Overactive Bladder in Men: Symptoms & Real Treatment
Most men dealing with sudden, uncontrollable urges to pee have been told for years that it's "just their prostate." The reality is, if you treat an overactive bladder with standard prostate pills, you will stay miserable—and might end up having surgery you don't need. Here is how to finally tell the difference, and the exact treatments that actually work.

Most men think overactive bladder is a women’s condition. It isn’t. In my urology clinic, roughly one in six men over 40 meets the diagnostic criteria for overactive bladder in men — yet the majority have been told their symptoms are “just BPH,” “just aging,” or “just a small prostate problem.” The result: men sit with urgency, frequency, and night-time wakeups for years before anyone uses the correct label or starts the correct treatment. The reason this matters is simple. OAB and an enlarged prostate are not the same condition. They overlap, they can coexist, and the treatments differ. If a urologist treats your symptoms as BPH when the underlying problem is detrusor overactivity, the medication will not work — and you will be told the next step is surgery you may not need.
Key Takeaways
- OAB in men is real and underdiagnosed — affecting 10–16% of men over 40, with prevalence climbing steeply after 60 per AUA 2024 data.
- Urgency is the defining symptom, not frequency. A diagnosis of overactive bladder requires sudden compelling urge to urinate, with or without leakage, in the absence of infection.
- OAB and BPH overlap in 50–75% of older men — which is why prostate medication alone often fails to fix night-time wakeups and urgency.
- First-line treatment is behavioral, not pharmacological. Bladder training, timed voiding, and fluid management resolve symptoms in roughly 60% of motivated patients within 8–12 weeks.
- Mirabegron and vibegron (beta-3 agonists) have replaced anticholinergics as the preferred first-line drug class in older men due to a substantially lower dementia risk signal.
What Overactive Bladder Actually Is
Overactive bladder is a clinical syndrome, not a single disease. The International Continence Society and the American Urological Association define it as urinary urgency — a sudden, compelling desire to urinate that is difficult to defer — usually accompanied by frequency and nocturia, with or without urge incontinence, in the absence of urinary tract infection or other obvious cause.[1] The defining word is urgency. A man who urinates 10 times a day without ever feeling a sudden, compelling need does not have OAB. He has frequency from another cause — most commonly excess fluid intake, diabetes, or prostate-related bladder outlet obstruction.
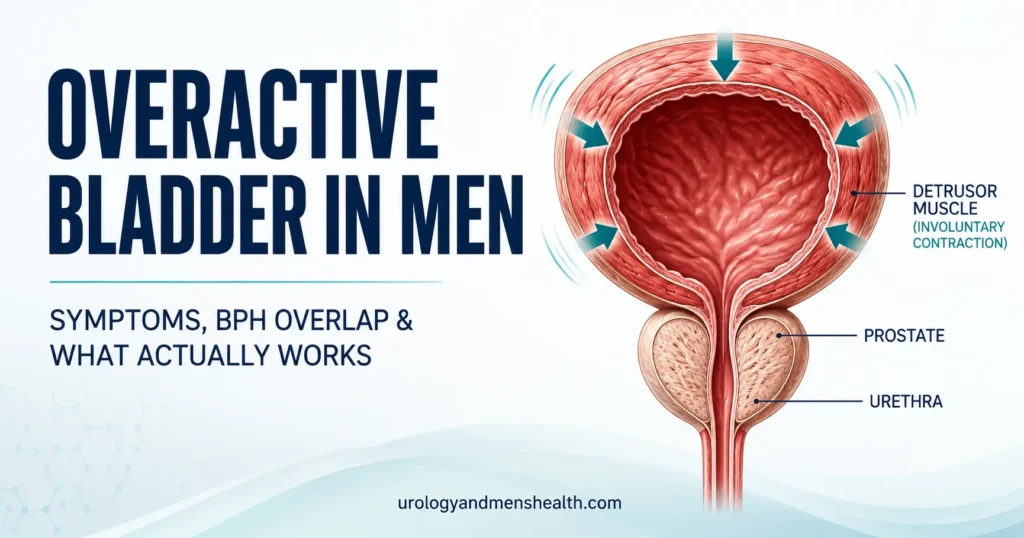
Mechanistically, OAB is detrusor overactivity. The detrusor is the smooth muscle wall of the bladder. In a healthy bladder, the detrusor stays relaxed as urine fills, then contracts on command when you reach the bathroom. In an overactive bladder, the detrusor contracts involuntarily during filling — sometimes at volumes as low as 100–150 mL (about 3.4–5 fl oz), well below the normal 400–500 mL capacity. Those involuntary contractions are felt as urgency. If the urethral sphincter cannot hold against the contraction, the result is urge incontinence.
