Prostatitis symptoms in young men are the single most common reason men under 50 land in a urology clinic — and the single most common reason they walk in convinced they have prostate cancer. He’s 32, otherwise healthy, and worried. His symptoms — burning when urinating, a dull ache between his scrotum and rectum, frequency, urgency, pain after ejaculation — have been going on for weeks. His primary care doctor checked a PSA. It came back elevated. Now he’s terrified.
The answer, almost invariably, is no — this is not cancer. What he has is prostatitis — inflammation of the prostate gland — and it is the most common urological diagnosis in men under 50 [1]. It accounts for roughly 8% of all urology outpatient visits and 1% of all primary care visits by men [2]. Yet despite how common it is, prostatitis remains one of the most misunderstood, misdiagnosed, and poorly managed conditions in urology.
The problem is that prostatitis mimics other conditions convincingly — urinary tract infections, sexually transmitted infections, bladder problems, and yes, even prostate cancer. It also elevates PSA, which triggers a cascade of unnecessary anxiety and sometimes unnecessary biopsies. Getting the diagnosis right is the first step toward effective treatment, and it starts with understanding that “prostatitis” is not one disease — it’s at least four distinct conditions bundled under a single name.
Key Takeaways
- Prostatitis is the #1 urological diagnosis in men under 50 — it is not a disease of older men, and it is overwhelmingly not cancer.
- There are 4 distinct categories (NIH classification): acute bacterial, chronic bacterial, chronic pelvic pain syndrome (CPPS), and asymptomatic — each requires a different treatment approach.
- 90-95% of prostatitis cases are CPPS (Category III), meaning no bacteria are found and antibiotics alone are usually insufficient.
- Prostatitis elevates PSA, which frequently triggers unnecessary cancer anxiety. PSA should not be checked during active prostatic inflammation.
- Acute bacterial prostatitis is a medical emergency — high fever, inability to urinate, and sepsis risk require urgent IV antibiotics and sometimes catheterization.
- CPPS treatment is multimodal: alpha-blockers, anti-inflammatories, pelvic floor physiotherapy, and stress management — not repeated antibiotic courses.
- The condition is not sexually transmitted, does not cause prostate cancer, and is not caused by sexual frequency in either direction.
In This Guide:
What Prostatitis Symptoms in Young Men Actually Look Like
Before classifying which type of prostatitis a man has, it’s worth describing what the condition actually feels like — because most patients I see have been told for weeks that they have a “UTI” or “muscle strain,” and the symptom pattern they describe is in fact textbook prostatitis. The dominant features cluster in three groups.
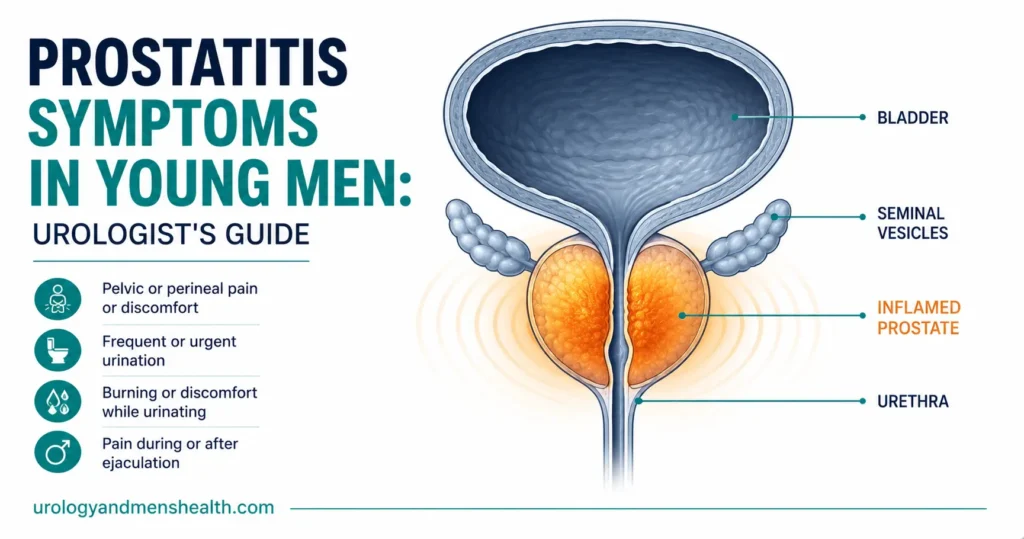
Pain or discomfort is the central feature. Most men describe it in one of these locations: the perineum (the area between scrotum and anus, often the most reliable site), suprapubic region (just above the pubic bone), tip or shaft of the penis, scrotum or testicles, lower back, or inner thighs. The pain is often dull and aching rather than sharp, frequently worse after sitting for long periods, and not uncommonly worsened by ejaculation — a pattern that distresses men who don’t yet understand its mechanism.
