Recurrent UTI in Men: The Workup Your GP May Skip
When a man gets his third UTI of the year, he usually assumes he just needs a stronger antibiotic to finally clear it. In my experience, the infection is rarely the actual problem—it is just the alarm bell for a hidden stone, enlarged prostate, or blockage that a prescription won't fix. This guide walks you through the medical workup you actually need to find out why the bacteria keeps returning.

A second UTI in twelve months is not bad luck. In women, recurrent urinary tract infection is common enough that guidelines treat it as a defined clinical category. In men, it is different. A recurrent UTI in men almost always means something inside the urinary tract is wrong — a stone, a prostate problem, incomplete bladder emptying, or a structural narrowing — and the second infection is the alarm. I see men in clinic every week who have been on their third or fourth course of antibiotics from their primary care doctor without anyone asking the question that matters: why does the infection keep coming back? This article walks through the diagnostic workup I run on every man with two or more confirmed UTIs in six months, and what to push for if your GP has not started it.
Key Takeaways
- Two or more confirmed UTIs in 6 months — or 3 in 12 months — meets the definition of recurrent UTI and warrants urology referral, per AUA 2022 guidance.
- The single most common cause in men over 50 is incomplete bladder emptying from an enlarged prostate, which leaves residual urine for bacteria to colonize.
- Every workup starts with a clean-catch urine culture before antibiotics — empirical treatment without a culture is the most common reason men cycle through infections for months.
- Imaging (renal and bladder ultrasound) plus flexible cystoscopy will identify the cause in the majority of cases; a normal workup is reassurance, not failure.
In This Guide:
What Counts as a Recurrent UTI in Men?
The American Urological Association defines recurrent UTI as two culture-proven infections in six months, or three in twelve months.[1] The word “culture-proven” matters. A urine dipstick showing leukocytes and nitrites is suggestive but not diagnostic. A culture identifies the specific bacterial organism, its concentration in colony-forming units per millilitre, and which antibiotics it responds to.
This distinction is the first place men get poorly served. A primary care doctor treating burning and frequency with a 5-day antibiotic course based on symptoms alone has no idea what organism was treated, whether the antibiotic was right, or whether the infection truly cleared. If symptoms come back four weeks later, there is no way to tell whether this is a relapse (same organism, treatment failed) or a reinfection (new organism, something is letting bacteria back in). The two scenarios point to different causes and need different workups.
Any UTI in a man is also, by default, classified as a complicated UTI under Infectious Diseases Society of America criteria.[2] The male urethra is anatomically longer than the female urethra and bacteria do not ascend it casually. When they do, it usually means an underlying mechanical or functional problem has helped them.
Why Men Get Recurrent UTIs: The Five Causes Worth Looking For
In my practice, recurrent UTI in a man almost always traces back to one of five problems. The workup is built to test for each in turn.
1. Incomplete bladder emptying (the most common cause over 50)
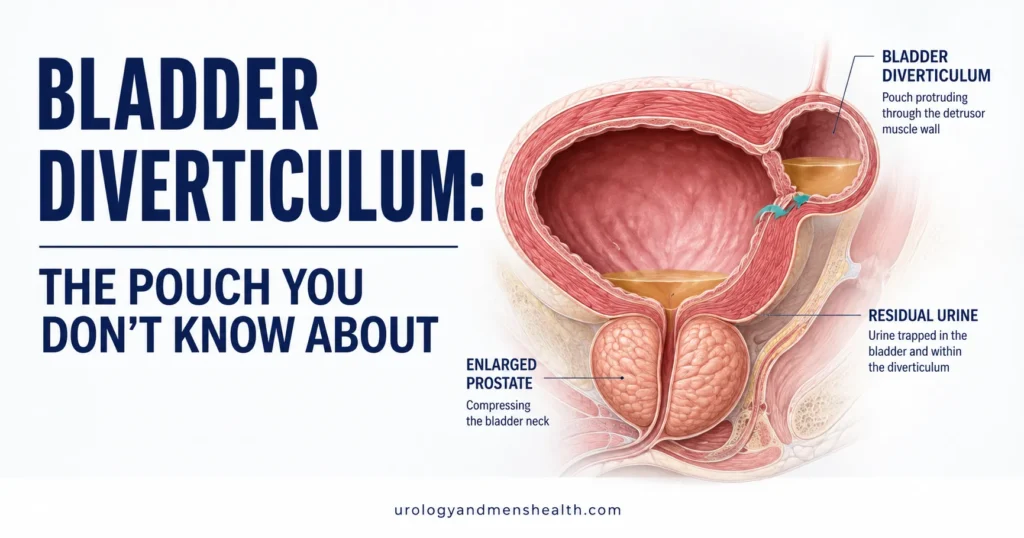
When the bladder does not empty fully, the leftover urine — called post-void residual — sits warm and still in the bladder for hours. Bacteria that would normally be flushed out at the next void get the chance to multiply. A residual volume above 100 mL is clinically meaningful; above 200 mL it is a near-guarantee of recurrent infections.[3] The most common reason for retention in men over 50 is benign prostatic hyperplasia (BPH), where an enlarged prostate compresses the urethra and blocks complete drainage.
