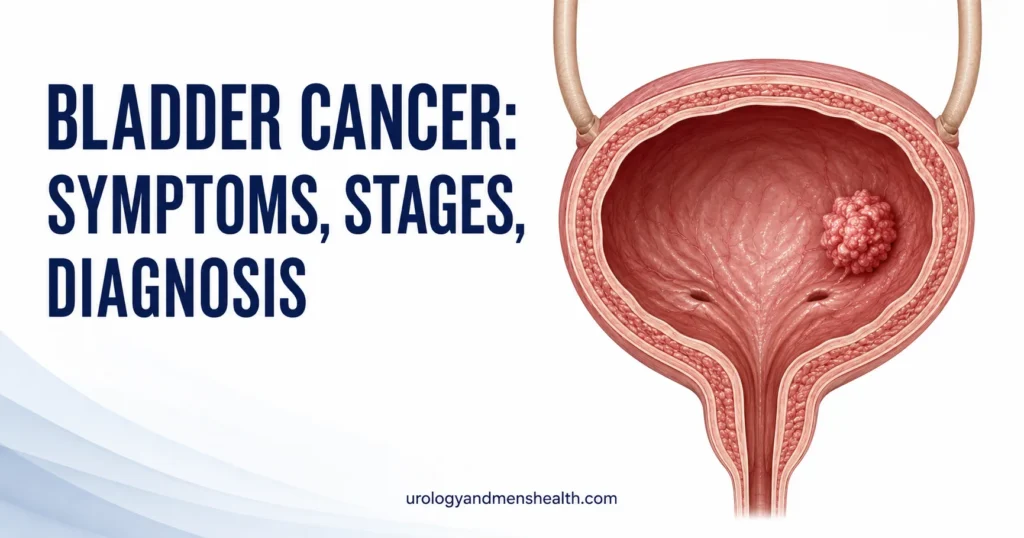
TURBT for Bladder Cancer: First Procedure (Urologist)
TURBT for bladder cancer is the only operation in urology that diagnoses and treats the disease in the same sitting. Here's exactly what happens between the moment you're wheeled into theatre and the moment you read your pathology report — and why the quality of this first procedure shapes everything that follows.

A TURBT for bladder cancer is the only operation in urology where the diagnosis and the treatment happen in the same sitting. You go to sleep with a bladder mass seen on a scan; you wake up with that mass removed, sitting in a specimen jar on its way to pathology. Most men I see for this procedure are anxious about two things — the catheter, and what the report will say. Both are reasonable concerns, and both are easier to handle when you know what’s actually happening at each step. This guide walks you through exactly what a transurethral resection of bladder tumor involves, why it’s done this way, what your pathology report will mean, and how the next few weeks unfold. For the broader picture of recovery from urological procedures, see our Surgery & Recovery Hub.
Key Takeaways
- TURBT is both a diagnostic biopsy and a definitive first treatment — the entire visible tumor is removed during the same procedure.
- Around 75% of bladder cancers are non-muscle-invasive at first diagnosis, meaning TURBT alone may be curative or buy you years of surveillance instead of major surgery.
- A catheter stays in for 24-48 hours afterward; pink urine for 1-2 weeks is normal, but bright red urine with clots is not.
- The pathology report drives everything: stage (Ta, T1, T2, CIS), grade (low or high), and whether muscle was present in the specimen.
- If the pathology shows T1 or high-grade disease, a second “re-TURBT” within 6 weeks is the AUA standard — not a sign that the first surgery failed.