Urinary symptoms overlap heavily with what looks like a UTI: burning during urination (dysuria), increased frequency, urgency, sometimes a weak or interrupted stream, and the sensation of incomplete emptying. The trap here is that a urine dipstick may be negative, and a urine culture may be sterile — yet the symptoms are real and clinically driven by the prostate.
Sexual symptoms are the third cluster and the one men least often volunteer: pain during or after ejaculation, reduced libido, erectile difficulties, and occasionally hematospermia (blood in semen). When a young man presents with the combination of perineal ache, dysuria, and post-ejaculatory pain, the diagnosis is almost always prostatitis until proven otherwise — even if the urine culture is negative.
The NIH Classification: Four Conditions, One Name
The confusion surrounding prostatitis starts with the name itself. The word literally means inflammation of the prostate, but that umbrella term covers conditions that range from life-threatening sepsis to chronic pain with no identifiable infection. The NIH classification system (1999) divides prostatitis into four categories, and understanding which one you have determines everything about your treatment [3].
Category I: Acute Bacterial Prostatitis
This is the dramatic one — and the only truly dangerous category. A patient with acute bacterial prostatitis presents acutely unwell: high fever (often 39-40°C / 102-104°F), severe perineal pain, inability to urinate, and sometimes frank sepsis with rigors and hemodynamic instability. The prostate is exquisitely tender on digital rectal examination — so tender that a vigorous exam is inadvisable because it risks bacteremia.
The causative organisms are typically Gram-negative bacteria — E. coli in 60-80% of cases, followed by Klebsiella, Proteus, and Pseudomonas [4]. Urine cultures are usually positive. Blood cultures should be taken if sepsis is suspected.
Treatment is urgent IV antibiotics — typically a fluoroquinolone (ciprofloxacin or levofloxacin) or a third-generation cephalosporin. The transition to oral antibiotics happens once the patient is afebrile for 24-48 hours and inflammatory markers (CRP, WBC) are clearly trending down. Total antibiotic duration is 4-6 weeks to ensure prostatic penetration and prevent transition to chronic infection [5]. If the patient cannot urinate, suprapubic catheterization is preferred over urethral catheterization — passing a urethral catheter through an acutely inflamed prostate risks worsening prostatic trauma and provoking bacteremia. This is a clinical distinction that often gets missed in the ER, and it matters.
Acute bacterial prostatitis accounts for less than 5% of all prostatitis cases — but it is the one category where delay in treatment can be life-threatening.
Category II: Chronic Bacterial Prostatitis
This is the frustrating recurrent version. The same bacteria that cause acute prostatitis establish a persistent focus within the prostate gland, protected by the prostatic tissue barrier that limits antibiotic penetration. Patients experience recurrent UTIs (often with the same organism on culture), with intervals of relative wellness between episodes.
