RIRS vs URS vs PCNL: Which Stone Surgery Fits You?
When a patient asks me "RIRS vs PCNL — which one do I need?" the honest answer almost always comes down to stone size, stone location, and one CT scan. Here is the framework I use in clinic, with the numbers behind every recommendation.

When a patient sits down across from me and asks “RIRS vs PCNL — which one do I need?”, my honest answer is that the choice is almost never about which surgery sounds better. It is about your stone. How big it is on CT. Where it sits inside the kidney. Whether you have one functioning kidney or two. Whether you are on blood thinners. The AUA’s 2026 surgical stone management guideline gives us a clean framework, and I use it daily in clinic.[1] This article walks through that framework — RIRS, URS, and PCNL side-by-side — so you walk into your consultation already understanding why your urologist is recommending what they are. For the full overview of stone surgery options, see our complete Urological Surgery & Recovery hub.
Key Takeaways
- For a kidney stone under 20 mm (about 4/5 inch), RIRS is usually the right answer — no incision, day surgery, 70–85% stone-free at one procedure.
- For a stone over 20 mm or a staghorn stone, PCNL is AUA-recommended first-line. Stone-free rates of 85–95% beat what flexible scopes can achieve at that size.
- For a ureteric stone, semi-rigid URS is faster and cheaper than RIRS — flexible scopes are wasted on stones that a straight scope can reach.
- Lower pole stones between 10 and 20 mm are the genuine grey zone: mini-PCNL gives a higher stone-free rate than RIRS in this size band, per AUA Grade B evidence.
What RIRS Actually Is (And Why The Name Confuses Patients)
RIRS stands for Retrograde IntraRenal Surgery. The name is technical and unhelpful — let me unpack it. “Retrograde” means we go in against the natural flow of urine: up through the urethra, into the bladder, up the ureter, and into the kidney itself. “Intrarenal” means we operate inside the kidney. “Surgery” is misleading because there is no incision anywhere on your body.
The instrument we use is called a flexible ureteroscope. Picture a thin, steerable tube about the diameter of an uncooked spaghetti strand (roughly 3 mm / 9.9 Fr), with a tiny camera at the tip and channels for irrigation and a laser fibre.[2] The tip deflects up to 270 degrees in some models, which is what lets us reach the lower pole of the kidney — a tucked-away anatomical corner where stones love to hide and rigid scopes cannot go.
Once the scope is inside the kidney and we can see the stone on the monitor, we pass a laser fibre through the working channel. Modern stone lasers are either Holmium:YAG or the newer thulium fibre laser, which produces less retropulsion (stones bouncing away from the laser) and finer dust.[3] The stone is broken into either small fragments we extract with a basket, or dust that washes out with urine over the following days.
The whole thing takes 30 to 90 minutes depending on stone size and complexity, you go home the same day, and you have nothing more to show for it than a small ureteric stent and some discomfort. The term “minimally invasive” gets used loosely in medicine — for RIRS it is genuinely accurate.
In My Practice
One of the questions I get most often, especially from patients who have already had a stone before, is “Why do I need a stent again? Last time was awful.” I understand — stent discomfort is the part of stone surgery that nobody warns you about properly. The reason RIRS almost always needs a stent is that the scope passing up and down the ureter causes oedema (swelling), and a swollen ureter can block urine drainage from a kidney that is already irritated. The stent keeps urine flowing while the ureter heals over the next 1–2 weeks.
If your urologist offers RIRS without a stent and your stone was small and uncomplicated, that is a reasonable conversation to have — but expect a stent most of the time, and plan around it.
