Kidney stone pain vs back pain is one of the most common diagnostic puzzles I see in the emergency room — and getting it wrong costs you. You wake at 3 a.m. with severe pain in your side. It is deep, it is relentless, and lying still makes it worse. Did you pull a muscle, or is a stone moving down your ureter?
Both conditions can cause intense flank and lower back pain, and patients regularly arrive at the hospital convinced they have one when they actually have the other. The distinction matters. A kidney stone causing obstruction can progress to infection and permanent kidney damage within hours. A muscular strain needs rest and an anti-inflammatory.
As a urologist with 11+ years of stone practice, I can usually identify renal colic within the first 30 seconds of watching a patient walk into the cubicle. There are specific patterns — in pain character, location, timing, and associated symptoms — that reliably separate these two conditions. Here is exactly what to look for, and the red flags that mean you go to the emergency room now, not in the morning.
Key Takeaways
- Kidney stone pain is colicky — it comes in waves. Back pain is constant and worsens with movement. This single pattern is the most reliable clinical clue I use in the ER.
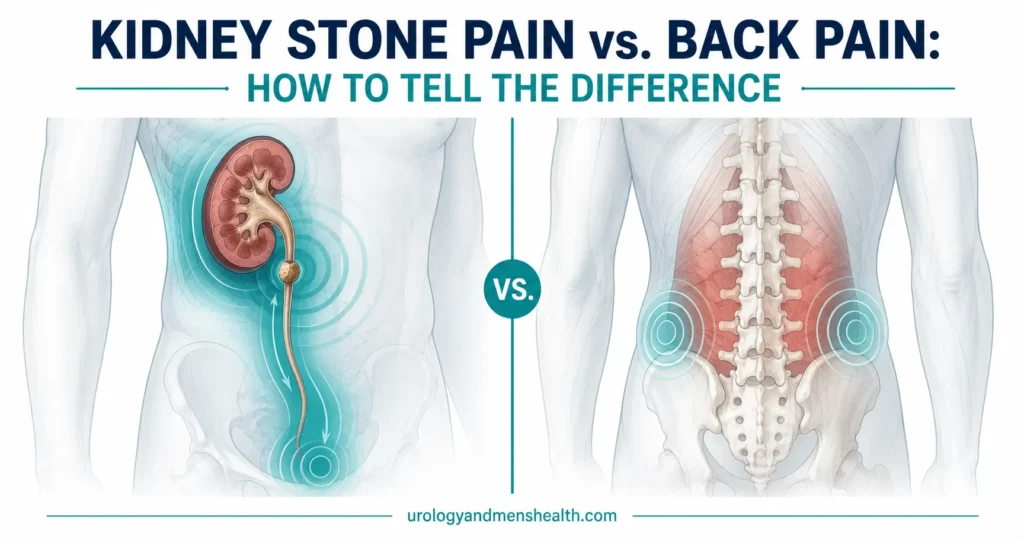
- Renal colic radiates from the flank downward toward the groin or testicle, following the ureter. Mechanical back pain stays in the lumbar area or radiates down the back of the leg — never to the groin.
- Stone patients pace the room. Back-pain patients find one position of relief and stay still. This “writhing sign” has over 85% sensitivity for renal colic.
- Nausea, vomiting, and visible or dipstick-positive blood in the urine occur in roughly 50–85% of stone episodes. They are essentially never caused by a pulled muscle.
- Fever above 38°C (100.4°F) plus flank pain = urological emergency. This may be an infected obstructed kidney and needs same-day drainage with a stent or nephrostomy.
- A non-contrast CT KUB is the gold standard. A plain abdominal X-ray misses up to 50% of stones, particularly small ones and uric acid stones.
In This Guide:
The 6 Key Differences Between Kidney Stone Pain and Back Pain
When I teach junior doctors in the emergency department, I tell them to focus on six specific features that separate renal colic from musculoskeletal back pain. Each feature on its own is suggestive. Three or more together make the diagnosis almost certain before any imaging is done.