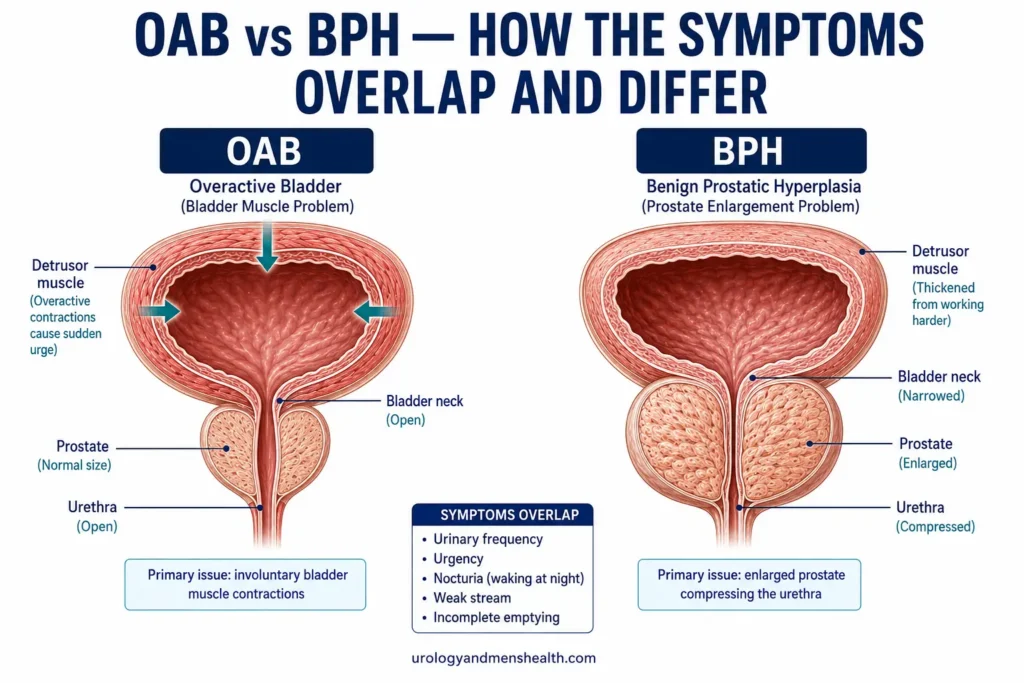
This is fundamentally different from benign prostatic hyperplasia (BPH), where the problem is mechanical obstruction at the bladder outlet. The two conditions produce overlapping symptoms because chronic obstruction eventually irritates the detrusor and causes secondary overactivity — but the primary fix is different. BPH responds to alpha-blockers and 5-alpha reductase inhibitors that target the prostate. OAB responds to drugs that calm the detrusor and to behavioral therapy that retrains the urge response.