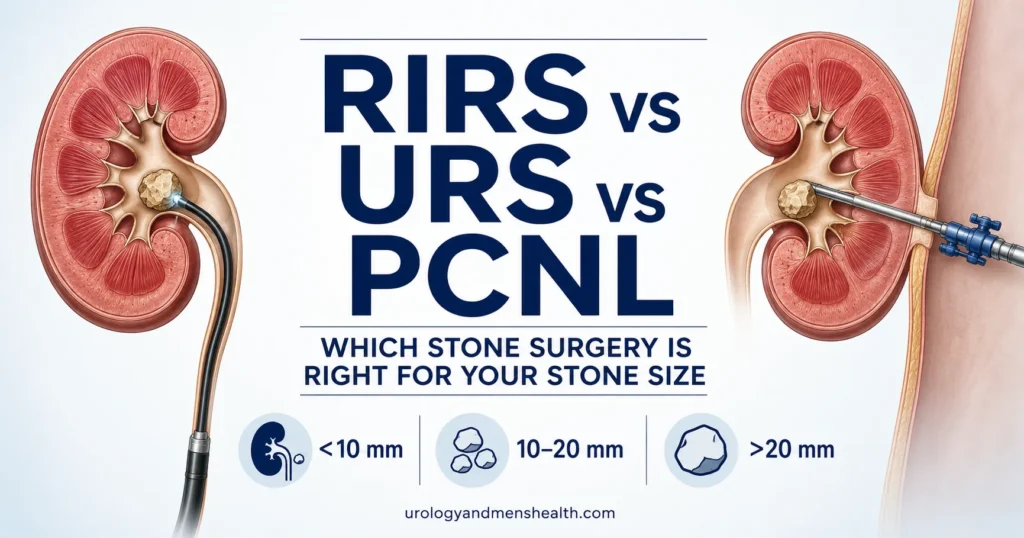
The Stone Size Decision: AUA 2026 Framework
The single most useful number on your CT scan report is the maximum stone diameter in millimetres. Almost every surgical decision flows from that one measurement, modified by location (kidney vs ureter, upper pole vs lower pole) and a few patient factors. Here is the framework from the AUA’s 2026 Surgical Management of Kidney and Ureteral Stones guideline, simplified into the way I explain it in clinic.[1]
Under 10 mm in the ureter
If the stone is sitting in the ureter and it is 10 mm or smaller (about 2/5 inch), surgery is often not the first conversation. The AUA recommends 30 days of medical expulsive therapy with an alpha-blocker like tamsulosin to help the stone pass on its own.[1] Roughly two-thirds of stones in this size band pass without intervention. You can estimate your specific odds with our Kidney Stone Passage Calculator, which uses size and ureteric location to give a passage probability.
If the stone does not move after a fair trial, or you cannot tolerate the pain, or you have signs of infection or kidney damage, the surgery of choice is semi-rigid URS — not RIRS. Ureteric stones do not need a flexible scope; a straight one reaches them faster and cheaper.
Under 20 mm in the kidney
This is the size band where RIRS shines. For kidney stones between roughly 5 mm and 20 mm (about 1/5 to 4/5 inch), RIRS gives stone-free rates of 70–85% at a single procedure, depending on stone location.[4] Upper pole and middle calyx stones do best; lower pole stones a bit less well because gravity works against you when you are trying to flush dust upward and out.
The alternative in this size band is shockwave lithotripsy (SWL) — non-invasive but with lower stone-free rates and a higher chance of needing a second procedure. I tend to favour RIRS for stones that are dense (over 1000 Hounsfield Units on CT), in the lower pole, or in patients who want one definitive procedure rather than a possible series of SWL sessions.
10–20 mm lower pole — the grey zone
The AUA 2026 guideline made a specific recommendation here that surprised some urologists: for kidney stones in the 10–20 mm range, the panel says clinicians may offer mini-PCNL over URS because of higher stone-free rates (Moderate Recommendation, Grade B evidence).[1] Mini-PCNL uses a smaller-diameter access tract than standard PCNL — typically 14–22 Fr versus 24–30 Fr — which reduces the bleeding risk that historically pushed urologists toward RIRS in this band.
What does that mean for you? If your stone is 14 mm in the lower pole of your kidney, ask your urologist whether mini-PCNL is offered at your centre, what their stone-free rate is for that size band, and what the trade-off is in hospital stay (typically 1–2 nights for mini-PCNL versus same-day for RIRS).
Over 20 mm or staghorn
Stones larger than 20 mm (about 4/5 inch) are PCNL territory. The AUA is unambiguous: for adult patients with stones over 2 cm, clinicians should recommend PCNL as first-line therapy.[1] The stone-free rate at one procedure is 85–95% for PCNL versus roughly 50–60% for RIRS at this size. Doing RIRS on a 25 mm stone usually means committing the patient to staged procedures, repeat anaesthesia, and weeks of stent discomfort. PCNL gets it done in one trip to theatre.