1. Pain character: waves vs. constant
This is the single most distinguishing feature. Kidney stone pain is colicky — it builds to an excruciating peak over 20 to 60 minutes, partially eases, and then surges back. These waves correspond to peristaltic contractions of the ureter (the muscular tube draining urine from kidney to bladder) as it tries to squeeze the stone downward. Pain between waves is still present but is noticeably less severe.
Muscular back pain, by contrast, is constant and dull, with a baseline ache that worsens with specific movements — bending, lifting, twisting — but does not fluctuate in the dramatic surge-and-ease pattern of colic. If your pain has a rhythmic wave quality, think stone first.
2. Pain location and radiation
Kidney stone pain typically begins in the flank — the area between the lower ribs and the hip on one side — and radiates downward, following the path of the ureter. Where the stone sits along that path changes where the pain travels to:
- Upper ureter (near the kidney): Pain stays in the flank and may spread to the upper abdomen.
- Mid-ureter: Pain radiates around the side toward the lower abdomen.
- Lower ureter (near the bladder): Pain refers down to the groin, inner thigh, or testicle. Men often describe a deep testicular ache without any testicular pathology — a phenomenon driven by shared genitofemoral nerve roots (L1–L2).
Musculoskeletal back pain centers on the lumbar spine (lower back, midline or slightly off-center) and may radiate into the buttock or down the back of the leg as sciatica. It does not radiate to the groin or testicle. If your pain tracks from your side down toward your groin, that is a ureter, not a muscle.
3. Effect of movement and position
This is the observation I make within seconds of seeing a patient. Kidney stone patients cannot sit still. They pace, they rock, they shift positions constantly, they curl up and then stand back up. No position provides relief. This restlessness is so characteristic that ER physicians call it the “writhing sign” — it has over 85% sensitivity for renal colic [1].
Back pain patients do the opposite. They find one position that reduces the pain — often lying flat or curled on one side — and they stay completely still. Movement makes it worse. If someone is lying motionless on the bed and asks not to be moved, that is almost certainly not a kidney stone.
➡ Related Read: Kidney Stones — Complete Guide from a Urologist
4. Associated symptoms
Kidney stones trigger a cluster of symptoms that mechanical back pain simply does not produce:
- Nausea and vomiting — present in 50–80% of acute renal colic episodes. The kidney and the gut share autonomic nerve pathways through the celiac plexus, so severe colic frequently triggers profuse vomiting before the pain is even fully established.
- Hematuria (blood in the urine) — visible or microscopic blood is present in approximately 85% of stone patients [2]. Even if your urine looks normal, a 60-second dipstick in the ER will usually show red blood cells.
- Urinary urgency and frequency — particularly when the stone reaches the lower ureter near the bladder. Patients describe a constant, intense need to urinate despite an empty bladder.
Mechanical back pain does not cause nausea, blood in the urine, or urinary symptoms. If you have severe flank pain combined with vomiting and pink, red, or brown urine, you can be reasonably confident you are dealing with a stone, not a strain.
5. Onset and trigger
Renal colic has a sudden, spontaneous onset — often waking patients from sleep between 2 a.m. and 6 a.m. when urine is most concentrated and a stone is more likely to shift into the ureter. There is typically no precipitating activity. You did not lift anything heavy. You did not twist the wrong way. The pain simply arrived.
Back pain almost always has an identifiable trigger or a gradual buildup: a heavy lift, a long drive, prolonged sitting at a desk, a specific gym movement, or a progressive worsening over days. If your severe flank pain appeared out of nowhere at 2 a.m. with no mechanical trigger, that pattern fits a stone far better than a strain.
6. Response to painkillers
Renal colic responds well to specific medications. NSAIDs (ketorolac, diclofenac) are first-line treatment and are more effective than opioids for acute stone pain across multiple randomized trials [3]. A single intramuscular dose of ketorolac 30 mg or diclofenac 75 mg typically delivers meaningful relief within 20 to 30 minutes. Acetaminophen (paracetamol) alone is rarely adequate for acute colic.
Muscular back pain responds to a combination of acetaminophen, NSAIDs, a muscle relaxant, and — most importantly — specific positioning and gradual mobilization. Heat therapy helps a muscle strain but has no effect on renal colic.
