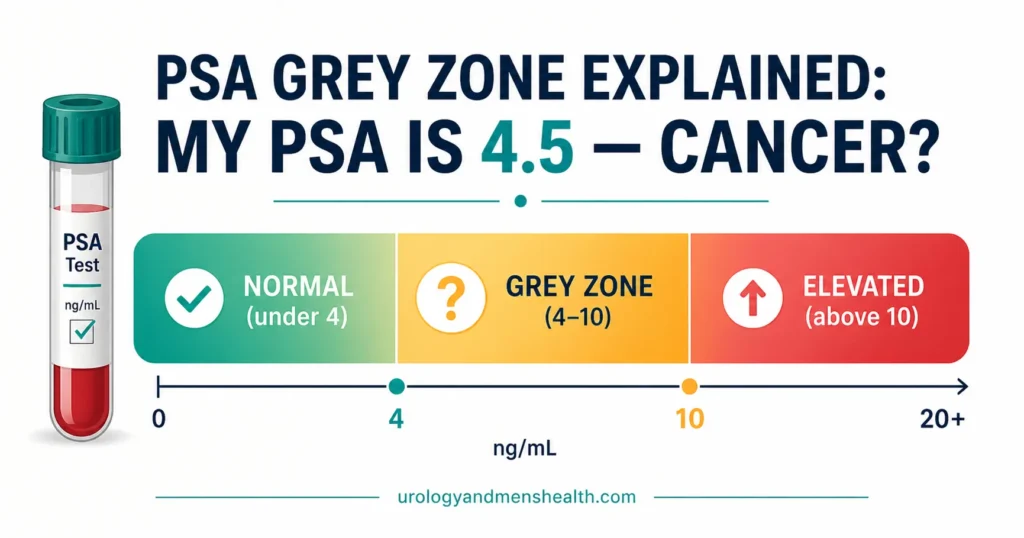
PSA Grey Zone Explained: My PSA is 4.5 — Cancer?
It takes about three minutes of online searching for a patient with a PSA of 4.5 to convince themselves they are facing a grim diagnosis. In my clinic, I spend most of my time explaining that a number between 4 and 10 is not a cancer diagnosis; it is simply a biological flag, and three out of four times, the cause is entirely benign. This guide is the unvarnished conversation you need to have before your urology appointment so you can arrive informed instead of terrified.

Your doctor calls. Your PSA is 4.5. There’s a pause, then: “It’s a bit raised — I’m going to refer you to urology.” You hang up, open Google, type “PSA 4.5 cancer,” and within three minutes you’re reading about biopsies, Gleason scores, and survival rates. By the time you close the browser, you’ve already mentally planned your funeral.
Stop. Take a breath. Here’s the number your doctor probably didn’t tell you: 75% of men with a PSA grey zone result between 4 and 10 ng/mL do NOT have prostate cancer. Three out of four. The majority. That “raised PSA” is far more likely to be caused by a benign enlarged prostate, a silent infection, or even vigorous exercise before the blood test. A PSA result is not a cancer diagnosis — it’s a flag that says “let’s look more carefully.”
I see this panic in clinic every week. A man walks in with a printed lab result, pale-faced, convinced he has cancer. Most of the time, by the end of our consultation, I’m explaining why we’re not rushing to biopsy — and why that’s the correct decision. This article is the conversation I have with those men, written down so you can read it before your appointment and arrive informed rather than terrified.
📋 Key Takeaways
- A PSA between 4 and 10 ng/mL is called the “grey zone” — only about 25% of men in this range have prostate cancer on biopsy [1]
- PSA is prostate-specific, not cancer-specific — BPH, prostatitis, UTI, ejaculation, and even cycling can raise it
- A single PSA number matters far less than PSA velocity (how fast it’s rising over serial tests) and PSA density (PSA divided by prostate volume)
- Free-to-total PSA ratio helps distinguish BPH from cancer — a ratio above 25% makes cancer less likely; below 10% makes it more likely
- MRI before biopsy is now standard practice — it reduces unnecessary biopsies by 28% and detects clinically significant cancers more accurately than blind biopsy [2]
- Not every elevated PSA needs a biopsy, and not every prostate cancer needs treatment — low-grade cancers are often safely monitored with active surveillance
In This Guide:
What Is PSA — and Why Does It Cause So Much Confusion?
