5 Chronic Kidney Disease Stages: A Urologist’s Guide
Patients reading about the five stages of kidney disease online almost always end up terrified, assuming their diagnosis means their organs are already in total failure. In my clinic, the first thing I explain is that an eGFR score isn't a death sentence—it is simply a tracking metric, and many people live out their lives completely stable in the middle stages. This guide strips away the medical jargon to explain exactly what each stage actually means for your body, and how to tell if your kidney function is stable or dropping fast enough to require action today.

The phrase “chronic kidney disease stages” sends most men straight into a Google spiral, and what they find is usually either too clinical to be useful or so alarming it implies dialysis is around the corner. Neither is true for most patients. CKD is a spectrum — five stages defined by a single number, the eGFR — and where you sit on that spectrum determines almost everything: whether you need a specialist, whether your kidneys are still recoverable, and whether the symptoms you’re feeling are even from CKD at all. I see CKD patients every week in clinic, and the most common thing I tell them is this: the stage matters less than the trajectory. A stable Stage 3a at 55 is in better shape than a Stage 2 dropping fast at 45. This guide explains every stage in plain language, names the two numbers that genuinely matter, and tells you when CKD becomes the kind of problem that needs action this month — not next year.
Key Takeaways
- CKD is staged 1 through 5 by eGFR, but Stage 3a (eGFR 45-59) is where the conversation gets serious — anything earlier rarely needs a nephrologist.
- Most men with Stage 1-3a CKD feel completely normal; the absence of symptoms is the defining feature of early kidney disease, not a sign you’re fine.
- The two numbers that matter more than the stage itself are your urine albumin-creatinine ratio (UACR) and the rate of eGFR change per year.
- Three interventions slow CKD progression with the strongest evidence: blood pressure control under 130/80 mmHg, glycemic control if diabetic, and an SGLT2 inhibitor in eligible patients.
- You need urgent attention — not a routine appointment — if eGFR drops more than 5 points in 12 months, if foamy urine appears, or if ankle swelling develops with fatigue.
What Is Chronic Kidney Disease, Really?
Your kidneys are two fist-sized filters that process roughly 180 liters (about 47 gallons) of blood every day. They strip out waste, balance your electrolytes, regulate your blood pressure, and produce hormones that build red blood cells and activate vitamin D. When that filtering capacity drops below normal for three months or more — confirmed on two separate tests — that is the formal definition of chronic kidney disease.
The word “chronic” matters here. Acute kidney injury can occur in 48 hours from dehydration, contrast dye, or sepsis, and it often reverses fully with treatment. CKD is the slow version — kidney function declining steadily over months or years, usually without the patient noticing.
The marker we use to track this decline is eGFR: estimated glomerular filtration rate. It is a calculated number based on your serum creatinine, age, and sex, expressed in mL/min/1.73m². A healthy young adult sits around 100-120. The number falls naturally with age — by roughly 1 mL/min per year after age 40 — which is why an eGFR of 75 in a 70-year-old man is not the same problem as 75 in a 35-year-old.
The 2024 KDIGO guidelines, which are the international standard for kidney disease management, define CKD as either an eGFR below 60 for three months, or evidence of kidney damage (proteinuria, abnormal imaging, or biopsy findings) at any eGFR [1]. That second clause is why some patients with a normal eGFR of 95 still get labeled as having CKD — if there is protein in their urine, the damage is already underway.