➡ Related Read: How to Pass a Kidney Stone Fast — What I Tell My Patients
The Quick Comparison Table
| Feature | Kidney Stone (Renal Colic) | Musculoskeletal Back Pain |
|---|---|---|
| Pain pattern | Colicky — comes in waves | Constant, dull ache |
| Location | Flank → groin / testicle | Lumbar midline → buttock / back of leg |
| Movement | Restless, cannot get comfortable | Lies still; movement worsens pain |
| Nausea / vomiting | Common (50–80%) | Rare |
| Blood in urine | Present in ~85% | Absent |
| Onset | Sudden, often nocturnal, no trigger | Gradual or linked to specific activity |
| Best initial painkiller | IM ketorolac / IM diclofenac | Acetaminophen + NSAID + muscle relaxant |
If you scored a stone-like pattern on at least three of these features, you should be checking your urine and heading toward medical assessment, not waiting it out. You can also estimate the likelihood your stone will pass on its own using our kidney stone passage calculator once size is confirmed on imaging.
The Dangerous Overlap: When You Have Both
Here is a clinical reality that textbooks gloss over: some patients genuinely have both. Chronic lumbar disc disease is common in men over 40 — the same population most likely to form kidney stones. I regularly see patients with a known back pain history who dismiss new flank pain as “just my back acting up again.” That assumption can be dangerous.
If you have a history of back pain but notice any of the following new features, do not assume it is your back:
- Pain that is unilateral (one-sided only) rather than central or bilateral.
- Pain that radiates toward the groin rather than down the back of the leg.
- New nausea or vomiting alongside the pain.
- Any visible change in urine color (pink, red, or dark brown).
- Pain that wakes you from sleep and makes you unable to lie still.
Any of these warrants an ER visit for a urine dipstick at minimum, and ideally a CT KUB to rule out an obstructing stone. The reverse trap also exists: a small, asymptomatic stone showing up on imaging done for back pain is often blamed for symptoms it is not causing. The decision-maker is whether the clinical picture matches the imaging finding, not the imaging finding alone.
How the Diagnosis Is Confirmed
CT KUB — the gold standard
A non-contrast CT scan of the kidneys, ureters, and bladder (CT KUB) is the definitive diagnostic study for kidney stones. The American Urological Association lists low-dose non-contrast CT as the recommended imaging for acute flank pain suspected of stone disease, with sensitivity of 95–98% and specificity of 96–100% for stones of any size and composition [4]. The scan takes under 5 minutes, requires no contrast dye, and reveals the stone’s size, exact location, and whether the ureter is obstructed — all of which directly drive treatment.
A plain abdominal X-ray (KUB film) misses roughly half of all stones, particularly uric acid stones (which are radiolucent) and small stones overlying bone. Ultrasound is a reasonable first-line study in pregnancy and in younger patients to avoid radiation exposure, but its sensitivity for ureteric stones is only around 45% [5]. If you are in the ER with suspected renal colic and they are only doing a plain X-ray, it is reasonable to ask about CT.
Urine dipstick
A bedside urine dipstick is quick, cheap, and informative. The presence of blood (hematuria) supports a stone diagnosis, though its absence does not rule one out — approximately 10–15% of confirmed stone episodes have a negative dipstick. The dipstick also screens for infection markers (leukocytes, nitrites), which is critical because an infected, obstructed kidney is a surgical emergency, not a problem antibiotics alone can fix.
➡ Related Read: Kidney Stone Size Chart — When You Can Wait and When You Need Surgery
Other Conditions That Mimic Kidney Stone Pain
Renal colic and back pain are not the only two possibilities. Several other conditions can present with similar flank or abdominal pain, and a good clinician keeps these on the differential:
- Pyelonephritis (kidney infection) — flank pain with fever, rigors, and painful urination. Distinguished from a clean stone episode by the high fever and systemic illness, though a stone can cause pyelonephritis when it obstructs the ureter.
- Abdominal aortic aneurysm (AAA) — in men over 60 with sudden severe flank or back pain, this has to be excluded urgently. A ruptured AAA is fatal without emergency vascular surgery. CT scan settles it in minutes.
