends on symptom severity, quality of life impact, and the presence of complications. Surgery should be seriously considered when:
- Acute urinary retention — you physically cannot urinate and require a catheter. If this happens more than once despite adequate medication, surgery is strongly indicated.
- Recurrent urinary tract infections — caused by a chronically elevated post-void residual (urine left in the bladder after voiding). Stagnant urine breeds bacteria.
- Bladder stones — form in stagnant residual urine. Their presence means the obstruction is significant enough to alter bladder chemistry.
- Renal impairment — elevated creatinine with bilateral hydronephrosis on ultrasound means backpressure from the obstruction is damaging your kidneys. This is an urgent indication.
- Recurrent gross hematuria — bleeding from engorged prostatic blood vessels that does not settle with conservative measures.
- Medication failure — symptoms persist or worsen despite optimized combination therapy for 6–12 months.
- Quality of life — subjective but valid. If nocturia is destroying your sleep, if you cannot sit through a meeting without needing the toilet, if you are planning your life around bathroom access — that is reason enough if medication is not working.
The first five are absolute indications — surgery is recommended regardless of patient preference. The last two are relative indications where the decision is shared between you and your urologist based on how much the symptoms affect your life.
→ Use the BPH Treatment Finder to Map Your Symptoms to a PathwayDownload Your Free Clinical Action Plan
Enter your email below to download Dr. Khalid’s complete BPH & Prostate Screening Guide as a free, printable PDF.
The Surgical Options: A Urologist’s Honest Comparison
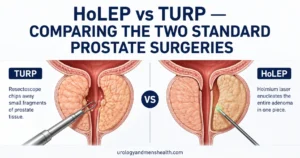
TURP (Transurethral Resection of the Prostate) — the reference standard
TURP has been the reference standard for BPH surgery for over 80 years. A resectoscope is passed through the urethra (no external incisions), and the obstructing prostate tissue is shaved away using an electrically heated wire loop. The chips of tissue are irrigated out and sent for histological analysis.
- Best for: Prostate volume 30–80 mL (about 1–2.7 fl oz of tissue — the majority of BPH cases).
- Success rate: 85–90% symptom improvement. Peak flow rate typically doubles or triples.
- Hospital stay: 1–3 days with a catheter for 24–48 hours.
- Recovery: Full recovery 4–6 weeks. Avoid heavy lifting and straining during this period.
- Durability: Long-term results are excellent. Re-treatment rate approximately 1–2% per year [7].
Side effects of TURP:
- Retrograde ejaculation: 65–75% — the most common side effect. Semen enters the bladder during orgasm instead of being expelled externally. Orgasm sensation is preserved in most men, but there is no visible ejaculate. This is permanent and must be discussed before surgery.
- Erectile dysfunction: 5–10% — often temporary, related to thermal or electrical injury near the neurovascular bundles.
- Urinary incontinence: 1–3% — usually mild and temporary. Severe permanent incontinence is rare (under 1%).
- Bleeding requiring transfusion: 2–5% — higher with larger prostates.
- TUR syndrome: Rare with modern bipolar TURP (uses saline irrigation). Was more common with older monopolar technique.
- Urethral stricture: 2–5% — narrowing of the urethra from instrumentation, may require dilation.
HoLEP (Holmium Laser Enucleation of the Prostate) — the modern challenger
HoLEP uses a holmium laser to enucleate (shell out) entire lobes of the prostate from within, rather than shaving tissue piece by piece like TURP. The enucleated tissue is pushed into the bladder, morcellated (cut into fragments), and removed.
- Best for: Any prostate size — including very large prostates (over 80–100 mL / about 2.7–3.4 fl oz of tissue) where TURP becomes risky. HoLEP is size-independent, which is its biggest advantage.
- Success rate: Equivalent to or better than TURP for symptom relief.
- Hospital stay: Often shorter than TURP — many centers discharge within 24 hours.