2. Kidney or bladder stones
A stone in the bladder or kidney provides a biofilm surface that antibiotics cannot fully sterilize. Bacteria embedded in the biofilm survive the antibiotic course and reseed the urine when treatment stops. Struvite stones in particular are formed by urease-producing bacteria and create a self-reinforcing cycle — the stone causes the infection, the infection grows the stone.[4] Anyone with recurrent UTI and a history of stones needs upper-tract imaging.
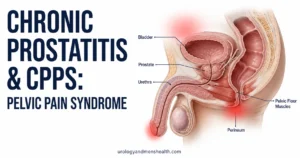
3. Chronic bacterial prostatitis
The prostate is a difficult organ for antibiotics to penetrate. When bacteria establish a chronic infection inside prostatic tissue, the gland becomes a reservoir that periodically reseeds the urine. The classic story is a man in his 40s or 50s with recurrent E. coli on culture, perineal discomfort between flares, and brief symptomatic improvement on antibiotics followed by relapse two to four weeks after stopping. Chronic prostatitis needs a longer antibiotic course (4 to 6 weeks) with a drug that penetrates prostate tissue.
→ Try the UTI Risk Assessment Tool for Men to estimate your underlying risk profile4. Urethral stricture
A narrowed segment of the urethra — from old infection, catheterization, instrumentation, or trauma — slows urinary flow and prevents the high-pressure stream that normally flushes bacteria out. Stricture is suggested by a slow stream, straining to void, post-micturition dribble, and a falling flow rate on uroflowmetry. It is confirmed with flexible cystoscopy.
5. Diabetes and immunocompromise
Poorly controlled diabetes raises urinary glucose, which feeds bacteria, and impairs the neutrophil response that normally clears low-grade infection. A man with new recurrent UTI and an HbA1c above 8% will not stop having infections until glycemic control improves. Long-term steroid use, chemotherapy, and untreated HIV have a similar effect.
In My Practice
The patient I think of often is a man in his late 50s referred for “another UTI.” He had been on four antibiotic courses in seven months. His primary care doctor was treating him on dipstick alone. When I ordered a clean-catch culture before antibiotics, the organism was Klebsiella with significant antibiotic resistance — not the E. coli the previous courses had been written for. His post-void residual was 280 mL. He had moderate BPH that nobody had ever measured because his prostate exam felt normal.
One urology workup — culture, ultrasound, flow study — found the cause two referrals and four antibiotic courses too late. The lesson is the one I keep repeating: in men, a second UTI is the signal to investigate, not to re-prescribe.
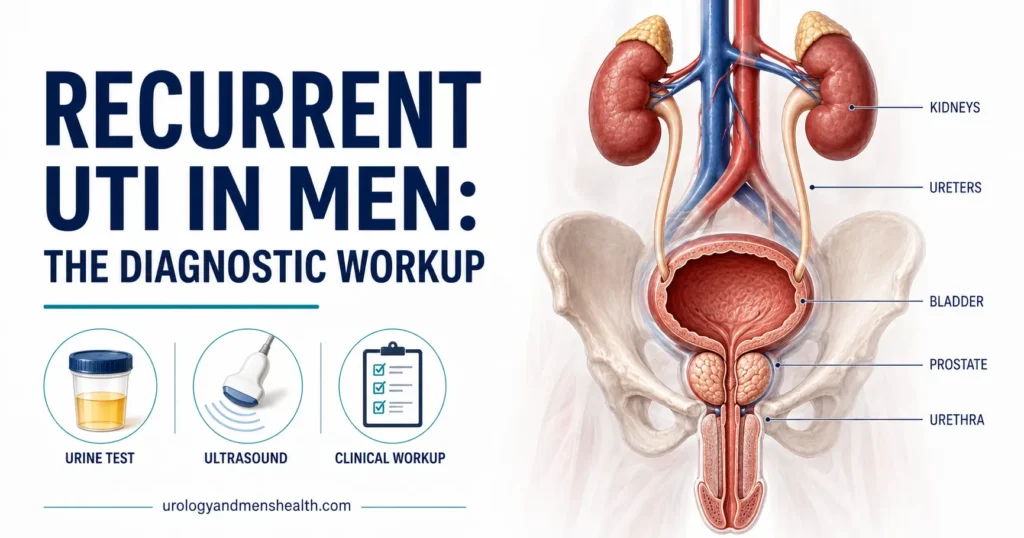
The UTI Workup for Men: What a Urologist Actually Does
Here is the workup I run on every man referred with two or more confirmed UTIs in six months. Each step rules in or out a specific cause. If your GP has not started this sequence, it is reasonable to ask for a urology referral.