PSA (prostate-specific antigen) is a protein produced by the prostate gland. Its biological function is to liquefy semen after ejaculation. In healthy men, small amounts leak into the bloodstream. When the prostate is enlarged, inflamed, infected, or cancerous, more PSA enters the blood — and the level rises.
Here is the distinction that most lab reports fail to communicate: PSA is prostate-specific, not cancer-specific. A PSA of 6.0 tells you the prostate is producing more antigen than expected. It does not tell you why. The “why” could be benign prostatic hyperplasia (BPH — a non-cancerous enlargement that affects 50% of men by age 60), a subclinical prostatitis you didn’t even know you had, a urinary tract infection, or yes — prostate cancer. But cancer is the least common cause of a mildly elevated PSA.
The traditional “normal” cutoff of 4.0 ng/mL was established decades ago as a pragmatic threshold, not a biological boundary. There is no magic number where cancer suddenly appears. Some men harbor cancer with a PSA of 2.5; others have a PSA of 8.0 from a massive benign prostate (sometimes 80 grams or more — about 2.8 oz, roughly three times the normal walnut size) and no cancer at all. This is why the PSA grey zone — values between 4 and 10 ng/mL — creates so much anxiety. You’re in a range where cancer is possible but unlikely, and the next steps matter enormously.
The PSA Grey Zone: What Do the Numbers Actually Mean?
When urologists talk about the PSA grey zone, they’re referring to PSA values between 4.0 and 10.0 ng/mL. In this range, the probability of finding prostate cancer on biopsy is approximately 25% [1]. That means 75% of biopsies performed solely because of a grey-zone PSA find no cancer whatsoever. Three out of four men undergo an invasive procedure — with its associated pain, bleeding risk, and infection risk — for a result that reads “benign.”
This is not a criticism of PSA testing. It’s a criticism of reacting to a single number without context. Modern urology has moved far beyond “PSA above 4 = biopsy.” We now use several refinements that dramatically improve how we interpret grey-zone results.
Age-adjusted PSA reference ranges
The prostate grows with age, and a larger prostate naturally produces more PSA. A PSA of 4.5 in a 75-year-old with a 90-gram prostate (about 3.2 oz) is entirely unremarkable. The same PSA in a 45-year-old with a 25-gram prostate is far more concerning. Age-adjusted reference ranges account for this:
| Age Range | Upper Limit of Normal PSA |
|---|---|
| 40–49 years | 2.5 ng/mL |
| 50–59 years | 3.5 ng/mL |
| 60–69 years | 4.5 ng/mL |
| 70–79 years | 6.5 ng/mL |
A 52-year-old man with a PSA of 4.5 is above his age-adjusted threshold (3.5) and warrants further investigation. A 72-year-old with the same PSA of 4.5 is within normal limits for his age. Context changes everything.
→ Use the PSA Age-Adjusted Interpreter Tool to check your number against your age bandPSA velocity — the trend matters more than the snapshot
A single PSA measurement is a photograph. PSA velocity is a video. If your PSA was 2.8 two years ago, 3.5 last year, and 4.5 now — that’s a rise of 0.85 ng/mL per year, which is above the concerning threshold of 0.75 ng/mL/year [4]. That trend is more alarming than the absolute number.
Conversely, a man whose PSA has been stable at 4.8 for five years is far less concerning than a man whose PSA has jumped from 2.0 to 4.8 in 18 months. This is why I always ask patients for their previous PSA results, not just the latest one. If you’ve had PSA tests before, bring all the results to your urology appointment. They tell a story that a single number cannot.