- Bleeding risk: Significantly lower than TURP — the laser cauterizes as it cuts. Suitable for men on anticoagulants.
- Durability: Excellent — re-treatment rate is very low because the adenoma is completely removed, not just debulked.
The catch: HoLEP has a steep surgical learning curve — a urologist needs approximately 50 cases to become proficient [8]. Not all centers offer it, and outcomes are highly surgeon-dependent. If your urologist performs HoLEP regularly, it is an excellent option. If they have done fewer than 20 cases, consider traveling to a high-volume center.
Side effects are similar to TURP — retrograde ejaculation (75–80%), ED (5–10%), incontinence (temporary stress incontinence more common initially than TURP but usually resolves within 3 months).
GreenLight (PVP — Photoselective Vaporization of the Prostate)
Uses a high-powered KTP or LBO laser to vaporize prostate tissue on contact, creating an immediate channel.
- Best for: Small to medium prostates (30–80 mL). Men on anticoagulants (lowest bleeding risk of all surgical options).
- Advantages: Very low bleeding risk, often same-day discharge, shorter catheter time.
- Disadvantages: No tissue specimen for histology (tissue is vaporized, not removed). Slightly higher re-treatment rate compared to TURP and HoLEP. Can cause irritative voiding symptoms for several weeks post-operatively.
Newer minimally invasive therapies (MISTs) — for ejaculatory preservation
Several newer procedures aim to preserve ejaculatory function — a major concern for sexually active men:
- UroLift (prostatic urethral lift): Small implants hold the enlarged lobes apart, like curtain tie-backs. Preserves ejaculation in most men. Best for small-to-moderate prostates without a median lobe. Re-treatment rates of 13.6% at 5 years [9].
- Rezūm (water vapor therapy): Steam is injected into the prostate, causing targeted cell death and shrinkage over weeks. Preserves ejaculation in most. Takes 2–4 weeks for symptom improvement.
- Aquablation: Robot-guided waterjet ablation using ultrasound mapping. Shows promise for larger prostates with lower retrograde ejaculation rates than TURP. Still relatively new with limited long-term data.
These MISTs fill a niche for men who need more than medication but want to preserve ejaculatory function. They are not equivalent to TURP or HoLEP for severe obstruction, and their long-term durability is still being established.
Open prostatectomy (simple prostatectomy)
Reserved for very large prostates (over 80–100 mL) in centers where HoLEP is not available. An abdominal incision is made and the adenoma is shelled out by hand. Highly effective but carries higher morbidity — longer hospital stay (3–5 days), more bleeding, longer recovery. Increasingly being replaced by HoLEP and robotic-assisted simple prostatectomy.
→ Related Read: Prostate Cancer Screening — The Age-by-Age Guide Every Man NeedsWhat to Expect After Prostate Surgery
Recovery after TURP or laser prostate surgery follows a predictable pattern, but patients are often surprised by some aspects:
- Week 1–2: Catheter removed (usually 24–48 hours post-op). Urination may burn initially. Urine may be blood-tinged — this is normal and can last 2–4 weeks. Drink plenty of fluids — aim for 2–2.5 liters per day (about 70–85 fl oz / 8–10 cups) — to keep urine dilute.
- Week 2–4: Frequency and urgency often temporarily worsen before they improve. This is counterintuitive and alarms many patients, but it happens because the raw prostatic bed is healing and the bladder is readjusting to lower resistance.
- Week 4–6: Stream should be noticeably stronger. Nocturia improving. Most men can return to normal activity. Avoid heavy lifting (over 10 kg / about 22 lb) until cleared by your surgeon.
- Month 3: Full benefit is usually apparent by this point. IPSS should be significantly lower than pre-surgery.
- Long-term: Annual follow-up with flow rate and residual volume measurement. PSA monitoring continues — BPH surgery does NOT eliminate the need for prostate cancer screening.