The Symptom Cluster: What Qualifies as OAB
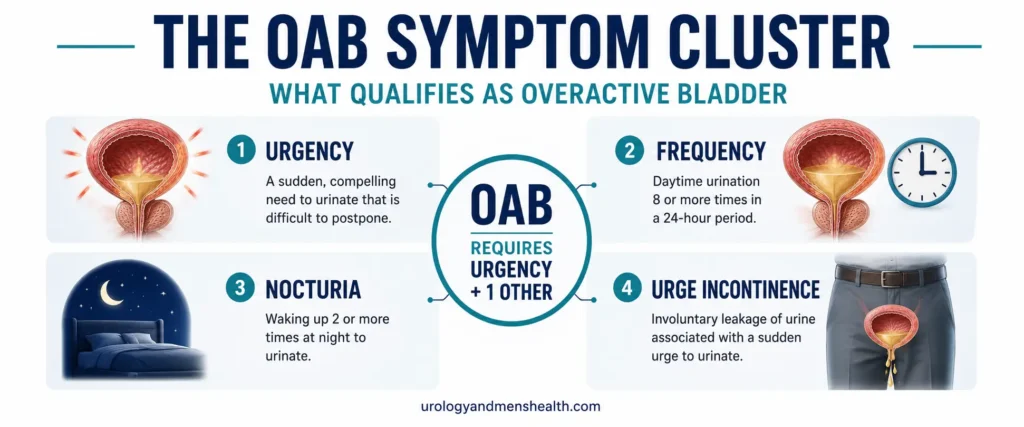
OAB has four cardinal symptoms. Urgency is mandatory; you need urgency plus at least one of the other three to meet the diagnosis.
- Urgency — a sudden, compelling desire to urinate that is hard to defer. Not the same as “I should probably go before the meeting.” Urgency is the feeling that if you don’t move now, you will leak.
- Frequency — more than 8 daytime voids in a 24-hour period, in the context of normal fluid intake (around 2 liters or 70 fl oz daily). Frequency without urgency usually points elsewhere.
- Nocturia — waking 2 or more times per night specifically to urinate. One wakeup is within normal limits for men over 60. Two or more, every night, is pathological. Nocturia has its own diagnostic workup because the differential is broader than OAB alone.
- Urge incontinence — leakage that occurs at the moment of urgency, before you reach the bathroom. Present in roughly one-third of men with OAB and called “OAB-wet.” The remainder have “OAB-dry.”
Symptoms that do not belong to OAB include weak stream, hesitancy, straining, intermittent flow, and the sensation of incomplete emptying. Those are obstructive symptoms and point toward BPH, urethral stricture, or — rarely — bladder outlet pathology. Many men have both pictures simultaneously, which is why a thorough history matters more than a single symptom.
In My Practice
A 58-year-old man came to clinic two years ago convinced he had prostate cancer. His symptom was night-time urgency so severe he was setting alarms to pre-empt the urge and still leaking on the way to the bathroom three nights a week. His previous GP had given him tamsulosin for six months. It had done nothing. His PSA was 1.4 ng/mL, his prostate volume was 32 mL on ultrasound — barely enlarged — and his uroflowmetry showed a normal peak flow of 18 mL/sec. This was not BPH. This was pure OAB with urge incontinence, and tamsulosin was the wrong drug class entirely.
The lesson I tell every patient: if a prostate drug hasn’t worked in 8–12 weeks, the diagnosis is probably wrong — not the dose.
Why OAB Is Missed in Men: The BPH Overlap
Population data from the EpiLUTS study estimated that around 27% of men in the United States report at least one OAB symptom, and 10–16% meet full diagnostic criteria.[2] Yet men receive a formal OAB diagnosis at roughly one-third the rate of women with equivalent symptoms. The reason is structural: when a man walks into primary care with urgency, frequency, and nocturia, the reflex diagnosis is “prostate.” The reflex prescription is an alpha-blocker. And because alpha-blockers do help a subset of mixed OAB/BPH cases by reducing outlet resistance, the partial response gets read as confirmation.
This matters because the conditions coexist in more than half of older men. AUA/SUFU 2024 guidance acknowledges this and recommends that men with persistent storage symptoms after alpha-blocker treatment be specifically evaluated for OAB, not pushed straight to TURP or other prostate surgery.[1] The reverse is also true: men diagnosed with OAB who have a significantly enlarged prostate need their outlet obstruction addressed because the chronic high pressure perpetuates the detrusor overactivity. Treating one without the other leaves symptoms half-solved.
