Catheter Care at Home: How to Avoid Infections
Done right, catheter care at home prevents most infections. The ones I treat usually trace to a few avoidable habits — bag height, hand hygiene, and opening the closed system too often. Here's what protects you.


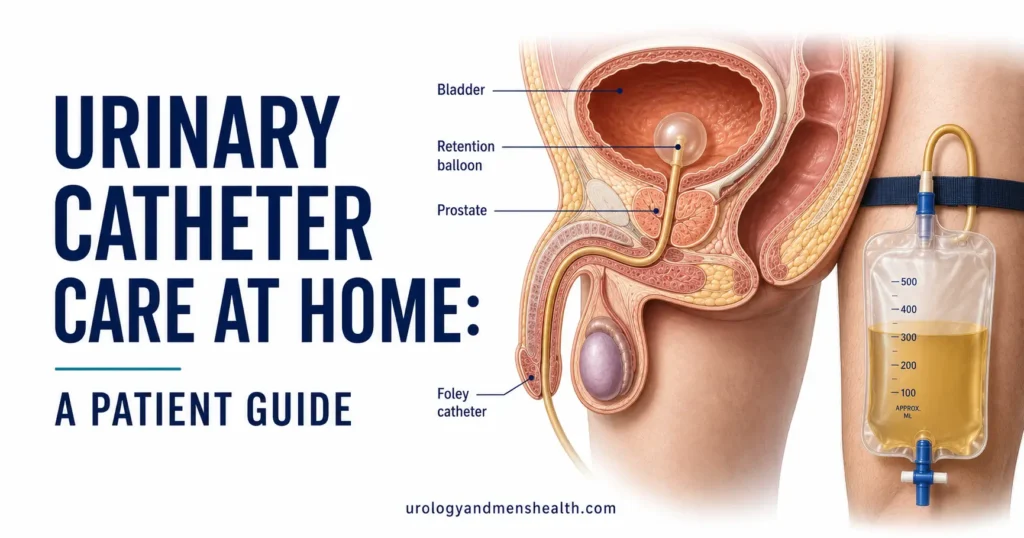
Catheter care at home comes down to one idea: a catheter is an open road from the outside world straight into your bladder, and your job is to stop bacteria from driving up it. Most of the catheter infections I see in clinic aren’t bad luck — they trace back to a few specific habits: a drainage bag lifted above the bladder, a closed system opened more often than it needs to be, hands that skipped a wash. Get those right and your risk drops sharply. A urinary catheter — the flexible tube, often called a Foley, that drains urine when you can’t empty your bladder on your own — protects you from retention, but it also bypasses every natural defense your urethra normally provides. This guide covers the daily routine, the drainage-bag rules that matter most, the habits that quietly invite infection, and the red flags that mean you call your doctor today. For the wider picture on urinary infections, see our complete UTIs & Infections Hub.
Key Takeaways
- Keeping the drainage bag below your bladder at all times is the single highest-impact habit — urine that flows backward carries bacteria with it.
- Wash your hands before and after touching the catheter or bag, and clean the catheter and surrounding skin once daily with plain soap and water — no powders, creams, or antiseptics.
- Cloudy or strong-smelling urine on its own is not a reason for antibiotics; fever, chills, flank pain, or new confusion are.
- Long-term catheters grow bacteria in the urine within weeks in almost everyone — treatment is for symptoms, not for a positive culture.
How Catheter Infections Actually Start
A healthy urethra is a hostile place for bacteria — it’s narrow, it flushes itself every time you urinate, and its lining fights colonization. A catheter undoes all three. It props the channel open, gives bacteria a surface to cling to, and lets urine sit in tubing instead of being flushed out. The result is a catheter-associated urinary tract infection (CAUTI) — a urinary infection that develops while a catheter is in place or within 48 hours of removing it.