💡 In My Practice
The most common pattern I see is a man in his early 60s who has been on tamsulosin for 2–3 years. It worked well initially, but over the past year his nocturia has crept back to 3–4 times per night, his stream has weakened again, and ultrasound shows a rising post-void residual. His prostate has continued growing despite the alpha-blocker. This is the classic moment we have the surgery conversation.
The biggest barrier to timely surgery in my experience is fear — specifically, fear of incontinence and impotence. When I explain that the actual risk of permanent incontinence after TURP is under 1%, and that ED risk is 5–10% (and often temporary), most men are surprised. They had imagined much worse. The conversation about retrograde ejaculation needs more careful handling — for sexually active men, the idea of a “dry orgasm” is genuinely distressing, and I always discuss UroLift or Rezūm specifically for men who tell me ejaculation preservation is a priority.
What I want more patients to understand: if you wait until you are in acute retention with a catheter in the emergency room, you have already developed bladder damage that may not fully recover even after successful surgery. The men who do best are those who have surgery while the bladder still has good contractile function — not after years of overdistension have compromised it.
⚠️ When to See a Doctor — Urgently
Go to the emergency room immediately for:
- Complete inability to urinate (acute urinary retention) — a catheter will be placed to drain the bladder, and you will be referred to urology for definitive management.
- Visible blood in urine (hematuria) — especially with clots. May indicate prostatic bleeding or the need to exclude bladder cancer.
- Fever with urinary symptoms — may indicate UTI secondary to incomplete emptying, or acute prostatitis.
- Pain in the lower back or flanks with reduced urine output — may suggest bilateral obstruction affecting the kidneys (hydronephrosis).
See your primary care doctor or urologist (non-urgent appointment) if:
- You are getting up 2+ times per night to urinate regularly.
- Your stream has become noticeably weaker over months.
- You feel your bladder does not empty completely.
- BPH medications that once worked are becoming less effective.
- You are taking tamsulosin and you need cataract surgery (intraoperative floppy iris syndrome risk — tell your ophthalmologist).
Frequently Asked Questions
What are the main enlarged prostate treatment options?
Enlarged prostate treatment options fall into three tiers. First-line is medication: alpha-blockers (tamsulosin, alfuzosin, silodosin) for fast relief, plus 5-alpha reductase inhibitors (finasteride, dutasteride) to actually shrink the prostate. Second-line is minimally invasive procedures (UroLift, Rezūm) for men who want to preserve ejaculation. Third-line is definitive surgery — TURP, HoLEP, or GreenLight laser. The right choice depends on your symptom severity, prostate size, and whether you have developed complications. The BPH treatment finder can help you map your situation to a pathway.
Does BPH increase my risk of prostate cancer?
No. BPH and prostate cancer are separate conditions. Having an enlarged prostate does not increase your cancer risk. However, both conditions become more common with age and can coexist. BPH can elevate PSA levels, which complicates cancer screening — this is why PSA interpretation requires urological expertise, not just a number on a lab report. If you are in the diagnostic grey zone, my PSA grey zone guide walks through what the numbers actually mean.
Can I take tamsulosin forever?
You can take it long-term, and many men do for years. However, it does not prevent disease progression. If your symptoms are well-controlled, your residual volumes are low, and your kidneys are normal, long-term tamsulosin is a reasonable strategy with regular monitoring — annual IPSS, flow rate, and residual volume measurement should all be tracked. If side effects become bothersome, the BPH medication side-effect checker can help you decide whether to discuss a switch with your urologist.
Can I avoid BPH surgery permanently?
Possibly, but not always. Roughly half of men with moderate symptoms manage their BPH with medication for many years without ever needing surgery. The men who can most reliably avoid surgery are those with prostates under 40 grams, low residual volumes, and stable IPSS scores on combination therapy. The men who cannot avoid it are those with progressive disease — rising residuals, recurrent retention, bladder stones, or kidney damage. Lifestyle changes (limited evening fluids, avoiding decongestants, treating constipation) can help. But if your bladder is failing, no amount of medication will rescue it — surgery is the only intervention that physically removes the obstruction.