Check Your Risk: BP & Kidney Damage Risk Tool →The 5 Chronic Kidney Disease Stages, Explained by eGFR
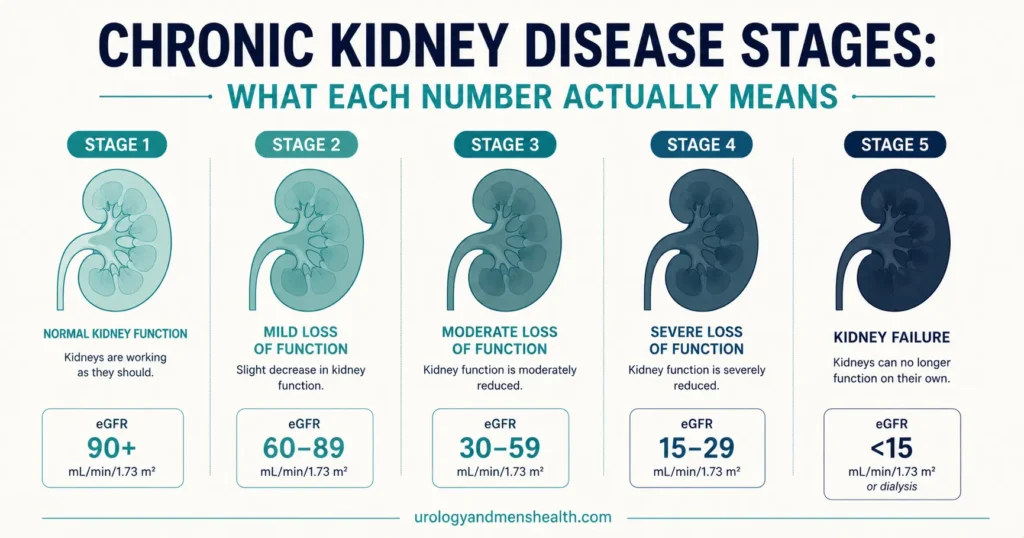
CKD has five stages, with Stage 3 split into 3a and 3b because the clinical implications differ. Here is what each stage means in practical terms.
Stage 1: eGFR 90 or above, with kidney damage
Filtration is normal, but there is structural or functional damage — usually picked up by protein in the urine or an imaging abnormality. Many men in this stage do not know they have CKD because their creatinine looks fine. The intervention here is identifying and treating the underlying cause: usually diabetes, hypertension, or recurrent kidney stones.
Stage 2: eGFR 60-89, with kidney damage
Mildly reduced filtration. Same caveat as Stage 1 — you only get this label if there is evidence of damage. An eGFR of 75 in a healthy 65-year-old with no proteinuria and no imaging changes is not CKD; it is age-appropriate filtration.
Stage 3a: eGFR 45-59 (Mild-to-moderate loss)
This is the line where CKD becomes a labeled, monitored condition that requires action. Roughly half of your kidney function is gone. Most patients still feel normal. Your primary care doctor should be checking creatinine and UACR every 6-12 months, blood pressure should be tight, and certain medications (NSAIDs, contrast dye) start needing caution.
Stage 3b: eGFR 30-44 (Moderate-to-severe loss)
This is when many men first feel a difference — fatigue, mild itching, or sleep disturbance. It is also the stage where nephrology referral becomes routine. Mineral and bone problems (low vitamin D, raised phosphate) begin to show up on bloods, and anemia from reduced erythropoietin can appear.
Stage 4: eGFR 15-29 (Severe loss)
Pre-dialysis territory. The conversation now includes preparing for kidney replacement therapy — dialysis or transplant — even if it is not yet needed. Patients in this stage need a nephrologist managing their care, not a primary care doctor doing it alone.
Stage 5: eGFR below 15 (Kidney failure)
Established kidney failure. Dialysis or transplant is required, or palliative kidney care is chosen if the patient is frail and not a candidate for replacement therapy. Symptoms — nausea, breathlessness, swelling, cognitive change — are typically prominent by this stage.
Calculate Your Stage: eGFR Calculator →CKD Symptoms: Why Stages 1-3a Often Feel Like Nothing
Here is the single most important thing to understand about CKD symptoms: your kidneys have enormous reserve capacity. You can lose 50% of total kidney function before any symptom appears, and even at 50% loss, most men still feel completely well. By the time symptoms force a doctor’s visit, the eGFR is usually below 30 — and a great deal of damage has already accumulated.
This is why CKD is sometimes called a “silent” disease. It is also why nearly 90% of US adults with CKD do not know they have it, according to CDC surveillance data [2].
Symptoms in Stage 3b and beyond
When symptoms do appear, they tend to come in clusters. The most common patterns I see in clinic:
- Fatigue that doesn’t lift with sleep — from anemia and toxin build-up, usually the first symptom mentioned.
- Foamy or bubbly urine — protein leaking into the urine. Persistent foaming that doesn’t disperse is meaningful.
- Ankle and lower-leg swelling — fluid retention from reduced filtration and protein loss.
