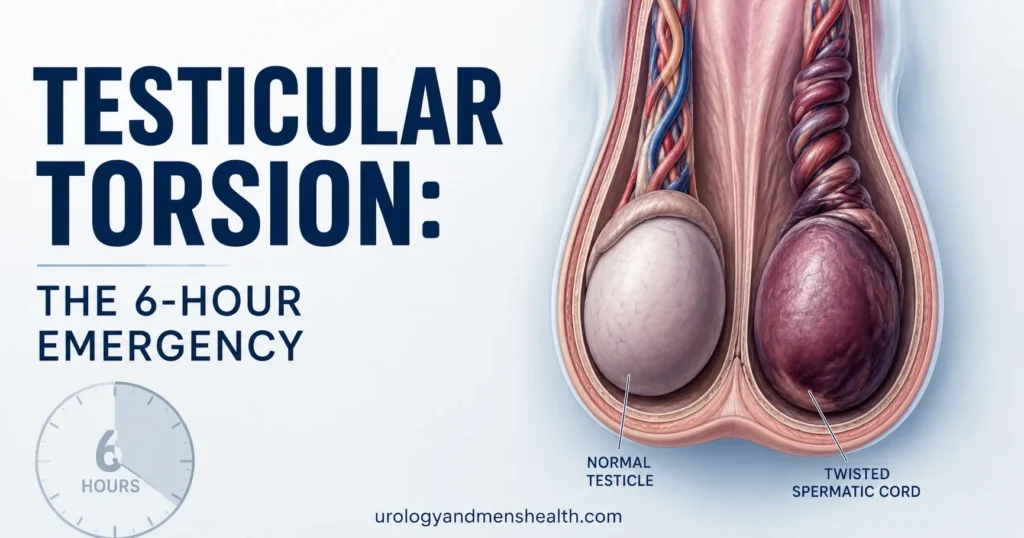
Testicular Torsion: The 6-Hour Emergency Window
Sudden one-sided testicle pain that comes on hard and won't ease isn't a strain or a bug. It's a clock — and every hour you wait is testicular tissue you won't get back. Here's how I assess and treat it in clinic.

Testicular torsion is the closest thing urology has to a stroke of the testis. A sudden twist of the spermatic cord cuts off blood supply to the testicle, and from that moment forward you have a window — measured in hours, not days — to get blood flow back before the tissue dies. I’ve operated on men whose testes were saved at hour five and on men whose testes were already lost at hour fourteen. The difference between those two outcomes was almost always a delay at home, in a waiting room, or with a wrong first diagnosis. This guide covers what testicular torsion actually is, the symptoms that mean an emergency room visit right now, what happens once you get there, and how to tell torsion apart from the conditions that mimic it. For the wider context of testicular and scrotal surgery, see our Urological Surgery & Recovery hub.
Key Takeaways
- Testicular torsion has roughly a 6-hour salvage window — within 6 hours, around 90 to 100 percent of testes are saved; after 24 hours, fewer than 10 percent are viable.
- The classic presentation is sudden, severe, one-sided scrotal pain — often waking a young man from sleep — with nausea, vomiting, and a high-riding tender testicle.
- Peak incidence is age 12 to 25, but torsion happens at any age, including newborns and men over 40.
- Surgery is the only definitive treatment. Imaging (Doppler ultrasound) confirms when uncertainty exists but should never delay theatre when clinical suspicion is high.
- Bilateral orchidopexy — fixing both testicles surgically — is standard, because the anatomical defect (bell-clapper deformity) is usually bilateral.
What Testicular Torsion Actually Is
Each testicle hangs inside the scrotum suspended by the spermatic cord — a bundle that carries the testicular artery, veins, vas deferens, and nerves. In testicular torsion, this cord rotates on its own axis, usually somewhere between 180 and 720 degrees. That twist physically pinches the testicular artery shut. The testis stops receiving oxygen-rich blood almost immediately. Think of it like a garden hose with a kink — flow stops at the kink, and everything downstream begins to die.
Most cases happen because of an anatomical variant called the bell-clapper deformity, where the testicle isn’t anchored properly to the inner scrotal wall. Instead of sitting like an egg in a fixed cup, it hangs like a clapper inside a bell — free to swing and rotate. Roughly 12 percent of men have this anatomy on at least one side, and most never know it. When torsion happens, it’s typically because that loose testicle rotated during sleep, sports, or sometimes for no identifiable reason at all.
