TURP surgery — transurethral resection of the prostate — is still the operation most urologists, including me, consider the benchmark for men whose enlarged prostate is no longer responding to medication. It has been performed for more than 80 years, and despite a wave of newer options like HoLEP, Aquablation, and UroLift, TURP remains the procedure other techniques are measured against. If your urologist has raised TURP with you, you are not being offered something outdated — you are being offered the most clinically validated surgical treatment for benign prostatic hyperplasia (BPH) available today. This guide walks you through exactly what happens before, during, and after the procedure, what the recovery actually feels like, and the side effects every man deserves to hear about before signing the consent form.
Key Takeaways
- TURP removes obstructing prostate tissue through the urethra — there are no external incisions, and most men go home within 2-3 days.
- About 85-90% of men get significant, durable symptom relief — strong urinary stream, fewer night-time trips, and the ability to empty the bladder properly.
- The most common long-term side effect is retrograde ejaculation (semen entering the bladder instead of exiting), which occurs in roughly 65-75% of men and does not affect orgasm or erection.
- Full recovery takes 6-8 weeks. Most men resume desk work at 2-3 weeks and full physical activity at 6 weeks.
- TURP is the right answer when medications have failed, urinary retention has occurred, or prostate volume is between 30-80 mL. Larger glands often suit HoLEP better.
In This Guide:
What TURP Surgery Actually Does
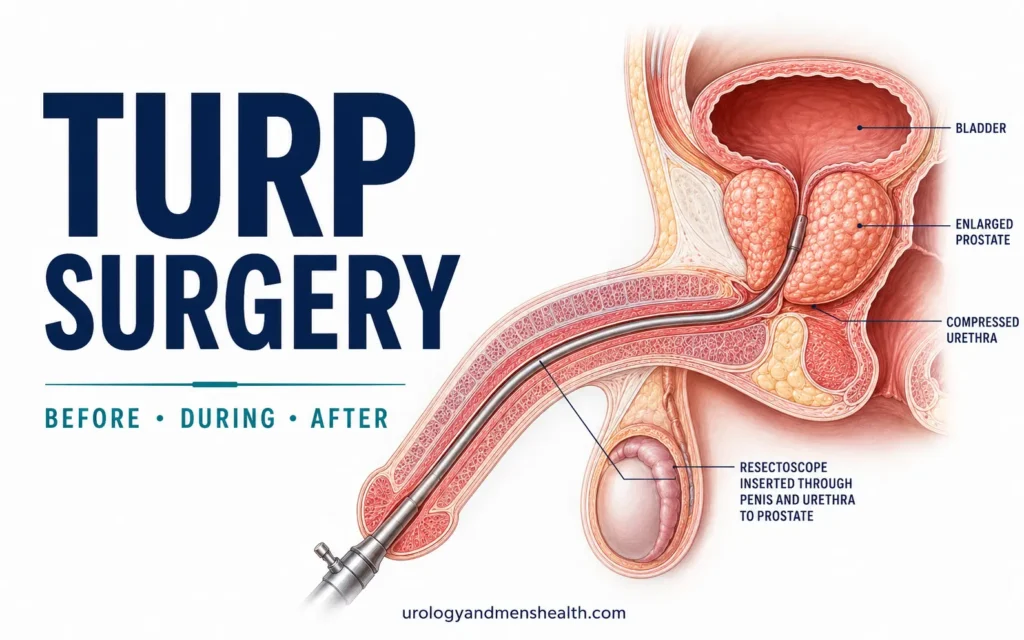
TURP stands for transurethral resection of the prostate. The word “transurethral” is the key: the entire operation happens through the urethra, using a thin instrument called a resectoscope. There are no cuts on your abdomen, no scars, and no opening of the bladder from outside.
The problem TURP solves is mechanical. An enlarged prostate squeezes the urethra running through its centre — imagine a doughnut quietly thickening around a straw. Over time the channel narrows enough that urine cannot pass cleanly, the bladder muscle tires from straining, and symptoms appear: weak stream, hesitancy, dribbling, getting up multiple times at night, sometimes complete inability to pass urine.