For a complete stone-size-to-treatment map, see our anchor article Kidney Stone Size Chart: When to Wait vs Surgery, which covers everything from sub-5 mm passage to staghorn cases.
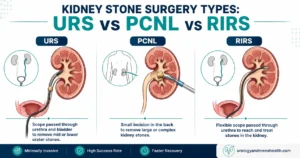
RIRS vs URS: Why Flexible Beats Rigid for Kidneys, Not Ureters
Patients sometimes assume RIRS and URS are different operations with completely different recoveries. They are not — they are the same family of procedures with different scopes, picked for different anatomical targets.
URS (semi-rigid ureteroscopy) uses a straight, slightly bendable scope — about 7–8 Fr — that reaches the lower and middle ureter reliably and the proximal ureter sometimes. Procedure time is short, equipment cost is lower, and the rigid optics are excellent for ureteric stones. The downside is reach: a rigid scope cannot navigate the bend where the ureter enters the kidney, and it cannot deflect into the calyces (the cup-shaped chambers inside the kidney).
RIRS (flexible ureteroscopy) uses a deflectable scope that can angle into any calyx inside the kidney. It is the right choice when the stone is sitting in the renal pelvis or any of the calyces. Single-use disposable flexible scopes are now widely used because they avoid the cross-contamination risk of reprocessed reusable scopes and give consistent image quality.[5]
The simple rule I use: ureteric stone → URS. Kidney stone → RIRS. Some cases need both — a stone in the proximal ureter might require URS to reach the location and then flexible work upstream to retrieve a fragment that has migrated up into the kidney. Your urologist will plan that in advance based on your CT.
RIRS vs PCNL: The Real Trade-Offs
This is the comparison patients want to understand most, and the one with the most variation in how it gets explained. Here is the honest version.
How the kidney is accessed. RIRS goes through the urethra — no incision, no scar. PCNL goes through a 1 cm puncture in your flank (the side of your back, below the rib), through which we pass a larger-bore tube directly into the kidney. The PCNL access tract is bigger, which is why we can break and extract much larger stones.
Stone-free rate at one procedure. For stones under 2 cm, RIRS achieves 70–85% stone-free at one sitting. For stones over 2 cm, PCNL achieves 85–95%.[6] A 2023 Cochrane Review comparing SWL with PCNL or RIRS for kidney stones confirmed that PCNL has the highest stone-free rates overall but the highest complication rate; RIRS sits in the middle on both axes.[7]
Hospital stay. RIRS is day surgery in most centres. PCNL requires 2–4 nights, sometimes with a nephrostomy tube (a temporary external drain from the kidney).
Bleeding risk. This is where PCNL has its biggest weakness. Transfusion rates run around 1–2% for standard PCNL; mini-PCNL drops this further but does not eliminate it.[1] RIRS bleeding risk is minimal — usually just transient pink urine. For patients on lifelong anticoagulation (warfarin, DOACs) or with bleeding disorders, RIRS is far safer.
The “one kidney” question. When a patient has only one functioning kidney — either congenitally or after a previous nephrectomy — I almost always favour RIRS where the stone size allows. The risk of bleeding or pyonephrosis (infected, blocked kidney) from PCNL in a solitary kidney is too high to accept lightly.
For a side-by-side comparison of all the available stone surgeries — URS, RIRS, mini-PCNL, standard PCNL, and SWL — use our Urology Surgery Comparison Tool, which weighs stone size, location, and patient factors to suggest which option fits your case.
Preparing for urological surgery? Download Dr. Khalid’s Urology Surgery Recovery Guide.
Enter your email below to receive Dr. Khalid’s complete Urology Surgery Recovery Guide as a free, printable PDF.
What Recovery Actually Looks Like
The recovery I describe below is for RIRS specifically — PCNL recovery is longer and more involved, which is one of the trade-offs in the size-based decision above.
The day of surgery. You go home the same day in most centres, usually within 4–6 hours of waking up from anaesthesia. Your urine will look pink or rosé — that is normal and means the ureter and kidney are mildly inflamed from the procedure. Bright red urine, clots, or inability to pass urine at all are not normal — those are red flags I cover in the next section.