Symptoms include dysuria, frequency, urgency, and perineal discomfort — similar to a UTI but with a pelvic pain component. The key diagnostic feature is positive bacterial cultures from expressed prostatic secretions or post-prostatic massage urine (the Meares-Stamey 4-glass test or the simplified 2-glass post-prostatic massage test) [6]. If you’ve had two or more UTIs with the same organism, this is the workup to ask for — not just another empirical antibiotic course. You can quickly check your overall risk pattern with our UTI risk assessment for men before pushing for the full prostatic localization workup.
Treatment requires prolonged antibiotics — 4 to 6 weeks minimum, using agents with good prostatic penetration: fluoroquinolones (ciprofloxacin, levofloxacin) or trimethoprim-sulfamethoxazole. Even with appropriate treatment, cure rates are only 60-80%, and some patients require suppressive low-dose antibiotics for months [5].
Chronic bacterial prostatitis accounts for roughly 5-10% of prostatitis cases.
Category III: Chronic Prostatitis / Chronic Pelvic Pain Syndrome (CP/CPPS)
This is the big one — and the most difficult. CPPS accounts for 90-95% of all prostatitis cases [1]. The hallmark is chronic pelvic pain lasting at least 3 of the previous 6 months, with or without urinary symptoms, in the absence of demonstrable bacterial infection.
The pain is typically felt in one or more of the following locations: perineum (between scrotum and anus), suprapubic area, lower back, penis tip, scrotum, or inner thighs. Pain is often worsened by sitting, ejaculation, or stress. Urinary symptoms (frequency, urgency, weak stream) may coexist.
Category III is further subdivided into:
- IIIA (inflammatory) — white blood cells found in prostatic secretions, semen, or post-massage urine.
- IIIB (non-inflammatory) — no inflammatory cells. This is essentially a pain syndrome without objective prostatic inflammation.
The cause of CPPS remains incompletely understood. Current theories include: pelvic floor muscle dysfunction (the most evidence-based), neural sensitization, autoimmune inflammation, prior infection with persistent inflammatory changes, and psychological stress amplification [7]. In practice, the cause is likely multifactorial and varies between patients.
The critical point: repeated courses of antibiotics are NOT the answer for CPPS. If two courses of appropriate antibiotics have not resolved symptoms, continuing to prescribe antibiotics is futile and potentially harmful (antibiotic resistance, gut dysbiosis). Yet this is exactly what happens to most CPPS patients before they reach urology — they’ve been through 4, 5, sometimes 8 courses of antibiotics without improvement. If you suspect you have CPPS, the most useful first step is to objectively score your symptoms with the validated NIH-CPSI chronic prostatitis symptom index — this gives you and your doctor a number to track, and a structured framework for the consultation.
Category IV: Asymptomatic Inflammatory Prostatitis
This is an incidental finding — inflammatory cells found in prostatic tissue during biopsy for another reason, or in semen during infertility evaluation. The patient has no symptoms. No treatment is needed unless the inflammation is affecting fertility.
Related Read: UTI in Men — It’s Not Normal. Here’s When to WorryProstatitis and PSA: The Anxiety Trap
Here is the scenario that brings the most distress to young men: a primary care doctor checks a PSA level during a prostatitis workup, finds it elevated, and now the patient is convinced he has cancer. This happens more often than it should.
Prostatitis can raise PSA dramatically — sometimes to 10, 20, or even 50+ ng/mL in acute bacterial cases. The inflammation disrupts the prostatic epithelial barrier, allowing PSA to leak into the bloodstream in much higher concentrations than normal [8].
The clinical guideline is clear: PSA should not be checked during active prostatic inflammation. If it was already checked and found to be elevated, it should be repeated 6-8 weeks after treatment, once the inflammation has resolved. In the vast majority of young men with prostatitis, the PSA returns to normal. If it remains elevated after treatment, further investigation (including MRI) may be warranted — but this is the exception, not the rule. You can put your specific PSA value into context with our age-adjusted PSA interpreter to see whether your number is genuinely outside the expected range for your age, or simply elevated because of inflammation.