- Itching — particularly at night, from raised phosphate and uremic toxins.
- Poor appetite, metallic taste, nausea — uremia accumulating, typically Stage 4-5.
- Breathlessness on exertion — fluid overload or anemia, often the combination.
- Nocturia — waking 2 or more times per night to urinate, often dismissed as prostate-related.
In My Practice
I had a patient in his late 50s — a long-distance trucker — who came in with what he assumed was a prostate problem. He was waking three or four times a night to urinate and putting it down to the BPH symptoms his cousin had described. His IPSS was actually only 6, which is mild. His creatinine, when we checked it, gave an eGFR of 38. That’s Stage 3b, and the nocturia was almost entirely from loss of urinary concentrating ability, not his prostate. Once we tightened his BP, started an SGLT2 inhibitor, and treated the contributing hypertension properly, his nocturia improved within four months.
The pattern I want men to remember: nocturia in a 50+ year-old is more likely to be a kidney or BP problem than a pure prostate one. Always check both.
The Two Numbers That Matter More Than the Stage Itself
If you take only one thing from this article, take this: knowing your CKD stage is incomplete information. Two patients with identical eGFRs can have completely different five-year outcomes. The numbers that actually predict your trajectory are these.
Number 1: Your urine albumin-creatinine ratio (UACR)
This is a simple urine test that measures how much protein is leaking through your kidney filters. It is the single strongest predictor of CKD progression — stronger than eGFR alone [3]. Categories:
- A1 (Normal): UACR less than 30 mg/g
- A2 (Moderate): UACR 30-300 mg/g — “microalbuminuria”
- A3 (Severe): UACR above 300 mg/g — “macroalbuminuria”
A man with Stage 3a CKD and A1 albuminuria has a markedly different risk profile than a man with Stage 2 CKD and A3 albuminuria. The KDIGO “heatmap” combines eGFR and UACR to assign a risk category (low, moderate, high, very high) — and that risk category is what determines your monitoring frequency and treatment intensity.
Number 2: Your rate of eGFR decline per year
A stable eGFR is a good eGFR, even if the number itself is low. The normal age-related drop is roughly 1 mL/min per year. A drop of 3-5 mL/min per year is concerning. A drop above 5 mL/min per year is rapid progression and demands urgent assessment.
This is why I tell patients to keep their own running log of eGFR results. Compare each new result not just to the reference range but to your own previous numbers. A trajectory of 65 → 62 → 58 over three years is a slow drift. The same numbers reached in twelve months — 65 → 62 → 58 — is something completely different and needs nephrology input now.
Tool: Estimate Your BP-Driven Kidney Damage Risk →What Causes CKD in Men: The Top 5 Drivers I See
The causes of CKD have shifted over the last 30 years. In men presenting today, this is the order of frequency I see, and it broadly matches US and international registry data [4].
1. Diabetes (roughly 40% of cases)
Diabetic nephropathy is the leading cause of end-stage kidney disease in the US. Years of high blood glucose damage the small filtering vessels in the kidney (glomeruli). The first warning sign is microalbuminuria — long before eGFR starts dropping. Every diabetic man should have a UACR test annually, no exceptions.
2. Hypertension (roughly 25% of cases)
Untreated or under-treated high blood pressure scars the kidney’s small arteries and reduces filtration over years. The link runs both ways: hypertension causes CKD, and CKD causes hypertension. Tight BP control under 130/80 mmHg is the single most evidence-backed intervention to slow progression in non-diabetic CKD.
3. Kidney stones and obstructive uropathy (roughly 10-15%)
Recurrent stones, prolonged obstruction from an enlarged prostate, or chronic urinary retention all damage the kidney over time. This is the urological piece I see in my own clinic. A man with a single stone and no obstruction is at minimal CKD risk. A man with three stones in five years, particularly with any episode of obstruction or infection, has meaningful CKD risk and needs his eGFR monitored.
4. Glomerulonephritis and inherited disease (roughly 10%)
IgA nephropathy, focal segmental glomerulosclerosis, polycystic kidney disease, and Alport syndrome. These usually present with proteinuria, blood in the urine, or a strong family history. They are nephrologist territory from diagnosis onward.