What a TURBT Actually Is
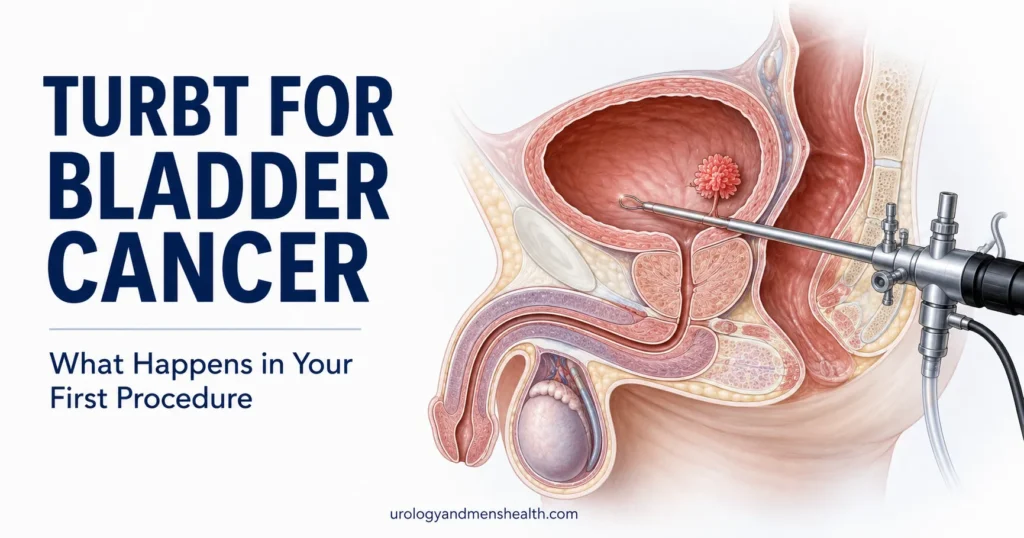
TURBT stands for transurethral resection of bladder tumor. “Transurethral” means I reach the bladder through your urethra — no skin cuts, no abdominal incision. “Resection of bladder tumor” means I shave the tumor off the bladder wall, layer by layer, using a specialized instrument called a resectoscope.
The resectoscope is essentially a slim metal telescope with a wire loop at the tip. The loop carries a low-voltage current that lets me cut and seal blood vessels at the same time. I pass it into the bladder, fill the bladder with sterile irrigation fluid to expand it like a balloon, then use the loop to slice through the tumor in deliberate layers.
Here is the part most patients don’t realize: I’m not just trying to remove what I can see. A good TURBT goes deeper than the obvious tumor. I deliberately resect down through the lamina propria (the layer beneath the urothelium) and ideally include a strip of detrusor muscle in the specimen. Why? Because the pathologist needs to look at the muscle layer to tell whether the cancer has invaded it. Without muscle in the specimen, the staging is incomplete, and a repeat TURBT becomes mandatory.
The procedure typically takes 30 to 60 minutes for a single tumor under 3 cm. Larger or multiple tumors can stretch it to 90 minutes. You’re under either spinal or general anesthesia — your anesthetist will decide based on your medical history, and either works well for this operation.
Why TURBT Is Done as Your First Procedure
Most men land in my clinic for a TURBT after one of two pathways. Either they had visible blood in their urine (hematuria) that led to a CT urogram and a flexible cystoscopy showing a bladder mass, or a routine ultrasound for something else picked up a thickened bladder wall or a polypoid growth. In either case, the next investigation is not another scan — it’s the TURBT itself.
This is what surprises patients. They expect a needle biopsy first, then surgery later if the biopsy is positive. Bladder cancer doesn’t work that way. The bladder wall is too thin and too vascular for a percutaneous needle. The safest, fastest, and most informative way to get tissue is to remove the tumor itself.
So the TURBT serves three jobs simultaneously:
- Diagnosis — confirms whether the lesion is cancer, what type, and how aggressive
- Staging — tells us how deep the tumor has invaded the bladder wall
- Treatment — physically removes the visible disease, which for many men is the only cancer treatment they will ever need
Around three out of four bladder cancers are non-muscle-invasive at first presentation [1]. For those men, a well-done TURBT plus appropriate follow-up surveillance is often the complete treatment plan. No chemotherapy, no radiotherapy, no cystectomy. That is why the quality of your first TURBT matters so much — it sets the ceiling on how good your long-term outcome can be.