The bottom line: prostatitis symptoms in young men and elevated PSA is almost certainly caused by the inflammation, not by cancer. Prostate cancer under age 40 is extraordinarily rare.
Related Read: My PSA Is 4.5 — Do I Have Cancer? Understanding Grey Zone ResultsIn My Practice
The typical referral I receive for prostatitis looks like this: a man between 25 and 40, often a young professional, who has been treated with three or more courses of ciprofloxacin by his primary care doctor without ever sending a urine culture. By the time he reaches me, he has WebMD open on his phone, is convinced he has cancer, and sometimes has been told to worry because his PSA “came back elevated.” The first thing I do — before examining him, before ordering tests — is explain clearly and with certainty that this is not cancer, that prostatitis elevates PSA in exactly the way he has experienced, and that the PSA will normalize once the inflammation settles.
The relief on a patient’s face when a urologist tells him plainly that he does not have cancer is something I encounter almost every week in this clinic — and the reason this article exists is to short-circuit that anxiety as early as possible.
Months of pelvic pain and no real answers? Download Dr. Khalid’s Chronic Prostatitis / CPPS Guide.
Enter your email below to receive Dr. Khalid’s complete Chronic Prostatitis / CPPS Guide as a free, printable PDF.
How CPPS Is Actually Treated (When Antibiotics Aren’t the Answer)
The treatment of Category III CPPS is where urology struggles the most — and where patients suffer the most from ineffective management. There is no single magic bullet. The EAU guidelines recommend a multimodal, phenotype-directed approach based on the predominant symptom domain [5].
The practical framework I use in clinic is the UPOINT system, which categorizes symptoms into six domains and targets each with specific interventions [9]. The reason this matters: men with CPPS who are managed with a phenotype-directed strategy improve at meaningfully higher rates than those given the standard “another antibiotic course” approach.
U — Urinary symptoms. If frequency, urgency, or poor flow dominate, alpha-blockers (tamsulosin, alfuzosin) are first-line. These relax the smooth muscle of the prostate and bladder neck, reducing obstruction and irritation. Treatment should continue for at least 6-12 weeks before assessing response — stopping at 2-3 weeks because “it’s not working” is the most common error.
P — Psychosocial. Anxiety, depression, and catastrophizing are common in CPPS and significantly amplify pain perception. Cognitive behavioral therapy (CBT), stress management, and in some cases antidepressants (amitriptyline, duloxetine) address this domain. The psychological component is not “in the patient’s head” — it is a real neurobiological phenomenon where central pain sensitization amplifies pelvic signals. I now routinely ask about life stressors during the CPPS consultation, and I have noticed repeatedly that patients under significant occupational or personal stress experience disproportionately severe symptom flares. Addressing this domain is foundational, not optional.
O — Organ-specific (prostatic). If the prostate itself is the primary pain source (tenderness on DRE, improvement with ejaculation or prostatic massage), a trial of quercetin (a bioflavonoid with anti-inflammatory properties) or pollen extract (Cernilton) may be considered. Evidence is limited but these are low-risk interventions [10].
I — Infection. Only if there is genuine microbiological evidence of infection should antibiotics be used. One properly directed course of a fluoroquinolone for 4-6 weeks. If two courses fail, stop prescribing antibiotics — the condition is not bacterial.
N — Neurological / systemic. Central sensitization and neuropathic pain components may respond to pregabalin, gabapentin, or tricyclic antidepressants at low doses.
T — Tenderness (pelvic floor). This is increasingly recognized as the most important domain. Pelvic floor muscle dysfunction — chronic tension and trigger points in the levator ani, obturator internus, and perineal muscles — is present in the majority of CPPS patients [7]. Treatment involves specialized pelvic floor physiotherapy — but the type matters. When you book the appointment, ask specifically for myofascial release, trigger point therapy, biofeedback, and paradoxical relaxation training. Standard “Kegel exercises” are the wrong intervention for CPPS — they can actually worsen symptoms by further tightening already hypertonic muscles. In my practice I have found that even teaching patients a simple pelvic floor awareness and relaxation sequence — emphasizing release rather than contraction — produces meaningful benefit in a subset of CPPS patients, particularly those whose pain is provoked by sitting or stress.