5. Drug-induced and miscellaneous (roughly 10%)
Long-term NSAID use (ibuprofen, naproxen) is a widely underappreciated cause. Lithium, certain chemotherapy agents, and repeated contrast exposure also contribute. I have seen otherwise healthy men in their 60s with Stage 3a CKD whose only identifiable cause was a decade of daily ibuprofen for joint pain.
→ Related Read: Why creatine raises your creatinine without harming the kidney.If you have recurrent kidney stones or persistent blood in your urine, both deserve a proper workup — not just for stone or bladder reasons, but to identify CKD early.
Slowing CKD Progression: What Actually Works
The good news about CKD is that progression is not a foregone conclusion. Three interventions have strong, high-quality evidence behind them. The other things you read about online — special diets, supplements, herbal remedies — range from “minor effect at best” to “actively harmful.”
Lever 1: Blood pressure under 130/80 mmHg
The SPRINT trial and subsequent KDIGO 2024 guidance both support a systolic target under 130 mmHg in most CKD patients [1]. The preferred first-line agents are ACE inhibitors (e.g. ramipril, lisinopril) or ARBs (e.g. losartan, telmisartan). These medications do more than just lower BP — they reduce protein leakage and slow filtration loss directly. If you have CKD and are not on one of these, that conversation needs to happen at your next visit.
Lever 2: Glycaemic control if diabetic
An HbA1c around 7% (53 mmol/mol) is the typical target for diabetic CKD, though this gets individualized. Aggressive control below 6.5% sometimes does more harm than good in older patients due to hypoglycemia risk. The point is consistency: erratic glucose with frequent highs damages the kidney filters more than a steadily controlled higher target.
Lever 3: SGLT2 inhibitors (the genuine breakthrough of the last decade)
Dapagliflozin and empagliflozin were originally developed as diabetes drugs but have been shown to slow CKD progression by roughly 40% in eligible patients, including non-diabetic CKD [5]. The DAPA-CKD and EMPA-KIDNEY trials are the strongest renal protection evidence we have seen in 20 years. If you have CKD with proteinuria and you are not on one of these, ask your doctor specifically whether you should be.
What else helps (smaller effects, but real)
- Reducing sodium below 2,000 mg per day (about 1 teaspoon of salt) — helps BP control and reduces fluid retention.
- Maintaining adequate hydration — around 2-2.5 liters per day (about 70-85 fl oz) for most men. Not excessive — there is no benefit beyond this and risk of hyponatremia.
- Stopping NSAIDs — ibuprofen, naproxen, diclofenac. Acetaminophen (paracetamol) is safe up to 3 g/day. This single switch is one of the most impactful changes I prescribe.
- Treating proteinuria-driving conditions — gout, hypothyroidism, sleep apnea.
High blood pressure and worried about your kidneys? Download Dr. Khalid’s Blood Pressure & Kidney Protection Guide.
Enter your email below to receive Dr. Khalid’s complete Blood Pressure & Kidney Protection Guide as a free, printable PDF.
When to See a Nephrologist vs. Stay With Your Primary Doctor
Most early CKD is managed perfectly well by primary care. Specialist referral becomes the right call at specific thresholds, and over-referral is its own problem — it congests nephrology clinics and delays the patients who genuinely need a specialist. The KDIGO criteria for referral are clear [1]:
- eGFR below 30 (Stage 4 or 5) — automatic referral.
- UACR above 300 mg/g regardless of eGFR — heavy proteinuria needs specialist input.
- eGFR drop above 5 mL/min in 12 months — rapid progression needs urgent assessment.
- Persistent hematuria with proteinuria — possible glomerulonephritis, needs biopsy consideration.
- Resistant hypertension — BP not controlled on 3 or more medications including a diuretic.
- Suspected hereditary disease — polycystic kidneys, family history of dialysis.
- Recurrent kidney stones with declining eGFR — urology and nephrology often share care here.
Stage 1, 2, and 3a CKD without proteinuria are primary-care conditions in almost every guideline. If you are in those stages and have been told “you have CKD, see a kidney specialist immediately,” that is not wrong, but it is not the only reasonable approach either.