Step 1: Clean-catch midstream urine culture with sensitivities
This is the foundation. The sample must be taken before any antibiotic is started, midstream (after the first few millilitres have been discarded), into a sterile container. The lab identifies the organism, the colony count (a true infection is typically above 10⁵ CFU/mL in a midstream sample), and the antibiotic sensitivity panel.[2] Without this, antibiotic choice is guesswork.
Step 2: Post-void residual ultrasound
A bladder scan takes thirty seconds in clinic. The patient voids normally, then the bladder is scanned with a portable ultrasound to measure how much urine is left behind. Anything above 100 mL warrants attention. Above 200 mL is a clear contributor to recurrent infection and needs targeted treatment — usually for BPH or a neurogenic bladder.
Step 3: Upper urinary tract imaging
Renal and bladder ultrasound is the standard first-line image. It identifies kidney stones, hydronephrosis (a backed-up kidney), and bladder stones. If ultrasound is inconclusive, or if there is microscopic blood in the urine, a non-contrast CT KUB is the next step. CT is more sensitive for small stones and for upper-tract abnormalities the ultrasound may miss.
Step 4: Flexible cystoscopy
A flexible cystoscope is a thin fibre-optic camera passed through the urethra into the bladder under local anaesthetic gel. The whole procedure takes around five minutes. It directly visualizes urethral strictures, bladder stones, bladder diverticula (pouches that trap urine), and any suspicious bladder lining. For a man with recurrent UTI and any element of voiding difficulty, this is the test that often finds what imaging missed.
Step 5: Targeted additional testing
Depending on what the first four steps show, the workup may include uroflowmetry (objective measurement of urinary flow rate), PSA testing if the prostate is enlarged, a digital rectal examination, an HbA1c if diabetes is suspected, and — for men with perineal pain or prostatitis features — a four-glass test or the simpler pre- and post-massage urine specimen.
Stuck in the antibiotic cycle? Get Dr. Khalid’s full eradication plan.
Enter your email below to receive Dr. Khalid’s complete Recurrent UTI Eradication Protocol as a free, printable PDF.
Relapse vs Reinfection: A Distinction That Changes Treatment
Once two cultures are available, the next clinical question is whether the infections are relapses or reinfections. The distinction comes from comparing the organism and sensitivities between episodes.
- Relapse: same organism, same sensitivity profile, within 2 weeks of finishing antibiotics. This usually points to a sanctuary site the antibiotic could not reach — chronic prostatitis, a stone, or an unresolved foreign body.
- Reinfection: a different organism (or the same organism with a different sensitivity pattern), more than 2 weeks after finishing antibiotics. This usually points to a mechanical reason bacteria keep getting in — incomplete emptying, a stricture, or behavioral factors.
Relapse needs a longer, prostate-penetrating antibiotic course and a search for the sanctuary site. Reinfection needs treatment of the mechanical cause. Both need urology input — neither is something to keep cycling through 5-day amoxicillin courses for.
When to Push for Urgent Referral
Not every recurrent UTI is an emergency, but certain features change the timeline. The presence of any of these in combination with a UTI warrants same-week urology assessment, and some warrant an emergency room visit.
Red Flags: See a Doctor Without Waiting
Any of these in combination with a UTI should not wait for the next routine appointment:
- Visible blood in the urine — frank hematuria with infection needs imaging to rule out bladder pathology.
- Flank or back pain plus fever above 38°C (100.4°F) — suggests pyelonephritis (kidney infection); this is an ER presentation.
- Inability to pass urine at all — acute retention is an emergency; do not wait.
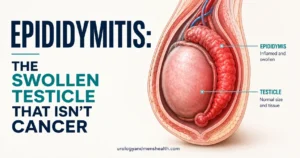
- Scrotal pain or swelling — possible epididymo-orchitis; needs same-day assessment.
- Confusion, low blood pressure, or rigors — possible urosepsis; call emergency services.
- UTI in a man with a single functioning kidney, recent stent, or recent urological surgery — escalate immediately.