In My Practice
The most common moment of recognition in my clinic isn’t during the cystoscopy itself — it’s the day a patient sees his pathology report and reads the word “carcinoma.” Even when I’ve prepared him, even when we’ve discussed the biopsy result is likely cancer, the word on the page hits differently. I tell every patient before their TURBT: when you read that report, what matters is not the word “cancer” — it is the four pieces of information beside it. Stage. Grade. Muscle present yes or no. CIS present yes or no. Everything else flows from those four data points.
If your report names all four clearly, the surgery did its job. If even one is missing, ask your urologist whether a re-TURBT within six weeks is appropriate before any other treatment is started.
The Day of Your TURBT
You arrive at the hospital fasted from midnight — no food, no water, no chewing gum. Most centers admit you the morning of surgery rather than the night before. Bring a small bag with loose-fitting clothes for the trip home, your regular medications in their original packaging, and your most recent imaging on a disc if you have it.
Pre-op assessment
The anesthetist will see you first. Expect questions about previous anesthetics, drug allergies, blood-thinning medications, and your last meal. Tell them honestly about any blood thinners — aspirin, clopidogrel, warfarin, apixaban, rivaroxaban. Most will have been stopped 5-7 days before based on your urologist’s instructions, but cross-checking matters. If you were not told to stop them and you’ve taken your usual dose, say so — surgery may need to be deferred 24-48 hours.
Anesthesia
You’ll be offered either general anesthesia (you’re fully asleep) or spinal anesthesia (you’re awake but numb from the waist down, usually with sedation). For a tumor on the side wall of the bladder, near the obturator nerve, many urologists prefer general anesthesia with muscle relaxation — it prevents the leg-jerk reflex that can cause the resectoscope to perforate the bladder. Ask your urologist which they recommend and why.
The procedure itself
Once you’re asleep, your legs are placed in stirrups and the surgical area cleaned with antiseptic. I pass the resectoscope through the urethra into the bladder under direct vision on a monitor. The bladder is filled with sterile irrigation. I systematically inspect every wall — anterior, posterior, lateral, dome, trigone — and document what I see. Then I resect each visible tumor, send fragments to pathology, and take additional biopsies from any suspicious flat areas. At the end, I cauterize the base of each resection site to stop bleeding.
A Post-Operative Recovery Timeline tool can help you map out the next few weeks once your surgery date is set. A urinary catheter goes in before you wake up. It’s connected to a bag of saline that runs continuously through the bladder for the first 12-24 hours to flush out blood and prevent clots — this is called continuous bladder irrigation.
Single-dose intravesical chemotherapy
If the lesion looks like a typical low-grade tumor and there’s no perforation, AUA and EAU guidelines recommend a single dose of intravesical chemotherapy (usually mitomycin C or gemcitabine) instilled into the bladder within 6-24 hours after the resection [2]. This reduces the risk of tumor recurrence by about 35% over the next two years. Not every patient is a candidate — high-grade tumors, deep resections, or any suspicion of perforation are contraindications. If your team doesn’t mention it, ask whether you qualify.
Preparing for urological surgery? Download Dr. Khalid’s Urology Surgery Recovery Guide.
Enter your email below to receive Dr. Khalid’s complete Urology Surgery Recovery Guide as a free, printable PDF.
What Your Pathology Report Will Say
Your TURBT specimen typically reaches the pathologist within 24 hours and a final report follows in 7-14 days. The report is dense and uses technical language, but four pieces of information matter most. Memorize them before your follow-up appointment.
Stage (how deep)
- Ta — tumor confined to the urothelium (innermost lining). The most favorable stage.
- T1 — tumor invades the lamina propria (the layer beneath the lining). Still non-muscle-invasive, but more aggressive.
- T2 — tumor invades the detrusor muscle. This is muscle-invasive bladder cancer and changes the entire treatment plan — usually toward cystectomy or chemoradiation rather than further TURBT.
- CIS (carcinoma in situ) — flat, high-grade cancer cells confined to the urothelium. Aggressive despite being technically non-invasive. Often coexists with Ta or T1 disease.