Bacteria reach the bladder by two routes. They creep up the outside of the catheter along the thin film of mucus where it meets your skin, or they travel up the inside of the tube from the drainage bag whenever the system is opened or urine flows backward. Within days, a slimy layer called biofilm coats the catheter surface and shields the bacteria from both your immune system and antibiotics [1]. This is why prevention is mostly mechanical — you’re managing surfaces and flow, not fighting an infection that has already taken hold.
Most men I catheterize have been through acute urinary retention — a sudden, painful inability to empty the bladder. If that’s what led to yours, our emergency guide to acute urinary retention explains what comes next. Catheters also differ in ways that affect risk: urethral (through the penis) versus suprapubic (through a small opening in the lower abdomen), and a range of sizes and materials that change comfort and how readily biofilm builds. If you’re unsure what you have, our catheter size and type selector walks through the differences.
Daily Catheter Care at Home: Your Cleaning Routine
Good indwelling catheter care is a short routine done consistently, not a complicated one. Start and finish every catheter task by washing your hands — soap and water if they look dirty, otherwise an alcohol-based sanitizer is fine [3]. Once a day, ideally in the shower, clean the catheter and the skin around where it enters your body using plain soap and warm water.
- Hold the catheter gently and wash away from your body — start where it exits and move outward down the tube, never back toward the opening.
- Rinse well and pat dry with a clean towel. Moisture left behind feeds bacteria.
- Do not apply powder, lotion, antiseptic, or antibiotic cream to the area — they irritate skin and offer no infection benefit.
- Secure the catheter to your thigh with a leg strap or anchoring device so it can’t tug at the bladder neck. Repeated micro-tugging causes tiny injuries that bacteria exploit.
That’s the whole daily routine for infection prevention. For the step-by-step mechanics beyond hygiene — changing bags, troubleshooting leaks, what to keep on hand — our full home catheter patient guide covers the practical side in detail.
In My Practice
One of my long-term catheter patients came back with his third infection in four months, and on paper he was doing everything right. When I walked through his evening, the problem appeared: he hung the night bag over the footboard, but his recliner sat higher than the tubing, so for three hours each evening urine pooled in a loop level with his bladder. We changed nothing except where the bag hung. He went the next eight months without a single infection.
Recurrent catheter infections are far more often a mechanics problem — bag height, a kinked loop, an opened system — than a hygiene-effort problem.
Drainage Bag Rules That Prevent Infection
If you remember only one rule from this article, make it this one: keep the drainage bag below the level of your bladder at all times — sitting, standing, walking, and lying down [1]. Gravity has to pull urine away from you. The moment the bag rises to or above your bladder, urine that has been sitting in the tube — already carrying bacteria — drains backward into you.
- Never rest the bag on the floor. Hang a night bag on the bed frame; strap a leg bag below the knee or mid-thigh.
- Keep the tube free of kinks and dependent loops. A loop of tubing hanging below the bag traps urine and stalls flow.
- Empty the bag when it is half to two-thirds full, and at least every 4 to 8 hours — a full bag back-pressures urine toward the bladder.
- Wash your hands before and after emptying, and don’t let the outlet spout touch the toilet, container, or floor.
Above all, keep the system closed. Every time you disconnect the catheter from the bag, you hand bacteria a direct path inside. Major prevention guidance is built around maintaining an unbroken, sealed drainage system and opening it as rarely as possible [1].
Caring for a catheter and worried about infections?
Enter your email below to receive Dr. Khalid’s complete Recurrent UTI Eradication Protocol as a free, printable PDF.
Habits That Quietly Raise Your Infection Risk
Preventing catheter infections is as much about what you stop doing as what you start. Several common, well-meaning habits make things worse:
- Routine “just in case” antibiotics. Both CDC and IDSA guidance specifically advise against preventive antibiotics for catheter users — they don’t reliably stop infection, and they push your own bacteria toward resistance [2].
- Antiseptic in the bag, bladder washes, and cranberry. Putting antiseptic solution in the drainage bag and routine bladder irrigation are not recommended, and cranberry products have not been shown to prevent catheter infections [1].