→ Track your PSA over time with the PSA Velocity CalculatorFree-to-total PSA ratio — the underused refiner
PSA circulates in the blood in two forms: bound to proteins (complexed PSA) and free (unbound). Prostate cancer tends to produce more complexed PSA, meaning the proportion of free PSA drops. Measuring the free-to-total PSA ratio helps distinguish cancer from BPH in the grey zone [5]:
- Free PSA above 25%: Lower cancer risk — more consistent with BPH. Biopsy can often be deferred with monitoring
- Free PSA 10–25%: Intermediate risk — clinical judgment needed, consider MRI
- Free PSA below 10%: Higher cancer risk — biopsy should be strongly considered
Free-to-total ratio is most valuable precisely in the grey zone (PSA 4–10), where the raw total PSA alone is a poor discriminator. If your doctor has only checked total PSA, ask whether free PSA was included. If not, it can sometimes be added without a new blood draw if the sample is still available at the laboratory.
PSA density — adjusting for prostate size
A large prostate produces more PSA simply because there is more prostate tissue. PSA density corrects for this by dividing PSA by prostate volume (measured on ultrasound or MRI). A PSA density above 0.15 ng/mL/cc is more suspicious for cancer [6].
Consider two men, both with a PSA of 7.0. Man A has a prostate volume of 80 cc on ultrasound — his PSA density is 0.09. That PSA is almost certainly coming from a large benign prostate. Man B has a prostate volume of 30 cc — his PSA density is 0.23. That’s a small prostate producing a disproportionate amount of PSA, which raises the suspicion for cancer significantly. Same PSA, completely different clinical meaning.
→ Related: Enlarged Prostate (BPH) — When Medication Fails and Surgery Becomes the AnswerWhat Else Can Cause a Raised PSA? (It’s a Long List)
Before assuming the worst, you should know that many benign conditions raise PSA — sometimes significantly. If any of the following applied to you before your blood test, the result may be a false alarm:
Benign prostatic hyperplasia (BPH): The most common cause of mildly elevated PSA. A prostate that has grown from 25 grams to 80 grams (about 2.8 oz) will produce proportionally more PSA. This is physiology, not pathology.
Prostatitis (prostate infection or inflammation): Acute bacterial prostatitis can spike PSA to 20, 30, or even higher. Chronic prostatitis can cause persistent mild elevation. If you’ve had any urinary burning, perineal discomfort, or flu-like symptoms recently, this needs to be excluded before interpreting the PSA [7].
Urinary tract infection: Any infection in the urinary tract can transiently raise PSA. A simple UTI treated with antibiotics should be followed by a repeat PSA 6–8 weeks later to check whether the level normalizes.
Recent ejaculation: Ejaculation can raise PSA by 0.5–0.8 ng/mL for up to 48 hours. This won’t turn a normal PSA into a grey-zone result, but it can nudge a borderline PSA just above the threshold. Most guidelines recommend avoiding ejaculation for 48 hours before a PSA test [8].
Vigorous exercise and cycling: Prolonged cycling puts direct pressure on the perineum and prostate. A long bike ride the day before a blood test can cause a transient PSA rise. Similarly, vigorous exercise (not casual walking) can elevate it.
Urological procedures: Digital rectal examination (DRE), catheterization, cystoscopy, and prostate biopsy all raise PSA — sometimes for weeks. If you’ve had any of these recently, your PSA result should be interpreted with caution or repeated after an appropriate interval (typically 4–6 weeks).
Your PSA Is Confirmed Elevated — What Happens Next?
Let’s say you’ve repeated the test, excluded obvious confounders (infection, recent ejaculation, cycling), and the PSA is still in the grey zone. Here is the modern clinical pathway — and it does not begin with a biopsy needle.
Step 1: Clinical assessment and DRE
Your urologist will take a detailed history — urinary symptoms, family history of prostate cancer (first-degree relatives double your risk), medication use, and any recent events that could explain the rise. A digital rectal examination (DRE) assesses the prostate’s size, shape, symmetry, and surface. A hard nodule, asymmetry, or fixed irregular surface raises suspicion independently of PSA.
DRE has limitations — it only assesses the posterior part of the prostate, and anterior cancers are missed. But approximately 15–25% of prostate cancers are detected by DRE in men with a normal PSA [9], which is why most guidelines recommend DRE alongside PSA, not PSA alone.