Days 1–3. Most patients have burning on urination and a tugging or twingeing sensation in the flank when they pass urine. Both are caused by the stent — every time you urinate, urine refluxes briefly up the stent back toward the kidney, and the kidney complains. Painkillers and an alpha-blocker (tamsulosin) help. Drink 2.5–3 litres of water a day (around 85–100 fl oz / 10–12 cups) to flush stone dust through the system.
Days 4–7. Most desk-job patients return to work between days 4 and 7. Avoid heavy lifting, gym work, or anything that significantly increases intra-abdominal pressure.
Week 2. Stent removal in clinic. This takes about 5 minutes, is uncomfortable for a few seconds, and patients almost universally describe immediate relief once it is out. The dragging sensation in the flank usually disappears within hours. If the stent has a string, your urologist may have arranged for self-removal at home; the technique is straightforward but the moment itself is brief and surprising.
Week 4. A follow-up imaging study (low-dose CT or KUB X-ray) to confirm you are stone-free. Roughly 15–30% of patients will have residual fragments under 4 mm on this scan — these usually pass on their own with continued hydration, but you and your urologist may decide to track them with imaging at 3 and 6 months.
Week 6. Resume full physical activity including gym and heavy lifting. By this point the ureter and kidney have completely healed.
For a deeper look at the stent itself — why it hurts, what you can do about it, and how it differs by procedure — read our companion article on stent pain after stone surgery.
When To Call Your Urologist (Or Go Straight To The ER)
RIRS is a safe procedure but the post-operative period has a small but real complication rate. The complications that matter — and what to do about them — are listed below.
Red Flags After RIRS — Get Seen Today
If any of the following happen in the first two weeks after RIRS, do not wait until your follow-up appointment. Go to the emergency room or contact your urologist’s on-call service immediately:
- Fever above 38°C / 100.4°F — this can signal pyelonephritis (kidney infection) or urosepsis, both of which need IV antibiotics within hours.
- Heavy red bleeding, clots, or inability to urinate — clot retention can block the bladder and the kidney.
- Severe loin pain not relieved by your painkillers — this can mean the stent has migrated or the ureter is obstructed.
- Shaking chills (rigors) — even without a measured fever, rigors after stone surgery mean infection until proven otherwise.
- The stent string has come out (if your stent had one) — call your urologist within 24 hours so they can plan removal.
The two complications I worry about most are urosepsis (a systemic infection from bacteria entering the bloodstream through the kidney) and ureteric injury (rare with modern flexible scopes but possible if the ureter was tight on the way in).[8] Both are highly treatable when caught early. Both can become serious within hours if ignored. Trust your instincts — if something feels significantly worse than the discomfort your urologist warned you about, get checked.
Preventing The Next Stone
Here is a number that should make every stone-former pay attention: roughly 50% of patients who form one kidney stone will form another within 5–10 years without preventive measures.[9] RIRS is excellent at clearing the stone you have. It does nothing to stop the next one.
The single highest-yield change is hydration. Aim for a urine output of at least 2.5 litres a day, which usually means drinking 3 litres of fluid (around 100 fl oz / 12 cups) spread across the day. The second highest-yield change is reducing dietary sodium below 2,300 mg per day (about 1 teaspoon of salt), which lowers urinary calcium excretion.
If this is your second or third stone, ask your urologist to arrange a 24-hour urine collection and a metabolic workup — these tests find the specific reason your urine is forming stones (high calcium, low citrate, high oxalate, high uric acid) and let us tailor prevention to your chemistry rather than guessing. You can also use our Kidney Stone 5-Year Risk Profiler to estimate your individual recurrence risk based on diet, history, and clinical factors.
And know your stone. The composition of your stone — calcium oxalate, calcium phosphate, uric acid, struvite, cystine — determines the right prevention plan. If your urologist captured fragments at the time of RIRS, the lab analysis is gold; if not, your 24-hour urine results plus the stone’s CT appearance can usually tell us enough to act on.
Frequently Asked Questions
Is RIRS or PCNL better for a 15 mm lower pole kidney stone?
For a 15 mm lower pole stone, the AUA 2026 guideline gives mini-PCNL a moderate recommendation over URS/RIRS because of higher stone-free rates at one procedure. The trade-off is one extra night in hospital and a small bleeding risk. In my practice I will offer both options and let the patient weigh “one trip to theatre” against “no incision” — both are clinically reasonable. If you are anticoagulated or have a single kidney, that tips me toward RIRS. For more on the broader comparison, see our overview of all kidney stone surgeries.