Two clinical signals point toward OAB rather than pure BPH: (a) symptoms that are storage-dominant — urgency, frequency, nocturia — with minimal hesitancy or weak stream, and (b) urge incontinence. A man who never has to wait or strain to start urinating but feels he has 30 seconds from urge to the toilet has OAB physiology until proven otherwise.
What Causes Detrusor Overactivity
The honest answer is that in most men with OAB, no single cause is ever identified. This is called idiopathic OAB and accounts for the majority of cases. The detrusor becomes hypersensitive, the urge signaling pathway in the spinal cord and brainstem becomes upregulated, and the bladder fires before it should. Why this happens is incompletely understood, but several contributors are well-documented:
- Bladder outlet obstruction from BPH — chronic high-pressure voiding causes detrusor hypertrophy and secondary overactivity over years
- Neurological disease — Parkinson’s disease, multiple sclerosis, stroke, and spinal cord injury directly cause neurogenic detrusor overactivity, which is a distinct subtype
- Type 2 diabetes — autonomic neuropathy alters bladder sensation and detrusor function; OAB prevalence is roughly double in diabetic men
- Excess caffeine and alcohol — direct bladder irritants and diuretics that worsen urgency in a dose-dependent way
- Constipation and pelvic floor dysfunction — a chronically loaded rectum directly compresses the bladder and triggers urgency
- Sleep apnea — obstructive sleep apnea drives nocturnal polyuria via atrial natriuretic peptide release, masquerading as nocturnal OAB
- Aging — detrusor afferent nerves become more sensitive and bladder capacity declines progressively after 50
Identifying contributors matters because removing them often resolves OAB without medication. A man who drinks 6 cups of coffee a day and 3 beers a night does not need mirabegron — he needs to drop the caffeine to 2 cups and the alcohol to weekends, and reassess in 4 weeks.
Tired of mapping every bathroom on your commute?
Download Dr. Khalid’s complete Men’s Health Screening Checklist — a free, printable PDF covering the 5 tests every man over 40 should know about, including bladder and prostate workup.
How OAB Is Diagnosed: The Workup You Should Expect
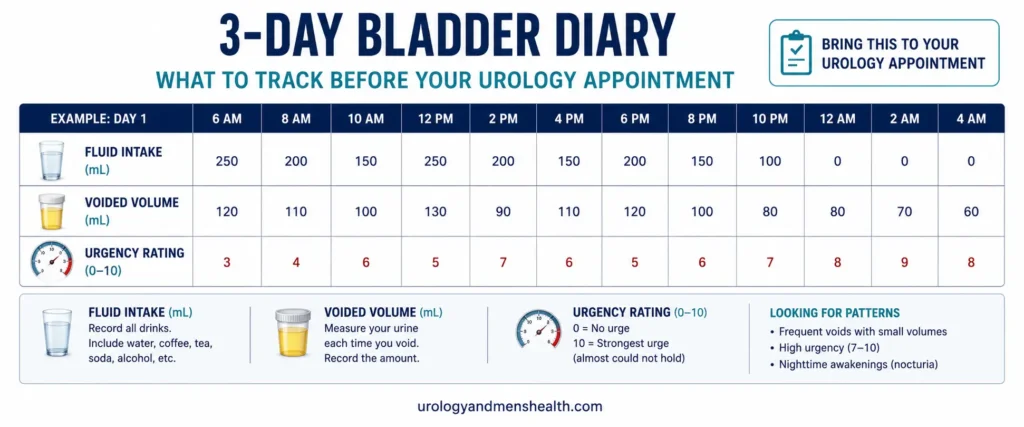
OAB is a clinical diagnosis based on symptoms, supported by a focused workup designed to rule out other conditions. AUA/SUFU 2024 guidelines specify the minimum evaluation: history, physical exam (including a digital rectal exam in men), urinalysis, and a bladder diary.[1] If those are unremarkable and symptoms fit, OAB is the diagnosis. Imaging and urodynamic testing are reserved for complicated or refractory cases.