- Appendicitis — right-sided lower abdominal pain can mimic a right lower ureteric stone. Distinguished by McBurney’s point tenderness, fever, and elevated white cell count.
- Testicular torsion — sudden testicular pain in younger men can be confused with lower ureteric stone pain radiating to the groin. Torsion is a surgical emergency that needs intervention within 6 hours.
- Renovascular hypertension — in patients with poorly controlled blood pressure, flank pain combined with worsening kidney numbers should make a clinician consider renal artery problems. If you have a history of uncontrolled high blood pressure damaging your kidneys, the threshold for full imaging is lower.
- Musculoskeletal rib pain — pain from a lower rib fracture or intercostal neuralgia can overlap with upper ureteric stone pain. Distinguished by tenderness on pressing directly over the affected rib.
What to Do Right Now If You Are Not Sure
If you are reading this at 3 a.m. trying to work out whether your pain is a stone or your back, here is the practical decision framework I give patients:
- Check your urine. If it is pink, red, or brown — go to the ER. Visible blood in urine with flank pain is a stone until proven otherwise.
- Assess your movement pattern. If you are pacing and shifting positions, unable to get comfortable, that is colic behavior. If you found a comfortable position and moving makes it worse, it is more likely musculoskeletal.
- Check for nausea. If you are vomiting alongside the pain, especially without any gut symptoms beforehand, that strongly favors a stone.
- Take an NSAID if safe for you. Ibuprofen 400 mg or naproxen 500 mg orally with food. If the pain responds meaningfully within 30 to 45 minutes, that is consistent with renal colic (though not diagnostic). Skip NSAIDs if you have stage 3+ chronic kidney disease, a peptic ulcer, or you are on blood thinners — go straight to the ER instead.
- Go to the ER if you have a fever above 38°C (100.4°F) with the pain (possible infected, obstructed stone — emergency), you have only one functioning kidney, you cannot keep fluids down because of vomiting, or the pain is uncontrollable despite maximum oral analgesia.
In My Practice
The pattern I see most often is a man in his late 30s or 40s who arrives at the ER convinced he pulled something at the gym two days ago. He hands the triage nurse a story about deadlifts and is mildly annoyed at being asked for a urine sample. The dipstick comes back 3+ for blood. The CT shows a 6 mm stone wedged at the ureterovesical junction. He has not lifted anything heavy in his life that the kidney cared about — the stone formed silently over months and chose that night to move.
The reverse trap is just as common, and arguably more dangerous: a 50-something man with a long history of disc disease who dismisses new right-sided flank pain because “it’s the back again.” When the picture finally points to a stone, the kidney has been quietly under pressure for days. If you have a known back history and the pain feels different — one-sided, radiating to the groin, with any nausea — treat it as a new problem until proven otherwise.
When to See a Doctor — Urgently
- Fever above 38°C (100.4°F) with flank pain — suggests an infected, obstructed kidney (obstructive pyelonephritis). This is a urological emergency that needs same-day ureteric stent insertion or percutaneous nephrostomy drainage. Antibiotics alone will not solve an obstructed system.
- Complete inability to pass urine (anuria) — suggests bilateral obstruction or obstruction of a single functioning kidney. Needs emergency decompression.
- Uncontrollable vomiting with inability to stay hydrated — dehydration worsens stone impaction and kidney function. You need IV fluids and parenteral analgesia.
- Pain unresponsive to maximum oral analgesia — if 400 mg ibuprofen plus 1 g acetaminophen together are not controlling the pain, you need ER assessment and IV or IM analgesia.
- Known single kidney or chronic kidney disease — any flank pain in someone with a solitary functioning kidney warrants urgent imaging to rule out obstruction. There is no backup kidney to maintain function.
Think Your Flank Pain Might Be a Stone? Get the Full Prevention Protocol
Enter your email below to receive Dr. Khalid’s complete 7-Day Kidney Stone Prevention Meal Plan as a free, printable PDF — the same protocol I give every patient leaving the ER after a stone episode.
Frequently Asked Questions
Can kidney stone pain feel exactly like back pain?