How long does a flexible ureteroscopy (RIRS) procedure take?
Most RIRS procedures take 30 to 90 minutes from anaesthesia to wake-up. Stone size, stone density on CT (measured in Hounsfield Units), and whether the stone is in the lower pole all affect operative time. Hard stones over 1000 HU and lower pole stones take longest. The whole hospital visit — admission, surgery, recovery, discharge — usually runs 6–8 hours from arrival.
Why do I need a stent after RIRS if I went home the same day?
The flexible ureteroscope causes swelling in the ureter as it passes up and down. A swollen ureter can block urine drainage from the kidney, which can cause pain or, in worst case, infection. The stent keeps urine flowing past the swelling for 1–2 weeks while the ureter heals. Most patients tolerate the stent reasonably well with painkillers and tamsulosin — but stent discomfort is real, and the relief after removal is one of the most consistent observations in stone surgery.
What is the stone-free rate after one RIRS session?
For kidney stones under 2 cm, RIRS gives a stone-free rate of roughly 70–85% at one procedure. Upper pole and middle calyx stones do better; lower pole stones do slightly worse because gravity works against dust clearance. Stones over 2 cm drop to around 50–60% stone-free rate with RIRS — which is why the AUA recommends PCNL as first-line above that size threshold.
Can I have RIRS if I am on blood thinners like warfarin or a DOAC?
Yes — RIRS is one of the safer stone surgeries for anticoagulated patients, which is one of its advantages over PCNL. Your urologist will still want to coordinate with your cardiologist or haematologist about whether and how to interrupt the anticoagulation around surgery, but RIRS is often achievable without stopping blood thinners at all in carefully selected cases. PCNL, by contrast, almost always requires anticoagulation interruption because of its higher bleeding risk.
Does RIRS hurt during recovery?
Most patients describe RIRS recovery as uncomfortable rather than painful. The two main sources of discomfort are burning on urination (usually settles in 3–5 days) and stent-related flank twinges (settle after stent removal at week 2). Severe loin pain after the first 24 hours is not normal and should prompt a call to your urologist — it can signal stent migration or ureteric obstruction.
References
- Pearle MS, Matlaga BR, Antonelli JA, et al. Surgical Management of Kidney and Ureteral Stones: AUA Guideline (2026), Parts I–III. J Urol. 2026;215(2). AUA
- Geavlete P, Multescu R, Geavlete B. Pushing the boundaries of ureteroscopy: current status and future perspectives. Nat Rev Urol. 2014;11(7):373-382. PubMed
- Kronenberg P, Traxer O. The laser of the future: reality and expectations about the new thulium fibre laser — a systematic review. Transl Androl Urol. 2019;8(Suppl 4):S398-S417. PubMed
- Aboumarzouk OM, Monga M, Kata SG, et al. Flexible ureteroscopy and laser lithotripsy for stones >2 cm: a systematic review and meta-analysis. J Endourol. 2012;26(10):1257-1263. PubMed
- Ventimiglia E, Somani BK, Traxer O. Single use versus reusable flexible ureteroscopes: a systematic review. Curr Opin Urol. 2020;30(2):113-119. PubMed
- De S, Autorino R, Kim FJ, et al. Percutaneous nephrolithotomy versus retrograde intrarenal surgery: a systematic review and meta-analysis. Eur Urol. 2015;67(1):125-137. PubMed
- Srisubat A, Potisat S, Lojanapiwat B, et al. Extracorporeal shock wave lithotripsy (ESWL) versus percutaneous nephrolithotomy (PCNL) or retrograde intrarenal surgery (RIRS) for kidney stones. Cochrane Database Syst Rev. 2023;8:CD007044. Cochrane
- Somani BK, Giusti G, Sun Y, et al. Complications associated with ureterorenoscopy (URS) related to treatment of urolithiasis: the Clinical Research Office of Endourological Society URS Global Study. World J Urol. 2017;35(4):675-681. PubMed
- Scales CD Jr, Smith AC, Hanley JM, Saigal CS. Prevalence of kidney stones in the United States. Eur Urol. 2012;62(1):160-165. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.