The 3-day bladder diary is the most useful single test and the one most often skipped. It captures fluid intake, voided volumes, and urgency or leakage episodes over 72 consecutive hours. Patterns reveal themselves immediately: a man who voids 50–100 mL ten times a day has a small functional capacity consistent with OAB; a man who voids 400 mL three times a day plus 800 mL overnight has nocturnal polyuria, not OAB. Bring the diary to your appointment — it changes the conversation entirely.
Urinalysis rules out the conditions that mimic OAB: urinary tract infection, glycosuria from undiagnosed diabetes, and microscopic hematuria that warrants further workup for bladder pathology. Post-void residual measurement — done with a bladder ultrasound — checks how much urine is left after urination. A residual over 150 mL (about 5 fl oz) suggests bladder outlet obstruction or detrusor underactivity rather than pure OAB. You can estimate your post-void residual significance with our calculator before your appointment.
Cystoscopy and urodynamic testing are not routine. They are indicated when there is hematuria, a history of bladder cancer risk factors, persistent symptoms despite second-line treatment, or planned advanced therapies like Botox or sacral neuromodulation.
Treatment Step 1: Behavioral Therapy (Where Real Improvement Happens)
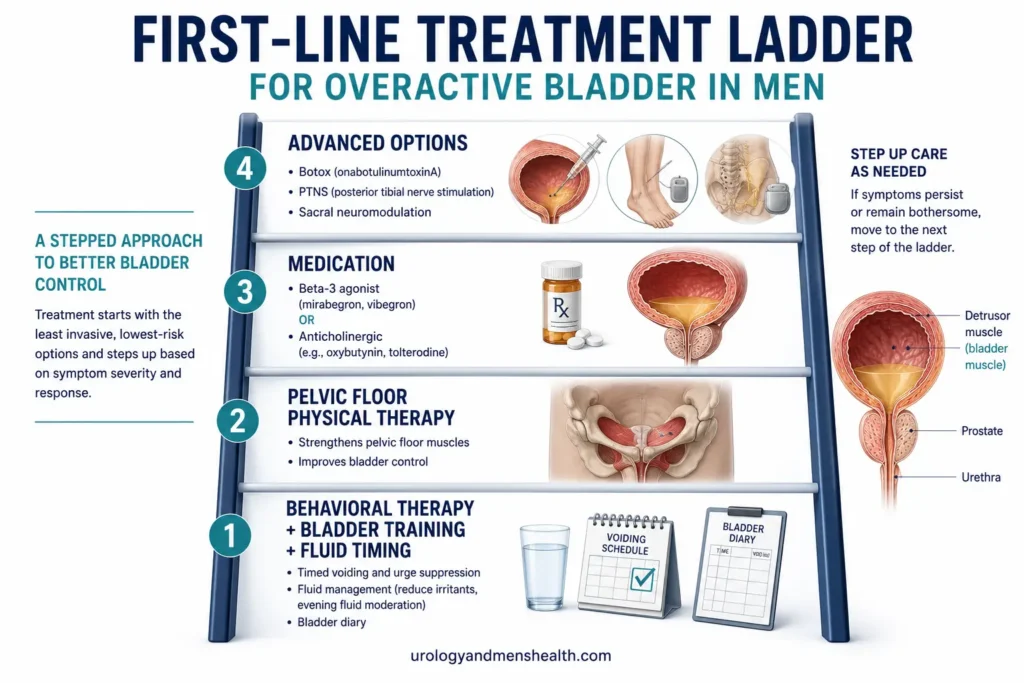
AUA/SUFU 2024 guidelines list behavioral therapy as first-line treatment for OAB — ahead of medication.[1] This is not a gentle suggestion. The data supporting behavioral therapy as monotherapy is genuinely strong: in motivated patients who complete a structured 8–12 week program, around 60% achieve clinically meaningful symptom reduction without any drug.[3] The reason this gets skipped is that it requires patient effort over weeks rather than a prescription that takes 30 seconds to write.