Score Your Symptoms: NIH-CPSI Chronic Prostatitis Symptom IndexWhat Prostatitis Is NOT: Myths That Need Correcting
Myth: Prostatitis is caused by too much (or too little) sex
There is no evidence that sexual frequency causes prostatitis. Acute bacterial prostatitis is caused by bacteria ascending the urethra or refluxing from infected urine — not by sexual activity itself. CPPS has no established relationship with sexual frequency. Regular ejaculation may actually help some CPPS patients by reducing prostatic congestion, though this varies individually.
Myth: Prostatitis is an STI
Standard prostatitis is not a sexually transmitted infection. The most common causative bacteria (E. coli, Klebsiella) are gut organisms, not STI pathogens. However, Chlamydia trachomatis and Neisseria gonorrhoeae can occasionally cause prostatitis in younger men — which is why STI screening is part of the workup, but the vast majority of cases are not sexually transmitted.
Myth: Prostatitis leads to prostate cancer
There is no proven causal link between prostatitis and prostate cancer [11]. Some epidemiological studies have suggested a weak association, but this may reflect detection bias (men with prostatitis get more PSA tests and biopsies, leading to more cancer diagnoses). Prostatitis should not trigger cancer screening beyond age-appropriate guidelines.
Myth: You can “cure” CPPS with the right antibiotic
If no bacteria are found, antibiotics cannot cure the condition. Repeated antibiotic courses are the single most common treatment error in CPPS management. The condition requires a multimodal approach targeting pain, muscle dysfunction, urinary symptoms, and psychosocial factors simultaneously. The men who do best with CPPS over time are those who accept early that this is a chronic pain management condition, not an infection that will be cured with the next prescription.
When to See a Doctor — Urgently
Red Flags — Get Same-Day Care
- High fever (above 38.5°C / 101.3°F) with perineal pain and difficulty urinating — this suggests acute bacterial prostatitis, which can progress to sepsis and requires emergency IV antibiotics.
- Complete inability to urinate (urinary retention) — in the context of prostatitis, this requires urgent catheterization (suprapubic preferred over urethral).
- Rigors (uncontrollable shaking chills) — a sign of bacteremia. Present to the ER (A&E) immediately.
- Pelvic pain lasting more than 3 months that has not responded to standard antibiotic treatment — you need a urologist to evaluate for CPPS and start appropriate multimodal management.
- Recurrent UTIs with the same organism — this pattern suggests chronic bacterial prostatitis and requires specialized investigation including expressed prostatic secretion cultures.
Frequently Asked Questions
Can prostatitis affect fertility?
Potentially, yes. Both acute and chronic bacterial prostatitis can impair semen quality by introducing inflammatory cells, bacteria, and reactive oxygen species into the seminal fluid. Category IV (asymptomatic inflammatory prostatitis) discovered during infertility workup may also contribute. However, the relationship is not straightforward — many men with prostatitis have normal fertility. If you are trying to conceive and have prostatitis symptoms, a semen analysis and treatment of any active infection is warranted. The NIH-CPSI score can help your doctor track whether your symptoms are improving with treatment.
How long do prostatitis symptoms in young men typically last?
Acute bacterial prostatitis (Category I) typically resolves with 4-6 weeks of appropriate antibiotics, though full recovery may take 2-3 months. Chronic bacterial prostatitis (Category II) may require months of treatment and can recur. CPPS (Category III) is by definition chronic — lasting at least 3 months — and in some patients persists for years with fluctuating severity. With appropriate multimodal treatment, most CPPS patients achieve significant symptom improvement, though complete resolution is not always possible. Track your symptom score every 4-6 weeks to give your urologist objective data on whether your treatment plan is working.