During TURP, I pass the resectoscope down the urethra under direct vision. A small electrified wire loop at the tip shaves obstructing prostate tissue away in thin strips, opening the channel back up. The bladder neck and external sphincter — the structures that control continence — are deliberately left alone. The capsule of the prostate, the outer shell, also stays intact. What gets removed is only the inner adenoma — the part that has overgrown and is blocking flow.
The result, when done well, is dramatic. International outcome data show flow rates roughly double after surgery and IPSS symptom scores drop by 15-20 points on average [1]. If you are not sure where you currently sit on that scale, the IPSS Prostate Symptom Score Calculator gives you the same validated score I use in clinic to decide who needs surgery and when.
Who TURP Is Actually For
TURP is not the first treatment anyone with BPH gets. The standard pathway moves through lifestyle changes, then alpha-blockers (like tamsulosin), then 5-alpha-reductase inhibitors (like finasteride), often combined. Surgery becomes the conversation when one or more of the following is true:
- Medications have failed — symptoms remain disruptive after 3-6 months of optimised drug therapy.
- Medication side effects are intolerable — postural dizziness from alpha-blockers, sexual side effects from 5-ARIs, or both. The BPH Medication Side Effect Checker walks through which drug is likely causing which symptom.
- Acute urinary retention has occurred — you have been unable to pass urine at all and needed catheterisation. Once this has happened, the risk of it happening again rises sharply.
- Recurrent UTIs or bladder stones have developed because the bladder cannot empty properly.
- Kidney function is being threatened by high pressure in the bladder backing up to the kidneys (hydronephrosis).
- Visible bleeding from the prostate is recurrent and significant.
The other deciding factor is prostate size. TURP works best for glands between roughly 30 mL and 80 mL. Smaller than that and a minimally invasive option like UroLift or Rezum may be enough; larger than 80 mL and HoLEP or open simple prostatectomy is usually a better fit because resecting that much tissue with the electrocautery loop takes too long and carries more risk. If you want to see how the major techniques compare side by side, the Urology Surgery Comparison Tool lays out the trade-offs by gland size, recovery time, and side-effect profile.
In My Practice
The men I see most often for TURP are not the ones with the worst symptom scores — they are the ones whose lives have quietly shrunk around their bladder. A man stops accepting dinner invitations because he cannot trust himself for three hours without a bathroom. He stops driving long distances. He stops sleeping through the night and starts apologising to his wife at 3 a.m. By the time he sits in my consulting room, he has often spent two or three years adjusting his life around symptoms rather than treating them.
The decision to have TURP is rarely about the symptoms themselves — it is about getting your life back.
Before Surgery: The Workup
Before scheduling TURP, your urologist will confirm three things: that your symptoms really are from BPH (not prostate cancer, urethral stricture, or bladder dysfunction), that your prostate anatomy is suitable for this technique, and that you are fit enough for an anaesthetic.
The standard pre-op workup includes:
- IPSS questionnaire to quantify how bad symptoms currently are.
- Uroflowmetry — you urinate into a special funnel that measures flow rate. A maximum flow under 10 mL/sec strongly suggests obstruction.
- Post-void residual (PVR) ultrasound — a scan checking how much urine is left in the bladder after you urinate. Anything over 100 mL is concerning.
- PSA blood test and digital rectal exam (DRE) to rule out prostate cancer hiding alongside BPH.
- Prostate size measurement — either by transrectal ultrasound or, increasingly, MRI. This is what tells me whether TURP, HoLEP, or another technique is the right fit.
- Urinalysis and culture to make sure you are not going into surgery with an active urinary tract infection.
- Pre-anaesthetic assessment — bloods, ECG, and a review of medications, particularly blood thinners.
Your anticoagulants will need adjusting. Aspirin is usually stopped 7 days before surgery; warfarin, clopidogrel, and direct oral anticoagulants (DOACs) like rivaroxaban or apixaban are managed case by case with your prescribing doctor. Never stop these on your own — the bridging plan matters as much as the stopping date.
You will also be given clear fasting instructions (typically no food after midnight, clear fluids up to 2 hours before) and a date to arrive at the hospital, usually the morning of surgery.