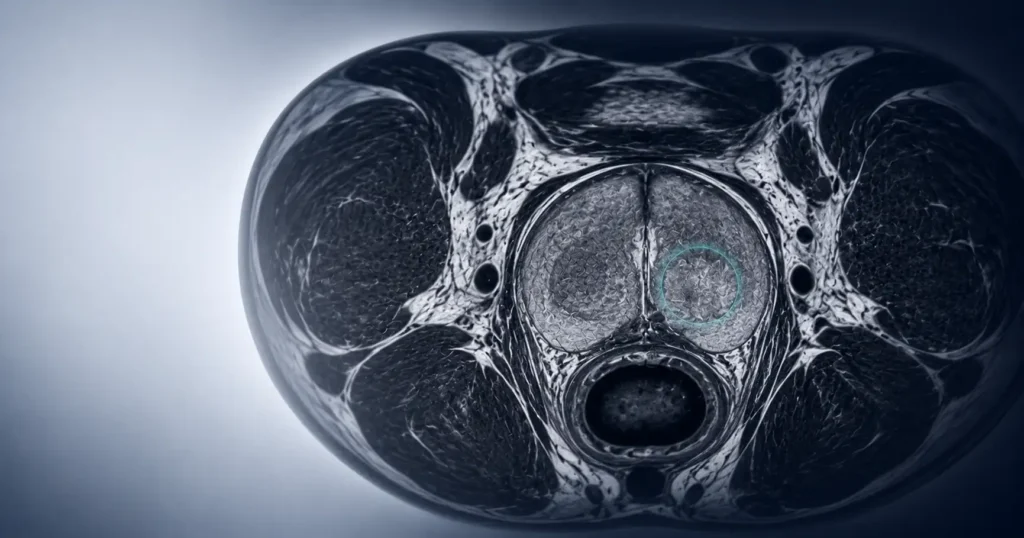
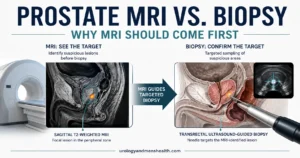
Step 2: Multiparametric MRI — the standard before biopsy
Until 2017, the pathway after a raised PSA was depressingly simple: straight to biopsy. A TRUS (transrectal ultrasound) guided biopsy — 10–12 needle cores taken semi-blindly through the rectal wall — was the standard. This approach had two major problems: it missed cancers that the needles didn’t sample (particularly in the anterior prostate), and it detected many low-grade cancers that would never cause harm but triggered treatment cascades with real side effects.
Multiparametric MRI (mpMRI) has fundamentally changed this. The landmark PROMIS trial (2017) and PRECISION trial (2018) demonstrated that performing an MRI before biopsy [2][10]:
- Reduces unnecessary biopsies by 28% — if the MRI shows no suspicious lesion, biopsy can often be safely deferred with PSA monitoring
- Detects clinically significant cancer 18% more accurately than blind TRUS biopsy
- Reduces detection of clinically insignificant cancers by 5% — fewer men diagnosed with cancers that were never going to harm them
The MRI uses a scoring system called PI-RADS (Prostate Imaging Reporting and Data System), scored 1–5:
- PI-RADS 1–2: Very low/low probability of clinically significant cancer. Biopsy generally NOT needed. Monitor with serial PSA
- PI-RADS 3: Equivocal — intermediate probability. Biopsy may be considered based on clinical context (PSA density, risk factors, patient preference)
- PI-RADS 4–5: High/very high probability of clinically significant cancer. MRI-targeted biopsy strongly recommended
Think of MRI as a reconnaissance mission before committing troops. Rather than sending needles in blind, you first map the territory. If the map shows no enemy (PI-RADS 1–2), you hold fire and watch. If it shows a suspicious target (PI-RADS 4–5), you aim precisely at that target instead of firing randomly.
Step 3: Biopsy — targeted, not blind
When biopsy IS indicated after MRI, modern practice favors MRI-targeted biopsy (fusion biopsy) — the MRI images are overlaid onto the ultrasound during biopsy, allowing the urologist to target specific suspicious areas rather than sampling blindly. This improves detection of clinically significant cancers while reducing the number of cores needed [10].