There are two main types. Intravaginal torsion is what we see in adolescents and young adults — the rotation happens inside the tunica vaginalis, the sac surrounding the testis. Extravaginal torsion occurs almost exclusively in newborns, where the entire testicle and its surrounding sac rotate together. The presentation and urgency differ slightly, but the principle is identical: cord twisted, blood flow stopped, tissue dying by the hour.[1]
The Symptoms That Mean Get to an ER Now
The hallmark of testicular torsion is sudden, severe, unilateral scrotal pain. Not a dull ache that built over a day. Not soreness that started after sex or exercise. A pain that turns up in minutes, often peaks within an hour, and is bad enough to stop a young man in his tracks. About half of cases begin during sleep — a man wakes up in the middle of the night with one testicle on fire.
The pain is typically accompanied by:
- Nausea and vomiting in 70 to 90 percent of cases — the visceral pain signal from a torsed testis is so strong it activates the vomiting reflex.
- Lower abdominal or groin pain — because the testis develops in the abdomen embryologically and shares its nerve supply, torsion pain often refers upward. I’ve seen men diagnosed with appendicitis or kidney stones for hours before someone examined the scrotum.
- A high-riding testicle on the affected side — the twisted cord shortens, pulling the testis upward.
- A horizontal lie — the testis sits transversely rather than vertically.
- Absent cremasteric reflex — stroking the inner thigh normally lifts the testicle on that side; in torsion, it doesn’t.
- Tender, swollen scrotum that may look red or bruised within hours.
Two things to understand. First, fever is uncommon early on — if a young man has scrotal pain plus high fever, epididymitis or an infection is more likely. Second, partial or intermittent torsion exists — the testis twists, untwists spontaneously, then re-twists. Men with this history report previous episodes of brief severe pain that resolved on their own. This is not reassurance. It is a warning sign that fixation surgery is needed before the next twist becomes the permanent one.[2]
When to Go to the ER — Don’t Wait
If you have sudden severe pain in one testicle, go to the emergency room immediately. Do not wait until morning. Do not call a primary care doctor for an appointment. Do not drive yourself if the pain is severe — have someone else drive, or call an ambulance.
- Sudden onset of one-sided testicle pain, especially if it woke you from sleep
- Pain with nausea or vomiting
- One testicle clearly higher than the other or lying sideways
- Scrotal swelling, redness, or warmth that came on within hours
- A history of similar brief episodes that resolved on their own
Tell the triage nurse: “I think I have testicular torsion.” Those exact words trigger an emergency urology assessment. Vague descriptions can put you behind sprained ankles in the queue.
The 6-Hour Window — Why Time Defines Outcome
The “6-hour rule” is the single most important number in this entire condition. It refers to the time from onset of pain to surgical detorsion in the operating theatre. The clock starts the moment the cord twists, not the moment you arrive at hospital.
The salvage data from large international series are remarkably consistent:
- Surgery within 6 hours: 90 to 100 percent testicular salvage rate.
- Surgery at 6 to 12 hours: 50 to 70 percent salvage.
- Surgery at 12 to 24 hours: 20 to 40 percent salvage.
- Surgery beyond 24 hours: Under 10 percent — most testes are necrotic and must be removed.[3]
These numbers assume a clean 360-degree twist. The degree of rotation matters: a tighter twist (720 degrees) damages tissue faster than a looser one (180 degrees). This is why a man who arrives at hour 10 with a partial twist may still keep his testicle, while a man who arrives at hour 5 with a complete double-twist may not. We never know the degree of rotation until we operate — which is exactly why we don’t wait to find out.
In My Practice
The worst preventable losses I’ve seen in eleven years of urology are almost always the same story: a teenage boy with severe testicular pain who was sent home from a non-urology ER with antibiotics for “epididymitis” because his urine dip showed a few white cells. Twelve to eighteen hours later he comes back, worse. By the time we explore him, the testis is dusky, then black. There was nothing wrong with the original physical exam — there was something wrong with the threshold for surgical consultation.
The clinical rule I drill into trainees is simple: in any male under 30 with acute scrotal pain, torsion is the diagnosis until urology has personally ruled it out — not the lab, not the radiologist, not the ER physician working alone.
What Happens at the Hospital
Once a man with suspected testicular torsion is in the emergency room, the pathway should move fast. A focused urological history (when did the pain start, was the onset sudden, any previous episodes, any urinary symptoms, sexual history) takes two minutes. A scrotal examination — looking at testicular lie, checking cremasteric reflex, palpating for tenderness and induration — takes another two. By minute five, the urology team should be paged.