What Happens on the Day of Surgery
You arrive at the hospital fasted. The anaesthetist will discuss two options: spinal anaesthesia, where you are awake but numb from the waist down, or general anaesthesia, where you are fully asleep. Both are safe. Spinal has the advantage of slightly faster recovery and lets the surgeon detect early signs of bladder perforation (which would cause shoulder-tip pain in an awake patient). Most TURPs I do are under spinal.
In theatre, you are positioned with your legs in stirrups. The skin around the genitals is cleaned, sterile drapes are placed, and a single dose of intravenous antibiotic is given. The resectoscope is then passed through the urethra. From this point onward, the entire operation is performed looking at a video monitor.
The resection itself takes between 45 and 90 minutes depending on prostate size. The cut tissue chips collect in the bladder and are flushed out at the end. A three-way urinary catheter is then placed — three-way because one channel drains urine, one inflates the balloon that holds the catheter in place, and the third allows continuous saline irrigation through the bladder to wash out blood and prevent clot formation.
You are then transferred to the recovery ward, then back to your hospital bed. The irrigation continues for 12-24 hours, during which the urine in your catheter bag will look pink to light red. This is expected, not an emergency.
Considering BPH surgery? Get the complete decision guide.
Enter your email below to receive Dr. Khalid’s complete BPH & Prostate Screening Guide as a free, printable PDF — covering when surgery is right, what to ask before consenting, and how to compare TURP with newer options.
The First 48 Hours After TURP
The hospital stay after TURP is typically 2-3 nights. Most of this is to monitor your catheter drainage, manage the irrigation, and give the bladder lining time to settle before the catheter comes out.
What to expect in the first 24 hours:
- Bladder spasms — sudden, cramping urges to urinate even though the catheter is doing it for you. Caused by the catheter balloon irritating the bladder. Usually settle within 24-48 hours and respond well to anticholinergic medications like solifenacin.
- Pink-to-red urine in the catheter bag. As long as it stays the colour of rosé wine or lighter, this is normal. The irrigation rate will be adjusted to maintain that.
- Mild burning at the penis tip from catheter contact. This eases significantly once the catheter is out.
- Need to drink plenty — once the irrigation comes off, you will be encouraged to drink 2-3 litres a day to keep flushing the bladder naturally.
The catheter usually comes out on day 2 or day 3 once the irrigation has been off for several hours and the urine is clear. There is a moment of anxiety here that every patient feels: will I be able to pass urine on my own? In around 90% of men, the answer is yes — within a few hours. About 10% need the catheter back in temporarily because the bladder muscle, which has been straining for years, needs another week or two to recover its strength. This is called a trial without catheter (TWOC) failure. It is inconvenient, not catastrophic.
Once you are urinating reliably, you go home, usually the same day.
The TURP Recovery Timeline
Full recovery from TURP takes 6-8 weeks. The bladder needs time to heal, the resected prostate bed needs to re-line itself with new tissue (a process called re-epithelialisation), and the bladder muscle needs to retrain itself to empty a low-resistance channel after years of pushing against a blockage.
- Week 1: Catheter out. Expect mild burning when urinating, frequency, and urgency. Some men describe it as feeling like a urinary tract infection — it is not, it is the raw prostate bed sending signals. Drink plenty. Avoid heavy lifting and prolonged sitting.
- Weeks 2-3: Symptoms settle steadily. Many men return to office or desk work. Driving is usually safe by day 10-14 once you can perform an emergency stop without hesitation. Sexual activity is best deferred until week 4-6.
- Weeks 4-6: Most men feel close to normal. Urinary stream is noticeably stronger than pre-op. Some men still experience occasional urgency or minor leakage, which continues to improve.
- Weeks 6-8: Full physical activity resumes — cycling, gym work, swimming. The prostate bed has fully re-epithelialised. Final symptom relief is usually achieved by week 12.
A common surprise: a small amount of blood in the urine can appear at week 2-3, often when the scab over the resection bed sheds. This is called secondary haemorrhage and is rarely serious. Increased fluid intake and rest usually settle it within 24-48 hours. If it persists or the urine becomes deep red with clots, contact your surgeon.