Four components matter most:
- Fluid management. Total daily intake of 1.5–2 liters (50–70 fl oz). No more, no less. Front-load fluids in the morning and afternoon; stop drinking 3 hours before bed. Eliminate caffeine after noon and cap total caffeine at the equivalent of 2 cups of coffee per day. Cut alcohol — every reduction below 2 drinks per day improves nocturia within 2 weeks.
- Timed voiding. Urinate on a schedule — every 2 hours during the day — regardless of urge. The goal is to empty the bladder before it triggers an urgency episode. After 2–3 weeks, lengthen the interval by 15 minutes weekly until you reach a 3–4 hour cycle.
- Urge suppression. When urgency strikes, do not run to the bathroom. Stop. Sit if possible. Contract the pelvic floor 5–10 times quickly. The pelvic floor reflexively inhibits the detrusor — this is real neurophysiology, not a relaxation technique. Wait until the urge subsides, then walk calmly to the bathroom.
- Pelvic floor training. Daily Kegel exercises strengthen the inhibitory reflex over 8–12 weeks. Three sets of 10 contractions, each held for 5 seconds, daily. Done correctly, this is the single highest-yield exercise for OAB in men.
Behavioral therapy works because OAB is partly a learned reflex pattern. The bladder has been signaling urgency at lower and lower volumes for years and the brain has accepted those signals as legitimate. Retraining is slow but durable — and unlike medication, the benefits persist after treatment ends.
Treatment Step 2: Medication — What Actually Works in 2026
If behavioral therapy alone is insufficient after 8–12 weeks, medication is added. AUA/SUFU 2024 substantially reshaped the drug ladder. The headline change: beta-3 agonists are now preferred first-line over anticholinergics in older men, primarily because of the accumulating evidence on anticholinergic burden and dementia risk.[1]
- Beta-3 agonists (preferred first-line): Mirabegron 25–50 mg daily or vibegron 75 mg daily. Both relax the detrusor through beta-3 adrenergic receptors. Side effects are limited — modest blood pressure elevation in some users, occasional headache. No cognitive effects. Vibegron in particular has shown clean tolerability data in trials.[4]
- Anticholinergics (second-line in older men): Oxybutynin, tolterodine, solifenacin, darifenacin, trospium, fesoterodine. Effective for symptom control but carry dry mouth, constipation, blurred vision, and — most importantly — a documented association with increased dementia risk with long-term use in adults over 65.[5] Trospium and darifenacin cross the blood-brain barrier least and are preferred when an anticholinergic is needed in an older man.
- Combination with an alpha-blocker: Men with mixed OAB/BPH may need tamsulosin plus a beta-3 agonist. The combination targets both outlet obstruction and detrusor overactivity. Tamsulosin has its own side-effect profile — most notably retrograde ejaculation and intraoperative floppy iris syndrome — which should be discussed before starting.
Realistic expectations matter. OAB medication typically reduces urgency episodes by 50–70% and urge incontinence episodes by a similar margin — but rarely eliminates them. A 4-week trial is the minimum before judging response; some patients need 8–12 weeks for maximal effect. If the first drug fails, the second has roughly a 30% chance of working — the response is partly idiosyncratic.