In some cases, particularly with stones lodged high in the renal pelvis or upper ureter, the pain can feel similar to lumbar back pain. The differentiators are: kidney stone pain is typically unilateral and colicky (comes in waves), while back pain is usually constant and worsens with movement. Nausea, vomiting, or blood in the urine tips the diagnosis strongly toward a stone. If you are genuinely uncertain, a urine dipstick and CT KUB will settle it within minutes — see our full guide to kidney stone symptoms and treatment for what to expect.
Can a kidney stone cause flank pain that lasts for weeks?
Yes, but with an important distinction. Acute renal colic — the severe, wave-like pain — typically lasts hours to a few days per episode. A stone that is partially obstructing the ureter, though, can cause a persistent dull ache in the flank that lasts weeks. This chronic discomfort is often milder than the initial colic but is a sign that the stone has not passed. Persistent pain beyond 4 weeks warrants repeat imaging and usually surgical intervention — review the size thresholds for waiting vs. treating before deciding.
Why does kidney stone pain sometimes radiate to the testicle?
The testicle and the kidney share the same embryological nerve supply — the genitofemoral nerve (L1–L2). When a stone irritates the lower ureter, the brain interprets the pain signal as originating from the testicle or groin. This is called referred pain — the same mechanism by which a heart attack causes jaw pain. A stone causing testicular pain does not mean there is anything wrong with the testicle itself, but if testicular pain is sudden and isolated with no flank component, see our guide on passing stones and rule out torsion separately.
Should I go to the ER for flank pain if I have had kidney stones before?
If you recognize the pain as identical to your previous stone episodes and you can manage it with oral analgesia at home, you may not need an immediate ER visit. You should go to the ER, though, if you develop a fever, you cannot keep fluids or painkillers down because of vomiting, the pain is worse than previous episodes, or you have only one functioning kidney. Even if you manage it at home, see your primary care doctor or urologist within 48 hours for a urine test and imaging to confirm stone location and size — guidance covered in how to pass a kidney stone fast.
Can mechanical back pain cause blood in the urine?
No. Pure musculoskeletal back pain — disc disease, muscle strain, facet joint arthritis — does not cause hematuria. If you have back or flank pain combined with visible or dipstick-positive blood in your urine, there is a urological cause until proven otherwise. The most common cause is a kidney stone, but bladder or kidney tumors and pyelonephritis are also on the list. Blood in the urine always warrants investigation regardless of any co-existing back symptoms — start with the full kidney stone workup if a stone is suspected.
I have chronic disc disease. How do I tell a new stone from a flare?
Three features reliably separate a new stone from a disc flare in someone with known back disease. First, location: a stone is one-sided in the flank radiating to the groin; a disc flare is usually central or radiates down the leg. Second, behavior: a stone makes you pace; a disc flare keeps you in one position. Third, urine: a dipstick showing blood, or any visible color change, points strongly to a stone. If any one of these three is new for you, treat it as a stone episode until imaging proves otherwise — and start with our stone passage calculator once size is confirmed.
References
- Eskelinen M, Ikonen J, Lipponen P. Usefulness of history-taking, physical examination, and diagnostic scoring in acute renal colic. European Urology. 1998;34(6):467–473. PubMed
- Luchs JS, Katz DS, Lane MJ, et al. Utility of hematuria testing in patients with suspected renal colic: correlation with unenhanced helical CT results. Urology. 2002;59(6):839–842. PubMed
- Pathan SA, Mitra B, Cameron PA. A systematic review and meta-analysis comparing the efficacy of nonsteroidal anti-inflammatory drugs, opioids, and paracetamol in the treatment of acute renal colic. European Urology. 2018;73(4):583–595. PubMed
- Assimos D, Krambeck A, Miller NL, et al. Surgical Management of Stones: AUA/Endourological Society Guideline. Journal of Urology. 2016;196(4):1153–1160 (amended 2023). AUA
- Smith-Bindman R, Aubin C, Bailitz J, et al. Ultrasonography versus computed tomography for suspected nephrolithiasis. New England Journal of Medicine. 2014;371(12):1100–1110. PubMed
- EAU Guidelines on Urolithiasis. European Association of Urology, 2024 edition. EAU

Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.