For non-emergency recurrent UTI, the AUA standard is that a man with two confirmed UTIs in six months should be referred for urological workup.[1] If your GP has prescribed antibiotics twice without sending a culture, or without arranging imaging, asking for a referral is reasonable and clinically appropriate.
What the Workup Looks Like in Practice
For most men, the full workup fits into two clinic visits. At the first visit, the urologist takes a focused history (voiding pattern, prior infections, prior instrumentation, sexual history, comorbidities), does a digital rectal examination, performs a bladder scan, and arranges a clean-catch culture and renal and bladder ultrasound. At the second visit, results are reviewed and flexible cystoscopy is offered if indicated. A diagnosis is reached in the majority of men by the end of the second visit.
If everything is normal — culture confirms infection, imaging is clean, residual is under 50 mL, cystoscopy unremarkable — that is a meaningful result. It means the recurrent infections are likely behavioral or related to fluid intake and hygiene, and prophylactic strategies (low-dose nightly antibiotic, post-coital antibiotic, methenamine, or D-mannose) can be considered with safer expectations. A normal workup is not failure; it is the green light to focus on prevention without missing something serious.
FAQ
Why do I keep getting UTIs as a man when I never had them before?
A new pattern of recurrent UTI in men over 50 most often signals an enlarged prostate causing incomplete bladder emptying. Under 50, the more common causes are kidney or bladder stones, chronic prostatitis, or a urethral stricture from old instrumentation. The starting test is a post-void residual measurement plus a clean-catch culture before any further antibiotics. New-onset recurrent UTI is the urinary tract telling you something has changed and needs investigation.
How many UTIs counts as recurrent in men?
Per AUA guidance, two culture-confirmed infections in six months — or three in twelve months — meets the definition of recurrent UTI. In men, even one well-documented UTI is considered complicated and worth investigating, because the male urinary tract is anatomically more resistant to infection than the female tract. If you have had two infections within six months, this is the point to ask your primary care doctor for a urology referral rather than for another antibiotic course.
Can recurrent UTIs in men be a sign of cancer?
Rarely, but it is one of the things the workup is designed to rule out. Bladder cancer can present with recurrent UTI-like symptoms and intermittent blood in the urine. This is exactly why imaging and flexible cystoscopy are part of the standard workup — they identify bladder pathology that culture and dipstick cannot. The majority of recurrent UTIs in men are not cancer, but the workup is what tells you that confidently.
What antibiotic is best for recurrent UTI in men?
There is no single best antibiotic — the right choice depends on the culture sensitivity panel and on whether the prostate is involved. For uncomplicated cystitis with a sensitive organism, nitrofurantoin or trimethoprim are common first-line choices. For suspected chronic bacterial prostatitis, a fluoroquinolone (ciprofloxacin or levofloxacin) for 4 to 6 weeks is standard because it penetrates prostate tissue. Empirical prescribing without a culture is the most common reason men cycle through infections — push for the culture first.
Does cranberry juice or D-mannose help recurrent UTI in men?
Evidence for cranberry products is mixed and mostly studied in women. D-mannose has slightly better evidence for preventing E. coli-driven reinfection. Neither will fix an enlarged prostate, a stone, or a stricture — so neither replaces the workup. They can be reasonable additions for men whose workup is clean and whose recurrences are likely behavioral. Discuss them with your urologist rather than starting them as a first step.
Is sex causing my recurrent UTIs?
Sexual activity is a recognized trigger for UTI in men, particularly with new partners or with anal intercourse. However, in men a sexual trigger usually only becomes a recurrent problem when an underlying mechanical factor is also present — incomplete emptying, a stricture, or prostatitis. The workup will identify the mechanical contributor; behavioral strategies (voiding after sex, adequate hydration) help only after the underlying issue is addressed or excluded.
References
- Anger J, Lee U, Ackerman AL, et al. Recurrent Uncomplicated Urinary Tract Infections in Women: AUA/CUA/SUFU Guideline. Journal of Urology. 2022;208(1):11-20. AUA Guidelines
- Nicolle LE, Gupta K, Bradley SF, et al. Clinical Practice Guideline for the Management of Asymptomatic Bacteriuria: 2019 Update by the Infectious Diseases Society of America. Clinical Infectious Diseases. 2019;68(10):e83-e110. IDSA
- Bonkat G, Bartoletti R, Bruyère F, et al. EAU Guidelines on Urological Infections. European Association of Urology. 2024. EAU Guidelines
- Flannigan R, Choy WH, Chew B, Lange D. Renal struvite stones — pathogenesis, microbiology, and management strategies. Nature Reviews Urology. 2014;11(6):333-341. PubMed
- Urinary Tract Infections in Adults. National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). 2024. NIDDK
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.