Red Flags: When CKD Needs Urgent Attention
Get Urgent Medical Attention If:
- Your eGFR drops more than 5 points in 12 months (call your doctor within a week — not your next routine visit)
- You develop sudden ankle swelling combined with foamy urine and fatigue (likely nephrotic-range proteinuria)
- You have not urinated in 8+ hours, or your urine output drops markedly
- You develop shortness of breath at rest or while lying flat (possible fluid overload)
- You develop confusion, severe nausea, or persistent vomiting (possible uremia in advanced CKD)
- You experience flank pain with fever in known kidney disease (possible infection requiring same-day assessment)
For any of the above, contact your doctor the same day or attend the emergency room. The kidney injury that starts as a slow decline can accelerate suddenly under the right combination of dehydration, infection, or a wrong medication.
Frequently Asked Questions
What are the 5 chronic kidney disease stages and what does each one mean?
The 5 chronic kidney disease stages are defined by eGFR: Stage 1 (eGFR 90+, with kidney damage), Stage 2 (60-89, with damage), Stage 3a (45-59, mild-moderate loss), Stage 3b (30-44, moderate-severe loss), Stage 4 (15-29, severe loss), and Stage 5 (below 15, kidney failure requiring dialysis or transplant). Stage 3a is the first stage where CKD becomes a formally monitored condition for most patients. You can calculate your eGFR-based CKD stage here.
Can CKD be reversed if caught early?
CKD is generally considered non-reversible — the structural damage to the kidney filters does not regrow. However, the rate of decline can be slowed dramatically, sometimes to near-zero progression, especially in Stages 1-3a. Early diagnosis combined with tight blood pressure control, glycemic management if diabetic, and SGLT2 inhibitor therapy can keep some patients stable for decades. Acute kidney injury, which is different from CKD, often does reverse fully if the cause is treated.
What is a normal eGFR for my age?
Healthy young adults typically have eGFR between 100 and 120. eGFR falls by roughly 1 mL/min per year after age 40 as a normal part of aging. By age 70, an eGFR of 70-80 in someone with no proteinuria and no other kidney disease is age-appropriate, not CKD. The number alone is not enough — your UACR (urine protein) and BP control both shape what the eGFR actually means for you.
Does drinking more water help with CKD?
Adequate hydration of around 2-2.5 liters daily (about 70-85 fl oz) is helpful, but more is not better. Excessive water intake does not “flush” the kidneys or improve function — and in advanced CKD it can cause dangerous fluid overload and low sodium. If you have Stage 3b or worse, your nephrologist will give you a specific fluid target based on your residual urine output and any swelling.
How fast does chronic kidney disease usually progress?
The average rate of eGFR decline in untreated CKD is around 3-4 mL/min per year — meaning a Stage 3a patient (eGFR 50) might reach Stage 4 (eGFR 20) over 8-10 years without treatment. With good control of blood pressure, blood sugar, and proteinuria, this rate can drop to 1 mL/min per year — the same as normal aging. Rapid progression — over 5 mL/min per year — is uncommon and demands urgent nephrology assessment.
Is Stage 3 CKD considered serious?
Stage 3a (eGFR 45-59) is the line where CKD becomes a labeled, monitored condition but is not in itself dangerous in the short term. Most Stage 3a patients remain stable for years and never reach dialysis. Stage 3b (eGFR 30-44) is more serious — symptoms become more likely, nephrology referral becomes routine, and the risk of progression rises. The severity depends heavily on the trajectory and on UACR, not just the eGFR number.
References
- KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International. 2024;105(4S):S117-S314. KDIGO
- Centers for Disease Control and Prevention. Chronic Kidney Disease in the United States, 2023. National Center for Chronic Disease Prevention and Health Promotion. CDC
- Matsushita K, van der Velde M, Astor BC, et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts. The Lancet. 2010;375(9731):2073-2081. PubMed
- United States Renal Data System. 2023 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. National Institute of Diabetes and Digestive and Kidney Diseases. NIDDK
- Heerspink HJL, Stefansson BV, Correa-Rotter R, et al. Dapagliflozin in Patients with Chronic Kidney Disease (DAPA-CKD). New England Journal of Medicine. 2020;383(15):1436-1446. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.