There is also an important shift toward transperineal biopsy (through the skin of the perineum between the scrotum and anus) rather than transrectal biopsy. The transperineal approach has a significantly lower infection rate — virtually eliminating the risk of post-biopsy sepsis that occurs in approximately 1–3% of TRUS biopsies [11]. The AUA and EAU Guidelines (2024) now recommend the transperineal route as the preferred approach where available [3].
→ Related: Prostate Cancer Screening — The Age-by-Age Guide Every Man NeedsDownload Your Free Clinical Action Plan
Enter your email below to download Dr. Khalid’s complete BPH & Prostate Screening Guide as a free, printable PDF.
If Cancer IS Found — Does That Mean I Need Treatment?
This is where the conversation becomes genuinely nuanced. Not all prostate cancers are created equal. The disease ranges from slow-growing tumors that will never affect your life to aggressive cancers that can be lethal. The distinction hinges on the Gleason score (now reported as Grade Group 1–5).
Understanding your Gleason score and Grade Group
The pathologist examines the biopsy tissue under a microscope and assigns two Gleason pattern numbers (each 1–5) that reflect how abnormal the cancer cells look. These are added together to give the Gleason score (e.g., 3+3 = 6, 3+4 = 7, 4+3 = 7). The Grade Group simplifies this into five categories [12]:
| Grade Group | Gleason Score | Risk Level |
|---|---|---|
| 1 | 3+3 = 6 | Low risk — often managed with active surveillance |
| 2 | 3+4 = 7 | Favorable intermediate — treatment or close surveillance |
| 3 | 4+3 = 7 | Unfavorable intermediate — treatment usually recommended |
| 4 | 4+4 = 8 | High risk — treatment recommended |
| 5 | 9–10 | Very high risk — aggressive treatment needed |
The difference between Gleason 3+4 and 4+3 is not trivial — even though both add up to 7. Gleason 4+3 (Grade Group 3) means the dominant pattern is more aggressive, and the prognosis and management differ from Gleason 3+4 (Grade Group 2). This is why the newer Grade Group system exists — it avoids the confusion of lumping two meaningfully different diseases under the same Gleason sum.
→ Use the Gleason Score Risk Interpreter to understand your biopsy reportActive surveillance — watching carefully, not doing nothing
For men with Grade Group 1 (Gleason 6) prostate cancer — which is the most commonly detected grade in the grey-zone PSA range — the evidence strongly supports active surveillance rather than immediate surgery or radiotherapy. This is not “watchful waiting” or “ignoring it.” It’s a structured monitoring program: regular PSA tests, repeat MRI, and sometimes repeat biopsies, with the intention to intervene if the cancer shows signs of progression [13].
The landmark ProtecT trial demonstrated that prostate cancer-specific mortality was extremely low (below 1%) at 10-year follow-up regardless of whether men received immediate treatment or were monitored [14]. Active surveillance spares approximately 50–60% of eligible men from unnecessary treatment over 10 years — treatment that would have impaired their erectile function, continence, or both, for a cancer that was never going to harm them.
The most common mistake I see is a man being told “you have cancer” and immediately assuming he needs surgery next month. Grade Group 1 cancer in a 65-year-old with a small-volume tumor on MRI is a condition that can be safely watched. The anxiety of living with a cancer diagnosis is real, but the side effects of unnecessary treatment — erectile dysfunction, urinary incontinence — are also real. This is a decision that deserves an unhurried, balanced conversation, not a panicked rush to the operating theater.
The Psychological Burden: Why “Grey Zone” Feels Like a Sentence
I want to acknowledge something that medical articles rarely address: the wait is brutal. Between your doctor’s phone call and your urology appointment — between the blood test and the MRI — between the MRI and the biopsy result — you are living in uncertainty. Every internet search feeds the fear. Every twinge in your pelvis feels like a symptom you missed.
This psychological burden is a genuine clinical problem, not a weakness. Studies show that men awaiting prostate biopsy experience anxiety levels comparable to those diagnosed with other cancers [15]. The grey zone, by its very name, denies you the comfort of a clear answer.