Grade (how aggressive)
Bladder cancer is graded as either low-grade (slow-growing, less likely to recur or progress) or high-grade (more aggressive, higher recurrence and progression risk). A high-grade T1 tumor is treated very differently from a low-grade Ta tumor, even though both are technically non-muscle-invasive.
Muscle present in specimen — yes or no
If the report does not explicitly state that detrusor muscle was present in the specimen, the staging is incomplete. Up to 1 in 4 patients with apparent T1 disease are upstaged to T2 on re-TURBT [3]. Ask your urologist directly: “Was muscle in my specimen?” If the answer is no, request a re-TURBT within 6 weeks before any maintenance treatment begins.
CIS — present or absent
CIS dramatically changes prognosis even when the dominant tumor is otherwise low-stage. A Ta low-grade tumor alone may need only surveillance. A Ta low-grade tumor with CIS elsewhere in the bladder is treated as high-risk disease, with intravesical BCG immunotherapy.
Recovery Week by Week
Most men go home either the same day or after one overnight stay. The catheter usually comes out before discharge or the following morning. Plan for someone to drive you home — you cannot drive for at least 24 hours after general anesthesia, and longer if you’re still passing visible blood.
Week 1: bleeding and burning
Expect pink or light-red urine for 7-14 days, with occasional darker episodes especially after physical activity. A burning sensation when you urinate is normal — the resection sites are essentially small internal wounds. Drink 2-2.5 liters of water daily (around 70-85 fl oz / 8-10 cups) to keep the urine dilute, which speeds healing and reduces clot risk. Paracetamol (acetaminophen) handles most of the discomfort; avoid aspirin and ibuprofen for the first 7-10 days unless your team specifically clears them, because they increase bleeding.
Week 2: back to desk work
Most desk-based jobs are manageable from day 7-10. Avoid heavy lifting (anything above 10 kg / 22 lb), straining, and prolonged sitting that puts pressure on the perineum. Long drives are not ideal — break them into 30-minute segments.
Week 3-4: light exercise
Walking and light cycling are fine. Avoid running, weightlifting, and contact sports until at least week 4. Sexual activity can resume around week 2-3 once urine is clear and there is no discomfort.
Week 5-6: full activity and first follow-up
Most men return to full activity by week 5-6. Your first follow-up cystoscopy is typically at 3 months — sooner if pathology was high-risk and intravesical treatment is starting. The follow-up cystoscopy is done in clinic with a flexible scope, takes about 5 minutes, and rarely requires more than topical anesthetic gel.
When to Go to the ER
The following symptoms after a TURBT need same-day assessment, not a follow-up appointment next week:
- Bright red urine with visible clots that does not clear after 1-2 hours of drinking water and rest — clot retention can block the catheter or, after catheter removal, the urethra itself.
- Unable to pass urine at all after the catheter has been removed — this is acute urinary retention and needs re-catheterization within 6 hours to prevent bladder injury.
- Fever above 38.5°C (101.3°F), shaking chills, or burning urine that is worsening rather than improving from day 3 onward — possible urinary tract infection or urosepsis.
- Severe lower abdominal pain that is sharp, sudden, and unrelieved by paracetamol — rare but raises concern for bladder perforation, especially in the first 48 hours.
- Persistent vomiting or inability to keep fluids down — affects healing and may indicate ileus or a post-anesthetic complication.
Bring your discharge summary and the name of the consultant who did your surgery when you present to the ER. It cuts the assessment time significantly.
What Comes After TURBT
Once the pathology report is finalized, your urologist will place you in one of three risk groups based on AUA/SUO 2024 guidance for non-muscle-invasive bladder cancer [4]. Each group has a different follow-up and treatment pathway.
Low risk
Single, primary, Ta low-grade tumor less than 3 cm with no CIS. Treatment is surveillance: cystoscopy at 3 months, then 9 months, then yearly. No further surgery, no intravesical treatment unless recurrence happens. Around half of these tumors do recur within 5 years, but progression to muscle-invasive disease is rare (under 5%).