A week-by-week breakdown of what to do and what to avoid at each stage is covered in the TURP Recovery Timeline: Week by Week guide.
Side Effects: What You Need to Be Told Before Consenting
Most patient information leaflets undersell TURP side effects. I will not. The information below is what I tell every man before he signs the consent form.
Retrograde Ejaculation (65-75%)
The most common long-term side effect of TURP is retrograde ejaculation. During resection, the bladder neck — the ring of muscle that closes during ejaculation to direct semen forward — is necessarily widened. Afterwards, when you climax, the semen takes the path of least resistance: backwards into the bladder instead of out through the penis. It comes out harmlessly in your next urination, mixed with urine.
This is sometimes called “dry orgasm.” It does not affect the sensation of orgasm and it does not affect erections. It does affect fertility — if you and your partner are still planning to have children, raise this with your urologist before surgery so alternative techniques can be considered.
Erectile Dysfunction (5-10%)
The honest figure for new-onset erectile dysfunction after TURP is around 5-10% [2]. The nerves responsible for erections (the cavernous nerves) run alongside the outside of the prostate capsule and are not directly cut during TURP, but heat from the electrocautery loop can cause some collateral effect. Men who already have borderline erectile function before surgery are most at risk. If this happens, it is usually treatable — the ED treatment protocol covers the step-up approach from oral medications onwards. For a deeper discussion specifically about sexual recovery after prostate surgery, see the sex after prostate surgery guide.
Urinary Incontinence (1-2%)
Permanent stress incontinence — leakage when you cough, sneeze, or lift — is uncommon, occurring in roughly 1-2% of men. It usually reflects damage to the external sphincter during resection, which a careful surgeon avoids. Temporary urgency and urge leakage in the first 4-6 weeks is much more common and almost always settles.
Urethral Stricture (3-5%)
Scar tissue can form in the urethra at the site where the resectoscope passed. If this happens — usually 3-12 months post-op — the symptoms feel like the original BPH coming back: weakening stream, hesitancy. A simple dilatation or, occasionally, a minor procedure called optical urethrotomy resolves it.
Bladder Neck Contracture (2-4%)
Similar to a stricture but located at the bladder neck rather than the urethra. Treated with bladder neck incision in theatre.
Need for Re-treatment (5-15% over 10 years)
TURP results are durable but not permanent. Long-term data show that around 5-15% of men need re-treatment within 10 years, either because regrowth has occurred or because a stricture has developed [1]. This compares favourably to most minimally invasive techniques, where re-treatment rates are higher.
TURP vs HoLEP, Aquablation, and UroLift
The honest answer to “is TURP the best surgery?” is: it depends on your prostate size, your priorities, and what is available where you live.
- HoLEP (Holmium Laser Enucleation): The strongest competitor. Works better than TURP for large prostates (over 80 mL), has less bleeding, shorter catheter time, and equivalent or better long-term outcomes. Side-effect profile (especially retrograde ejaculation) is similar. The main limitation is availability — it requires a urologist trained specifically in the technique.
- Aquablation: A newer water-jet technique that may preserve ejaculatory function better than TURP. Equivalent symptom relief but longer-term data is still maturing. A detailed comparison is in the Aquablation therapy guide.
- UroLift / Rezum: Minimally invasive options that preserve ejaculation almost completely. Best for smaller prostates (under 60 mL) without a middle lobe. Symptom relief is less than TURP and re-treatment rates are higher.
- Simple open prostatectomy: Reserved for very large prostates (over 100 mL) where endoscopic techniques become impractical. Largely being replaced by HoLEP.
The single most important conversation to have with your urologist is: “Given my prostate size, my symptoms, and my sexual function priorities, which of these techniques is the right fit for me?” If retrograde ejaculation matters to you, UroLift or Rezum is worth discussing. If you want maximum durable relief and have a large prostate, HoLEP. For most men with prostates between 30-80 mL where availability of HoLEP is limited, TURP remains the right answer. A detailed head-to-head of the two main techniques is in the HoLEP vs TURP comparison.
When to Call Your Surgeon After TURP
Red Flags After TURP — Act Now
Most post-TURP recovery is uneventful. The following symptoms are not — contact your urological surgeon or attend the emergency room without delay.