What I tell every man sitting in front of me with a grey-zone PSA: the odds are in your favor. Three out of four men in your position do not have cancer. And even among the one in four who does, the majority have low-grade disease that can be managed without radical treatment. The pathway is designed to give you clarity — not to rush you into unnecessary procedures. Every step (repeat PSA, free-to-total ratio, MRI, targeted biopsy) narrows the uncertainty until you have an answer you can act on.
💡 In My Practice
The most common scenario I encounter is a man referred from primary care with a PSA between 4 and 7, no urinary symptoms, and enormous anxiety. He’s Googled his result, read the worst-case scenarios, and arrives convinced he has cancer. My first task isn’t to order tests — it’s to recalibrate his expectations. I walk him through the 75% statistic, explain that his doctor did the right thing by referring him, and outline the stepwise pathway: repeat PSA, free-to-total ratio, DRE, and MRI before we even discuss biopsy. Most of the time, the relief is visible within the first five minutes of the consultation.
One pattern that concerns me more than a single elevated PSA is the man who has never had a PSA test and presents for the first time at 65 with a PSA of 9 — no previous baseline, no trend data, no way to assess velocity. A baseline PSA at 45–50 would have given us a trajectory to interpret this number against. Without that baseline, we’re flying blind. This is why I push my own patients hard on getting at least one baseline PSA in their mid-40s, especially if there’s any family history. It’s the cheapest, most informative single number in men’s health.
The cases that stay with me are the men where the system worked exactly as designed. A patient in his late 50s with a PSA of 6.2, a confidently abnormal DRE, PI-RADS 4 lesion on MRI, and Grade Group 2 cancer on targeted biopsy. He had a successful nerve-sparing prostatectomy, full continence within three months, and an undetectable PSA at his most recent follow-up. He’d never have caught that without the workup. The pathway isn’t there to scare you — it’s there to find the cancers that need finding, and reassure the majority who don’t have one.
How to Prepare for Your PSA Test (and Avoid False Elevations)
If you’re due for a PSA test — whether it’s your first or a repeat — these steps reduce the risk of a falsely elevated result that generates unnecessary worry:
Avoid ejaculation for 48 hours before the blood draw. Ejaculation transiently elevates PSA, and while the effect is usually small, it can push a borderline value above the threshold.
Avoid vigorous exercise and cycling for 48 hours. Casual walking is fine. A 50-mile (about 80 km) bike ride the day before is not.
Do not have the test during an active urinary infection. Treat the infection first, then recheck PSA 6–8 weeks later.
Tell your doctor about recent procedures. If you’ve had a DRE, catheterization, cystoscopy, or prostate biopsy in the past 6 weeks, the PSA may still be elevated from the procedure. Wait and retest.
Morning blood samples are preferred but not mandatory. PSA has a slight diurnal variation, and morning levels tend to be slightly lower, but the difference is small enough that it won’t change clinical decisions.
Family History and High-Risk Groups: When to Start Testing Earlier
Not every man carries the same risk. If you have a first-degree relative (father or brother) with prostate cancer, your risk is approximately doubled. If that relative was diagnosed before age 65, or if you have two or more affected relatives, your risk rises further [16]. Men of African or African-American descent also carry a higher baseline risk and are more likely to develop aggressive disease.
For these high-risk groups, both the AUA and EAU recommend baseline PSA testing from age 40–45 — not 50 [3]. A baseline PSA at 45 is one of the cheapest and most informative risk-stratification tools in medicine. If your baseline PSA is below 1.0 ng/mL at 45, your lifetime risk of clinically significant prostate cancer is very low, and screening intervals can be extended. If it’s above 1.0 at that age, closer monitoring is warranted.
→ Estimate your personal prostate cancer risk with the Prostate Cancer Risk CalculatorWhat a PSA Grey Zone Result Does NOT Mean
Let me be explicit about what your grey-zone result is not:
It is not a cancer diagnosis. It is a screening marker that prompts further investigation. The majority of men with a grey-zone PSA do not have cancer.