When OAB Symptoms Are Not OAB — Red Flags
The following warrant urgent urology evaluation rather than a trial of OAB therapy:
- Blood in the urine — even one episode of visible hematuria or persistent microscopic hematuria on dipstick warrants cystoscopy to exclude bladder cancer
- New-onset OAB symptoms after age 60 with weight loss, fatigue, or unexplained anemia
- Recurrent urinary tract infections — three or more in 12 months suggests an underlying structural or functional cause
- Sudden onset of urinary symptoms after a fall, back injury, or new neurological symptoms — rule out spinal cord pathology
- Suprapubic or perineal pain with urgency — suggests interstitial cystitis or chronic pelvic pain syndrome rather than OAB
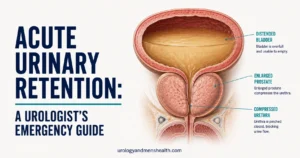
- Inability to urinate with a painful, distended bladder — acute urinary retention is an emergency
Treatment Step 3: Advanced Options When Drugs Fail
Roughly 20–30% of men do not respond adequately to behavioral therapy plus medication. AUA/SUFU 2024 guidelines specifically warn against escalating to a third or fourth oral drug — the yield drops sharply and side effects accumulate. Instead, third-line therapies are offered:
- Intradetrusor onabotulinumtoxinA (Botox). 100 units injected via cystoscope into the bladder wall under local anesthesia. Effects last 6–9 months. Roughly 60–70% of refractory OAB patients achieve significant improvement. The main risk — clean intermittent catheterization for transient urinary retention — affects around 6% of men and resolves as the Botox wears off. This is the most effective third-line option in my practice.[6]
- Posterior tibial nerve stimulation (PTNS). A weekly 30-minute session for 12 weeks, with a fine needle near the ankle delivering low-voltage stimulation that modulates the sacral nerve pathway. Roughly 60% response rate, minimal side effects, but requires ongoing maintenance sessions to sustain benefit.
- Sacral neuromodulation (Interstim, Axonics). An implanted device delivering continuous stimulation to the S3 nerve root. Requires a staged procedure — test phase first, permanent implant if effective. Long-term durability is excellent, with 5-year continued response in 60–70% of patients.
Surgery for OAB itself — bladder augmentation — is reserved for severe refractory cases with confirmed urodynamic detrusor overactivity and significantly impaired quality of life despite all other treatments. It is rarely needed in men.
Lifestyle Factors That Move the Needle
Several lifestyle interventions have measurable effects on OAB symptoms — independent of medication:
- Weight loss. A 5–10% body weight reduction reduces urgency episodes by 30–50% in overweight men. The mechanism is partly mechanical — less abdominal pressure on the bladder — and partly metabolic.
- Reduce sitting time. Prolonged sitting compresses the pelvic floor and contributes to urgency and pelvic dysfunction. Sedentary behavior has measurable urological consequences beyond OAB alone.
- Treat constipation. A loaded rectum directly compresses the bladder. Daily fiber to 30 g, adequate fluids, and a regular bowel routine reduce urgency episodes more than most patients expect.
- Sleep apnea screening. Men with nocturia and snoring or witnessed apnea should be evaluated for obstructive sleep apnea. CPAP treatment reduces nocturnal voids by 50% or more in men with confirmed apnea.
- Smoking cessation. Smokers have a 2–3-fold higher rate of OAB symptoms; nicotine is a direct bladder irritant and chronic cough increases pelvic floor strain.
When to See a Urologist
Most men with mild OAB can begin behavioral therapy through primary care. Specialist referral is warranted in any of the following situations. Ask your primary care doctor to refer you to a urologist if:
- Symptoms persist after 8–12 weeks of behavioral therapy plus a first-line medication
- You have hematuria, recurrent UTIs, or any of the red flags above
- An alpha-blocker for presumed BPH has failed to resolve urgency or nocturia after 8 weeks
- Symptoms are severe enough to restrict travel, work, or social activity
- You are considering advanced therapies (Botox, neuromodulation)
What to bring to the appointment: a completed 3-day bladder diary, a current medication list, any prior urinalysis or PSA results, and a one-line statement of which symptom bothers you most. The bladder diary alone shortens the consultation by 15 minutes and dramatically improves the accuracy of the initial diagnosis.
Frequently Asked Questions
Can overactive bladder in men go away on its own?
OAB rarely resolves spontaneously, but symptoms can fluctuate significantly. Episodes worsen with stress, caffeine, alcohol, and constipation and improve when those factors are addressed. Roughly 15–20% of men with mild OAB experience symptom improvement after lifestyle changes alone over 6–12 months, but moderate-to-severe symptoms almost always need structured treatment. The longer untreated OAB persists, the more entrenched the urge-reflex pattern becomes — which is why a structured workup matters even for symptoms that feel manageable today.