- Heavy bright red bleeding with clots that does not clear with increased fluid intake within a few hours, or that prevents you from urinating because clots are blocking the flow.
- Complete inability to pass urine after the catheter has been removed — this is acute urinary retention and needs immediate re-catheterisation.
- Fever above 38°C (100.4°F), particularly with shivering, lower back pain, or burning urination — possible UTI or, more seriously, sepsis.
- Severe lower abdominal pain not relieved by prescribed painkillers.
- Calf pain, swelling, or sudden breathlessness — possible deep vein thrombosis or pulmonary embolism, both more common in the post-op period.
- Chest pain at any point.
A follow-up appointment is typically scheduled at 6 weeks post-op, where your urologist will repeat the IPSS, check a uroflow, and confirm the bladder is emptying properly. Many men are discharged from urological follow-up at that visit, with the option to return if anything changes.
Frequently Asked Questions About TURP Surgery
How long does a TURP procedure take?
The TURP surgery itself usually takes 45 to 90 minutes, depending on the size of the prostate. The whole theatre time, including anaesthesia, positioning, and recovery transfer, is around 2-2.5 hours. Hospital admission to discharge is typically 2-3 nights. If you want to see whether your symptoms warrant surgery in the first place, the IPSS Calculator gives you the same score I use in clinic to make that call.
Will I still be able to ejaculate after TURP surgery?
You will still have orgasms, but in 65-75% of men the ejaculation goes backwards into the bladder instead of out through the penis. This is called retrograde ejaculation. It is harmless, it does not affect the pleasure of orgasm, and the semen passes out in the next urination. It does affect fertility, so if you are still planning children, discuss alternative techniques with your urologist before consenting to TURP.
Is TURP surgery painful?
TURP is performed under spinal or general anaesthesia, so the operation itself is painless. The recovery is uncomfortable rather than severely painful — bladder spasms in the first 24-48 hours, mild burning when urinating for the first week, and occasional urgency for 4-6 weeks. Most men describe the discomfort as manageable with simple painkillers like paracetamol and an anticholinergic for spasms.
How soon after TURP can I go back to work and exercise?
For desk or office work, most men return at 2-3 weeks. For jobs involving heavy lifting, prolonged standing, or driving long distances, allow 4-6 weeks. Light walking is encouraged from day 1 to reduce DVT risk. Avoid cycling, gym work, and swimming until week 6. Sexual activity should be deferred until week 4-6. A detailed schedule is in the TURP recovery timeline.
Does TURP affect erections?
New erectile dysfunction occurs in about 5-10% of men after TURP. The nerves responsible for erections run outside the prostate capsule and are not directly cut, but heat from the resectoscope can cause some collateral effect, particularly in men whose erectile function was already borderline. If ED does develop, it usually responds well to standard oral treatments, as covered in the ED treatment guide.
How long does TURP last before symptoms come back?
TURP results are durable. Long-term studies show 85-90% of men maintain significant symptom relief at 5 years, and around 5-15% need re-treatment within 10 years — usually for prostate regrowth or stricture, not failure of the original surgery. This durability is one of the main reasons TURP remains the benchmark surgical option for BPH.
References
- Cornu JN, Ahyai S, Bachmann A, et al. A Systematic Review and Meta-analysis of Functional Outcomes and Complications Following Transurethral Procedures for Lower Urinary Tract Symptoms Resulting from Benign Prostatic Obstruction. European Urology. 2015;67(6):1066-1096. PubMed
- Reich O, Gratzke C, Bachmann A, et al. Morbidity, Mortality and Early Outcome of Transurethral Resection of the Prostate: A Prospective Multicenter Evaluation of 10,654 Patients. Journal of Urology. 2008;180(1):246-249. PubMed
- American Urological Association. Management of Benign Prostatic Hyperplasia (BPH) Guideline (Amended 2023). AUA Guidelines
- European Association of Urology. Guidelines on the Management of Non-neurogenic Male Lower Urinary Tract Symptoms (LUTS), incl. Benign Prostatic Obstruction (BPO). 2024. EAU Guidelines

Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.