Will BPH surgery affect my sex life?
Retrograde ejaculation is the most common sexual change after TURP and HoLEP, occurring in 65–75% of men. Orgasm sensation is usually preserved but there is no visible ejaculate. Erectile function is preserved in 90–95% of men. For men who prioritize ejaculatory preservation, UroLift and Rezūm are alternatives worth discussing — though their symptom relief is generally less dramatic than TURP for moderate-to-severe disease.
How do I choose between TURP, HoLEP, and laser surgery for BPH?
In practice, the choice often depends on what your urologist is most experienced with and what equipment is available at your hospital. For prostates under 80 mL, TURP, HoLEP, and GreenLight all produce excellent results. For very large prostates (over 80–100 mL), HoLEP or open prostatectomy are preferred. Ask your surgeon how many of each procedure they have performed — surgical volume correlates strongly with outcomes. The prostate volume calculator will give you a starting figure if you have an ultrasound report.
Can BPH come back after surgery?
Regrowth is possible but uncommon. After TURP, the re-treatment rate is approximately 1–2% per year. After HoLEP, it is even lower because the entire adenoma is removed. If symptoms recur years after surgery, the cause may be bladder dysfunction (detrusor failure) rather than prostatic regrowth — urodynamic assessment is needed to differentiate.
📚 References
- Berry SJ, Coffey DS, Walsh PC, Ewing LL. The development of human benign prostatic hyperplasia with age. J Urol. 1984;132(3):474–479. PubMed
- Speakman MJ, Kirby RS, Joyce A, Abrams P, Pocock R. Lower urinary tract symptoms suggestive of benign prostatic hyperplasia: more than treating symptoms? Eur Urol Suppl. 2008;7(11):680–689. DOI
- Barry MJ, Fowler FJ Jr, O’Leary MP, et al. The American Urological Association symptom index for benign prostatic hyperplasia. J Urol. 1992;148(5):1549–1557. AUA Journal
- Djavan B, Marberger M. A meta-analysis on the efficacy and tolerability of alpha-1 adrenoceptor antagonists in patients with lower urinary tract symptoms suggestive of benign prostatic obstruction. Eur Urol. 1999;36(1):1–13. PubMed
- McConnell JD, Roehrborn CG, Bautista OM, et al. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003;349(25):2387–2398. NEJM
- Roehrborn CG, Siami P, Barkin J, et al. The effects of combination therapy with dutasteride and tamsulosin on clinical outcomes in men with symptomatic benign prostatic hyperplasia: 4-year results from the CombAT study. Eur Urol. 2010;57(1):123–131. PubMed
- Sandhu JS, Bixler BR, Dahm P, et al. Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia (BPH): AUA guideline amendment 2023. J Urol. 2024. AUA Guidelines
- Elzayat EA, Elhilali MM. Holmium laser enucleation of the prostate (HoLEP): the endourologic alternative to open prostatectomy. Eur Urol. 2006;49(1):87–91. PubMed
- Roehrborn CG, Barkin J, Gange SN, et al. Five year results of the prospective randomized controlled prostatic urethral L.I.F.T. study. Can J Urol. 2017;24(3):8802–8813. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.

Finasteride Side Effects: BPH vs Hair Loss Trade-Offs
HoLEP vs TURP: Which Prostate Surgery Wins? | Urologist
Nocturia in Men: Causes, Diagnosis & Treatment
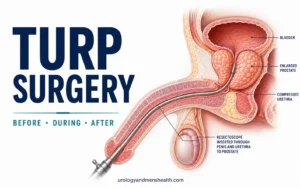
TURP Surgery: What to Expect Before, During & After
TURP surgery — transurethral resection of the prostate — is still the operation most urologists, including me, consider...
Tamsulosin (Flomax) Side Effects: A Urologist Explains
Tamsulosin side effects are something most men only learn about after they have started the medication — usually...