Imaging — Doppler Ultrasound
Color Doppler ultrasound is the standard imaging test. It looks for blood flow within the testicular parenchyma. Reduced or absent flow on the affected side, combined with a swollen heterogeneous testis, confirms torsion. Sensitivity is around 88 to 96 percent and specificity around 90 to 99 percent in experienced hands.[4]
Here’s the rule that matters: ultrasound should never delay surgery if clinical suspicion is high. A young man with classic symptoms goes to the operating theatre even if ultrasound is unavailable or equivocal. Imaging confirms; clinical judgement decides. AUA guidance, EAU paediatric urology guidelines, and NICE clinical knowledge summaries all agree on this point.[5]
Surgery — Detorsion and Orchidopexy
Under general anaesthesia, a scrotal incision is made (usually in the midline raphe). The testis is delivered, the cord is manually untwisted, and the testicle is then observed for a few minutes for return of color and pulsation. Warm saline-soaked gauze and papaverine are sometimes used to encourage reperfusion. If the testis pinks up, it is preserved. If it remains black and non-viable after observation, it is removed — a procedure called orchiectomy.
Whether the affected testis is saved or removed, the other testicle is also fixed. This is called bilateral orchidopexy — three or four non-absorbable sutures placed through the tunica albuginea to anchor each testis to the scrotal wall. Why both? Because the bell-clapper deformity is bilateral in around 80 percent of cases. Fixing only the symptomatic side leaves the other one statistically likely to torse later, sometimes years later. I have seen men present a second time at age 40 because their other testicle wasn’t fixed in their original teenage surgery.
Manual Detorsion
In a remote setting or when surgery is delayed, an experienced clinician may attempt manual detorsion at the bedside. The testis is rotated externally (most twists are inward; untwisting means rotating outward — “opening the book”). Pain relief is the sign it worked. This is a temporizing measure only; even if successful, the patient still needs urgent surgical fixation, because manual detorsion can be incomplete and the testicle can re-twist.
Torsion vs. Epididymitis — The Critical Differential
The single most dangerous mistake in acute scrotal pain is calling torsion “epididymitis” and treating it with antibiotics. The two can look superficially similar — both produce a swollen, painful testicle on one side. They are clinically distinct, and the differences matter enormously. For a deeper side-by-side, see our dedicated guide on torsion vs. epididymitis.
Testicular torsion typically:
- Strikes in minutes, often in sleep
- Peaks in age 12 to 25
- Produces nausea and vomiting
- Has no fever early on
- Shows a high-riding testis and absent cremasteric reflex
- Is not relieved by elevating the scrotum (Prehn’s sign negative)
Epididymitis typically:
- Builds gradually over hours to days
- Hits sexually active men or men over 50 with prostatic outflow issues
- Often produces urinary symptoms (burning, frequency, urethral discharge)
- Often presents with fever
- Shows a normal testicular position and present cremasteric reflex
- Is partially relieved by elevating the scrotum (Prehn’s sign positive)
The rule for any clinician facing uncertainty is simple: when in doubt, treat as torsion. The cost of a negative exploration is a small scrotal scar. The cost of missing torsion is a lost testicle. Other differentials that mimic torsion include hydrocele or spermatocele with sudden enlargement, incarcerated inguinal hernia, torsion of the appendix testis, and trauma — none of which produce the same clinical picture as true torsion, but all of which can confuse the picture.
After Surgery — Recovery and Fertility
Recovery from scrotal exploration with orchidopexy is straightforward. Most men go home the same day or the morning after surgery. Pain settles over 5 to 7 days with simple analgesia (paracetamol and a short course of an anti-inflammatory). A scrotal support garment helps for the first week. Expect bruising and swelling that look worse before they look better — peak bruising is usually day 3 to 4.
Typical activity restrictions:
- No heavy lifting, gym work, or contact sport for 4 to 6 weeks
- No sexual activity for 2 to 3 weeks
- Light walking from day 1 — movement reduces clot risk and aids healing
- Return to desk work in 1 week; to manual work in 4 to 6 weeks
The question every man asks me afterward is about fertility. The honest answer depends on whether the testis was saved and what its function will be over time. If the testis was salvaged and looks well-perfused, semen analyses at 3 and 6 months post-op are reasonable baselines. If the testis was removed, the remaining single testicle generally produces enough testosterone and sperm to maintain normal hormonal function and fertility in most men. However, around 30 to 50 percent of men show some reduction in sperm parameters after even a successful unilateral torsion — possibly due to an autoimmune response triggered by the ischemic insult. This is one reason fertility counseling matters even when “surgery went well.”[6]
If you’re entering family-planning years and have had a torsion, ask your urologist about a semen analysis at the 6-month mark. If you’re a parent of a teenage boy who has had torsion, the same advice applies in his early twenties. Building a relationship with a urologist for follow-up — and learning a proper monthly testicular self-exam — protects against the second-most-common scrotal emergency: a missed testicular tumor. For broader monitoring, the Men’s Health Screening Checklist tool walks through what to track at every age.