What’s the difference between overactive bladder and an enlarged prostate?
An enlarged prostate (BPH) mechanically obstructs urine flow at the bladder outlet, producing hesitancy, weak stream, and the sensation of incomplete emptying. Overactive bladder in men is detrusor overactivity — the bladder muscle contracts involuntarily during filling, producing urgency, frequency, and night-time wakeups. The conditions overlap in 50–75% of older men, which is why nocturia and urgency often need both conditions addressed separately. Storage symptoms point to OAB; voiding symptoms point to BPH.
Are anticholinergic medications safe for older men with OAB?
Anticholinergics like oxybutynin and tolterodine are effective but carry a documented dementia risk signal with long-term use in adults over 65 — a roughly 30% increased risk after 3+ years of cumulative exposure. AUA/SUFU 2024 guidelines now recommend beta-3 agonists (mirabegron, vibegron) as preferred first-line drug therapy in older men for this reason. If an anticholinergic is needed, trospium and darifenacin cross the blood-brain barrier least and are the safer choices.
How long does it take for OAB treatment to start working?
Behavioral therapy and pelvic floor training take 8–12 weeks for meaningful improvement — this is muscle and reflex retraining, not a quick fix. Beta-3 agonists like mirabegron typically show benefit within 2–4 weeks, with maximal effect at 8–12 weeks. Anticholinergics work similarly. Botox produces noticeable improvement within 2 weeks and lasts 6–9 months. If a drug hasn’t produced any benefit by 4 weeks, the diagnosis or the drug choice should be reviewed — increasing the dose rarely helps.
Does drinking less water cure overactive bladder?
No — and excessive fluid restriction makes OAB worse. Concentrated urine irritates the bladder lining and amplifies urgency. The right target is 1.5–2 liters (50–70 fl oz) of total daily fluid, front-loaded earlier in the day, with caffeine and alcohol minimized. Men who restrict to under 1 liter daily develop concentrated, irritating urine and chronic mild dehydration without improving their OAB. Fluid timing matters more than total volume.
Can stress and anxiety cause overactive bladder symptoms?
Stress amplifies OAB but rarely causes it alone. The urge-suppression reflex is partly under autonomic control, and sympathetic activation lowers the threshold for involuntary detrusor contractions. Many men notice urgency spikes during anxious moments — meetings, travel, public speaking. Treating coexisting anxiety with CBT or medication does reduce OAB symptoms in this subgroup, but does not replace the standard workup. If anxiety is the primary trigger, OAB is usually still present at lower intensity outside stressful situations.
References
- Cameron AP, Chung DE, Dielubanza EJ, et al. The AUA/SUFU Guideline on the Diagnosis and Treatment of Idiopathic Overactive Bladder. Journal of Urology. 2024;212(1):11-20. AUA
- Coyne KS, Sexton CC, Vats V, et al. National community prevalence of overactive bladder in the United States stratified by sex and age. Urology. 2011;77(5):1081-1087. PubMed
- Burgio KL. Behavioral treatment of urinary incontinence, voiding dysfunction, and overactive bladder. Obstetrics and Gynecology Clinics of North America. 2009;36(3):475-491. PubMed
- Staskin D, Frankel J, Varano S, et al. Once-Daily Vibegron 75 mg for Overactive Bladder: Results of the EMPOWUR Study. Journal of Urology. 2020;204(2):316-324. PubMed
- Coupland CAC, Hill T, Dening T, et al. Anticholinergic Drug Exposure and the Risk of Dementia: A Nested Case-Control Study. JAMA Internal Medicine. 2019;179(8):1084-1093. PubMed
- Nitti VW, Dmochowski R, Herschorn S, et al. OnabotulinumtoxinA for the treatment of patients with overactive bladder and urinary incontinence: results of a phase 3, randomized, placebo controlled trial. Journal of Urology. 2017;197(2S):S216-S223. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.