It does not mean you need an immediate biopsy. Modern practice involves repeat testing, refinement with free PSA and PSA density, and MRI before biopsy is considered. The days of “PSA above 4, biopsy next Tuesday” are over.
It does not mean you will lose your prostate, your continence, or your erections. Even if cancer is found, the grade and stage determine management — and the majority of grey-zone cancers are low-grade, manageable, and compatible with a normal life.
It does not mean you did something wrong. Prostate cancer has no known preventable cause. It is not caused by diet, lifestyle, or sexual activity. The guilt that some men feel — “Did I cause this?” — has no basis in the evidence.
⚠️ When to See a Doctor — Urgently
- Visible blood in your urine (hematuria) — may indicate prostate, bladder, or kidney pathology and should never be ignored, even if painless
- Complete inability to urinate (acute urinary retention) — this is an emergency. Go to the emergency room (ER) immediately. A catheter will be placed to drain the bladder
- New, unexplained bone pain (especially in the lower back, hips, or pelvis) — in the context of a raised PSA, this could indicate metastatic disease and requires urgent investigation
- Rapidly rising PSA — if your PSA has doubled or more in under 12 months, this warrants urgent urological assessment rather than routine follow-up
- Fever with urinary symptoms after a prostate biopsy — post-biopsy sepsis is a medical emergency. Temperature above 100.4°F (38°C) with chills, rigors, or feeling unwell after biopsy requires immediate hospital attendance
Trusted Patient Resources
If you’d like to read further from independent, internationally recognized organizations, the following are reliable starting points:
- Prostate Cancer Screening — The Age-by-Age Guide Every Man Needs
- External resource: Prostate Cancer Foundation — patient guides on PSA, diagnosis, and treatment
- External resource: ZERO Prostate Cancer — peer support and family-history risk tools
- External resource: Prostate Cancer UK — plain-English guides and a confidential nurse helpline
Frequently Asked Questions
Does a PSA of 4.5 mean I have prostate cancer?
No. A PSA of 4.5 falls within the PSA grey zone (4–10 ng/mL), where only about 25% of men have cancer on biopsy — meaning 75% do not. PSA is elevated by many benign conditions, including BPH (enlarged prostate), prostatitis, UTI, and even recent ejaculation. A raised PSA is not a diagnosis — it’s a trigger for further investigation, starting with clinical assessment, free-to-total PSA ratio, and MRI. The pathway is designed to separate the men who genuinely need biopsy from those who can be safely monitored. Use the PSA Interpreter tool to put your number in context.
Should I get a biopsy immediately if my PSA is elevated?
Not necessarily — and in modern practice, usually not as the first step. Current AUA and EAU guidelines recommend MRI before biopsy for grey-zone PSA results. The PROMIS and PRECISION trials showed that MRI reduces unnecessary biopsies by 28% while detecting clinically significant cancers more accurately. If the MRI is normal (PI-RADS 1–2), biopsy can often be safely deferred with PSA monitoring. Biopsy is reserved for men with suspicious MRI findings (PI-RADS 4–5), concerning PSA trends, or abnormal DRE. Read more in our guide to enlarged prostate and treatment options.
Can cutting out red meat or taking supplements lower my PSA?
There is no reliable evidence that dietary changes or supplements meaningfully lower PSA in a way that affects cancer risk. Some supplements (particularly saw palmetto) may slightly reduce PSA, which is actually dangerous because it can mask a genuinely rising PSA and delay cancer detection. If you’re taking any prostate supplement, tell your urologist — they need to know when interpreting your PSA. The goal is not to lower your PSA artificially; the goal is to know what’s causing it to be elevated.
What is the difference between PSA and free PSA?
Total PSA measures all PSA in the blood. Free PSA measures the unbound fraction. Cancer tends to produce more protein-bound (complexed) PSA, so a low free-to-total ratio (below 10%) raises cancer suspicion, while a high ratio (above 25%) suggests BPH. Free-to-total ratio is most useful precisely in the PSA grey zone (4–10 ng/mL), where total PSA alone cannot reliably distinguish cancer from benign enlargement. Ask your doctor whether free PSA was included in your blood panel — if not, it can sometimes be run on the same stored sample. Track changes over time with the PSA Velocity tool.