Finally, if you ever notice a painless lump in either testicle after recovery, that is a different problem entirely — see our guide on testicular lumps and cancer. Pain that comes on suddenly is torsion until proven otherwise. A lump that grew quietly is cancer until proven otherwise. Both deserve a urologist.
Frequently Asked Questions
Can testicular torsion happen without an injury or trauma?
Yes — and most cases do. Around 70 to 80 percent of testicular torsion happens without any preceding injury. The underlying cause is the bell-clapper deformity, which lets the testicle rotate freely inside the scrotum. The trigger is usually something minor or unidentifiable: turning in bed, sudden temperature change, vigorous exercise, or nothing at all. If you have acute scrotal pain, the absence of trauma does not rule out torsion.
What does testicular torsion pain actually feel like?
The pain is sudden, severe, and unilateral. Patients describe it as the worst pain they’ve ever felt — comparable to or worse than kidney stone pain — and it does not ease with rest, position, or over-the-counter painkillers. Nausea and vomiting accompany it in most cases. If the pain came on gradually over a day or longer, or if it’s tolerable with ibuprofen, it is far less likely to be true torsion and more likely to be epididymitis or muscular pain.
How quickly do I really need to get to the hospital?
Within the first 6 hours from the onset of pain, around 90 to 100 percent of testicular torsion cases are salvageable with surgery. Between 6 and 12 hours, the rate drops to 50 to 70 percent. After 24 hours, fewer than 10 percent of testes can be saved. The single most important variable in this condition is time — not which hospital, not which surgeon. Get to the nearest emergency room and use the words “testicular torsion” at triage.
Can testicular torsion fix itself without surgery?
Sometimes the cord untwists on its own — this is called intermittent or partial torsion, and it presents as brief episodes of severe pain that resolve spontaneously. This is not a reassuring scenario. It means your anatomy allows torsion, and the next twist may not untwist. Anyone with a history of episodic severe testicular pain should be referred to a urologist for elective bilateral orchidopexy to prevent the catastrophic event.
If a testicle is removed, will I still be able to have children?
In most cases, yes. A single remaining functional testicle generally produces enough sperm for fertility and enough testosterone for normal hormonal function. However, around 30 to 50 percent of men show reduced sperm parameters after a unilateral torsion, even with a successful salvage on the affected side. If fertility matters to you, ask your urologist for a semen analysis at 6 months post-op. Banking sperm before surgery is rarely possible in an emergency, but is worth discussing if torsion is recurrent or elective fixation is being planned.
What’s the recovery time after testicular torsion surgery?
Most men are home within 24 hours of surgery. Pain settles over 5 to 7 days with simple analgesia. Light walking from day 1, desk work after a week, and a return to gym, contact sport, or heavy lifting at 4 to 6 weeks. Sexual activity is generally fine after 2 to 3 weeks. Bruising peaks at day 3 to 4 and may look alarming — this is normal. Any fever, increasing redness, wound discharge, or escalating pain after the first 48 hours warrants a call to your surgeon.
References
- Sharp VJ, Kieran K, Arlen AM. Testicular Torsion: Diagnosis, Evaluation, and Management. American Family Physician. 2013;88(12):835-840. AAFP
- Eyre RC. Evaluation of acute scrotal pain in adults. UpToDate / NIH PubMed Bookshelf. 2024. NCBI Bookshelf
- Mellick LB, Sinex JE, Gibson RW, Mears K. A Systematic Review of Testicle Survival Time After a Torsion Event. Pediatric Emergency Care. 2019;35(12):821-825. PubMed
- Bandarkar AN, Blask AR. Testicular torsion with preserved flow: key sonographic features and value-added approach to diagnosis. Pediatric Radiology. 2018;48(5):735-744. PubMed
- European Association of Urology. Paediatric Urology Guidelines — Acute Scrotum. EAU Guidelines. 2024. EAU
- Arap MA, Vicentini FC, Cocuzza M, et al. Late hormonal levels, semen parameters, and presence of antisperm antibodies in patients treated for testicular torsion. Journal of Andrology. 2007;28(4):528-532. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.