- Fixed-calendar changes. Swapping the catheter or bag on an automatic weekly schedule is discouraged; each change briefly breaks the closed system. Change for a reason — blockage, infection, or leakage.
- Under-drinking. Unless your doctor has restricted fluids, aim for roughly 2 to 2.5 liters of water a day (about 68 to 85 fl oz, or 8 to 10 cups) to keep urine flowing and the tube flushed.
The strongest long-term move is reducing exposure altogether. Ask your urologist whether intermittent (in-and-out) catheterization is an option for you, and how long your current catheter can safely stay in — the fewer days it’s in place, the lower your cumulative risk.
When to Call Your Doctor or Go to the ER
A blocked catheter is an emergency, not an inconvenience. If no urine has drained for two hours and your bladder feels full or painful, do not wait for office hours — go to the emergency room, because backed-up urine can rapidly pressure your kidneys. Treat the warning signs below as prompts to act the same day, not to “see if it settles.”
When to Get Urgent Help
Contact your urology team or go to the ER right away if you notice:
- No urine in the bag for 2 hours while your bladder feels full or painful — the catheter is likely blocked.
- Fever, chills, or shaking — signs the infection may have reached your bloodstream.
- Pain in your side or lower back (flank pain) along with feeling unwell.
- Visible blood or clots, especially if they block the flow of urine.
- New confusion or agitation, particularly in older adults — often the first sign of infection before any fever.
- Leaking around the catheter with pain, or the catheter falling out entirely.
Catheter Care at Home: Common Questions
Does cloudy or smelly urine from my catheter always mean an infection?
No. Almost everyone with a long-term catheter grows bacteria in the urine within a few weeks, which often makes it cloudy or strong-smelling without causing harm. Antibiotics are reserved for symptoms — fever, chills, flank pain, or new confusion. If you’re unsure how to tell ordinary catheter cloudiness from a true infection, our guide on UTIs in men breaks down the warning signs.
How far below my bladder does the drainage bag need to be?
Below the level of your bladder at all times — sitting, standing, walking, and lying down. The exact distance matters less than the direction: gravity has to pull urine away from you, never back toward the bladder. Hang a night bag on the bed frame, not the floor, and keep a leg bag strapped below the knee or mid-thigh, with no looping tube hanging lower than the bag.
I keep getting catheter infections. What lowers my risk the most?
After bag position and hand hygiene, the biggest lever is reducing how often the closed system is opened and how long the catheter stays in — every disconnection and every extra week raises risk. Ask your urologist whether intermittent catheterization is an option for you. You can also gauge your own profile with our UTI risk assessment for men.
Should I take a daily antibiotic to prevent catheter infections?
No — major guidelines specifically advise against routine preventive antibiotics for catheter users. They don’t reliably prevent infection, they push your bacteria toward resistance, and they carry side effects of their own. The same applies to cranberry products, antiseptic bladder washes, and putting antiseptic in the drainage bag: none are recommended for routine prevention.
How often should I change my catheter or drainage bag at home?
Good catheter care at home isn’t about changing on a fixed calendar. Current guidance is to change the catheter and bag for clinical reasons — blockage, infection, leakage, or a damaged system — rather than at automatic weekly intervals, because each change briefly breaks the closed system and lets bacteria in. Your urology team will set a review schedule and tell you the longest safe interval for your catheter.
References
- Healthcare Infection Control Practices Advisory Committee (HICPAC). Guideline for Prevention of Catheter-Associated Urinary Tract Infections. Centers for Disease Control and Prevention. 2009 (updated 2017). CDC
- Hooton TM, Bradley SF, Cardenas DD, et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin Infect Dis. 2010;50(5):625-663. IDSA
- University of Iowa Health Care. Urethral (indwelling) catheter care. UI Health Care Patient Education. 2024. UI Health Care
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.