Does prostatitis cause erectile dysfunction?
Indirectly, yes — particularly CPPS. Pain during or after ejaculation, pelvic discomfort, and the psychological impact of chronic pain can all contribute to erectile and sexual dysfunction. Studies show that men with CPPS report significantly higher rates of ED and reduced sexual satisfaction compared to the general population [12]. Treating the underlying CPPS typically improves sexual function as well. If your ED is the dominant symptom rather than the pelvic pain, the workup direction may shift accordingly.
Should I avoid sitting if I have prostatitis?
Prolonged sitting can worsen CPPS symptoms because it compresses the perineum and increases pelvic floor muscle tension. Practical strategies include: using a cushion with a perineal cut-out (donut cushion), taking standing breaks every 30-45 minutes, and avoiding cycling until symptoms improve. These are supportive measures alongside definitive treatment, not cures in themselves. Many of my patients see meaningful improvement just from changing how long they sit at a desk in a single block.
Is a prostate biopsy needed for prostatitis?
Almost never. Biopsy is not part of the standard prostatitis workup. It may be considered only if PSA remains elevated after inflammation has been treated and resolved, or if there are other features raising genuine concern for malignancy. Typical prostatitis symptoms in young men and an elevated PSA, the appropriate action is to treat the prostatitis and recheck PSA after 6-8 weeks — not to biopsy. Use our age-adjusted PSA interpreter to put your number in context first.
Should I push my doctor for a urine culture if I’m being treated for prostatitis without one?
Yes — and this is one of the most important things you can do. The most common error in prostatitis management is empirical antibiotic prescribing without ever sending a culture. If no bacteria are growing, antibiotics cannot work, and you need to be re-classified as CPPS rather than receive a third or fourth antibiotic course. Ask specifically for either a mid-stream urine culture or, if your doctor suspects chronic bacterial prostatitis, a post-prostatic massage urine culture (the simplified 2-glass test). Bring this article to the appointment if it helps frame the request — most primary care doctors respond well to a patient who knows what investigation they need.
References
- Krieger JN, et al. NIH consensus definition and classification of prostatitis. JAMA. 1999;282(3):236-237. PubMed
- Collins MM, et al. Prevalence and correlates of prostatitis in the health professionals follow-up study cohort. J Urol. 2002;167(3):1363-1366. PubMed
- Nickel JC. Classification and diagnosis of prostatitis: a gold standard? Andrologia. 2003;35(3):160-167. PubMed
- Weidner W, et al. Acute bacterial prostatitis — etiology, diagnosis and therapy. J Urol. 2007;177(6):2050-2057. PubMed
- EAU Guidelines on Urological Infections. European Association of Urology. 2024. EAU
- Nickel JC, Shoskes DA. Phenotypic approach to the management of chronic prostatitis/chronic pelvic pain syndrome. Curr Urol Rep. 2009;10(4):307-312. PubMed
- Anderson RU, et al. Integration of myofascial trigger point release and paradoxical relaxation training in men with chronic pelvic pain syndrome. J Urol. 2005;174(1):155-160. PubMed
- Nadler RB, et al. Effect of inflammation and benign prostatic hyperplasia on elevated serum prostate specific antigen levels. J Urol. 1995;154(2):407-413. PubMed
- Shoskes DA, et al. Phenotypically directed multimodal therapy for chronic prostatitis/chronic pelvic pain syndrome: a prospective study using UPOINT. Urology. 2010;75(6):1249-1253. PubMed
- Shoskes DA, et al. Quercetin in men with category III chronic prostatitis: a preliminary prospective, double-blind, placebo-controlled trial. Urology. 1999;54(6):960-963. PubMed
- Sfanos KS, De Marzo AM. Prostate cancer and inflammation: the evidence. Histopathology. 2012;60(1):199-215. PubMed
- Liang CZ, et al. The relationship between chronic prostatitis and erectile dysfunction. J Androl. 2011;32(5):496-501. PubMed

Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.