If prostate cancer is found, will I definitely need surgery?
No. Low-grade prostate cancer (Grade Group 1, Gleason 6) is increasingly managed with active surveillance — structured monitoring with regular PSA, MRI, and sometimes repeat biopsies — rather than immediate surgery or radiotherapy. The ProtecT trial showed that cancer-specific mortality was below 1% at 10 years regardless of whether men were treated or monitored. Approximately 50–60% of men on active surveillance avoid treatment entirely. Surgery, radiotherapy, or other treatments are reserved for intermediate- and high-grade cancers, or for low-grade cancers that show signs of progression on monitoring. The Gleason Score Interpreter helps you understand what your specific report means.
📚 References
- Catalona WJ, Smith DS, Ratliff TL, et al. Measurement of prostate-specific antigen in serum as a screening test for prostate cancer. N Engl J Med. 1991;324(17):1156-1161. PubMed
- Kasivisvanathan V, Rannikko AS, Borghi M, et al. MRI-targeted or standard biopsy for prostate-cancer diagnosis (PRECISION trial). N Engl J Med. 2018;378(19):1767-1777. PubMed
- European Association of Urology. Guidelines on Prostate Cancer. 2024 Edition. EAU Guidelines. See also: American Urological Association. Early Detection of Prostate Cancer: AUA Guideline. 2023. AUA Guidelines
- Carter HB, Ferrucci L, Kettermann A, et al. Detection of life-threatening prostate cancer with prostate-specific antigen velocity during a window of curability. J Natl Cancer Inst. 2006;98(21):1521-1527. PubMed
- Catalona WJ, Partin AW, Slawin KM, et al. Use of the percentage of free prostate-specific antigen to enhance differentiation of prostate cancer from benign prostatic disease. JAMA. 1998;279(19):1542-1547. PubMed
- Benson MC, Whang IS, Pantuck A, et al. Prostate specific antigen density: a means of distinguishing benign prostatic hypertrophy and prostate cancer. J Urol. 1992;147(3 Pt 2):815-816. PubMed
- Sharp VJ, Takacs EB, Powell CR. Prostatitis: diagnosis and treatment. Am Fam Physician. 2010;82(4):397-406. PubMed
- Herschman JD, Smith DS, Catalona WJ. Effect of ejaculation on serum total and free prostate-specific antigen concentrations. Urology. 1997;49(2):207-210. PubMed
- Richie JP, Catalona WJ, Ahmann FR, et al. Effect of patient age on early detection of prostate cancer with serum prostate-specific antigen and digital rectal examination. Urology. 1993;42(4):365-374. PubMed
- Ahmed HU, El-Shater Bosaily A, Brown LC, et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confirmatory study. Lancet. 2017;389(10071):815-822. PubMed
- Xiang J, Yan H, Li J, et al. Transperineal versus transrectal prostate biopsy in the diagnosis of prostate cancer: a systematic review and meta-analysis. World J Surg Oncol. 2019;17(1):31. PubMed
- Epstein JI, Egevad L, Amin MB, et al. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am J Surg Pathol. 2016;40(2):244-252. PubMed
- Klotz L, Vesprini D, Sethukavalan P, et al. Long-term follow-up of a large active surveillance cohort of patients with prostate cancer. J Clin Oncol. 2015;33(3):272-277. PubMed
- Hamdy FC, Donovan JL, Lane JA, et al. 10-year outcomes after monitoring, surgery, or radiotherapy for localised prostate cancer (ProtecT trial). N Engl J Med. 2016;375(15):1415-1424. PubMed
- Wade J, Rosario DJ, Macefield RC, et al. Psychological impact of prostate biopsy: physical symptoms, anxiety, and depression. J Clin Oncol. 2013;31(33):4235-4241. PubMed
- Bruner DW, Moore D, Parlanti A, et al. Relative risk of prostate cancer for men with affected relatives: systematic review and meta-analysis. Int J Cancer. 2003;107(5):797-803. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.