Intermediate risk
Multifocal, recurrent, or larger (>3 cm) Ta low-grade tumors without CIS or T1. Treatment is induction intravesical chemotherapy (usually mitomycin C or gemcitabine) weekly for 6 weeks, with cystoscopy every 3-6 months for the first 2 years.
High risk
Any high-grade tumor, any T1 stage, or any CIS. Treatment is a repeat TURBT within 6 weeks (to confirm staging and remove residual disease), followed by induction intravesical BCG immunotherapy weekly for 6 weeks, then maintenance BCG for 1-3 years. Cystoscopy every 3 months for the first 2 years. If BCG fails or muscle invasion is found on re-TURBT, the conversation shifts toward radical cystectomy (bladder removal) or chemoradiation.
The treatment decision here matters because the wrong choice on this branch is the moment a curable cancer becomes incurable. If your risk stratification was based on a TURBT specimen without muscle, push back. If you’re being offered surveillance for a high-grade T1, get a second opinion. The Urology Surgery Comparison Tool can help you frame questions about more invasive options if cystectomy enters the discussion later.
One last point that connects bladder cancer to the rest of urological oncology: like kidney masses and renal cell carcinoma, bladder cancer is far more treatable when caught early. The men who do best are not the ones with the most aggressive treatment — they are the ones whose first procedure was thorough, whose pathology was complete, and who showed up for every follow-up cystoscopy on schedule.
Frequently Asked Questions
Is TURBT for bladder cancer painful?
The procedure itself is painless because you’re under general or spinal anesthesia. Afterward, expect a burning sensation when urinating for the first 7-10 days, similar to a urinary tract infection, plus mild lower abdominal discomfort. Paracetamol (acetaminophen) controls most of it. Severe pain is not normal and warrants the same-day ER assessment described in our guide on hematuria and post-procedure bleeding.
How long does a TURBT procedure take?
A standard TURBT for a single tumor under 3 cm typically takes 30-60 minutes of operating time. Multiple tumors, larger tumors, or tumors in awkward locations (dome, anterior wall) can stretch the procedure to 90 minutes. Total time in theater including anesthesia, positioning, and recovery is usually 2-3 hours.
How long until I get my TURBT pathology results?
Most centers turn around the report in 7-14 days. Complex specimens needing additional immunohistochemistry can take up to 3 weeks. If you have not been contacted within 14 days, phone your urologist’s secretary — do not wait for a letter. The four data points to confirm: stage, grade, muscle present, and CIS status.
Will I need a second TURBT?
Yes, in two situations: if your first specimen did not contain detrusor muscle (incomplete staging), or if the pathology showed T1 or any high-grade disease. AUA 2024 guidance is for re-TURBT within 6 weeks in both cases. A re-TURBT is not a sign that the first surgery failed — it is the standard of care for thorough staging in higher-risk disease.
Can a TURBT cause erectile dysfunction or incontinence?
True erectile dysfunction is uncommon after TURBT because the nerves controlling erection run outside the bladder and are not in the resection field. Incontinence is also rare because the bladder neck and external sphincter are deliberately avoided. Some men do have temporary urinary urgency, frequency, or mild stress leakage for a few weeks, which usually settles. If these persist past 6 weeks, mention it at your follow-up.
What’s the difference between TURBT and a bladder biopsy?
A “bladder biopsy” usually refers to taking small tissue samples from a suspicious flat area during a cystoscopy — this is part of a TURBT, not a substitute for it. TURBT removes the entire visible tumor down through the bladder wall layers; biopsy just samples the surface. For any raised or papillary lesion, TURBT is the correct procedure because it provides both diagnosis and treatment.
References
- Burger M, Catto JWF, Dalbagni G, et al. Epidemiology and risk factors of urothelial bladder cancer. European Urology. 2013;63(2):234-241. PubMed
- Sylvester RJ, Oosterlinck W, Holmang S, et al. Systematic review and individual patient data meta-analysis of randomized trials comparing a single immediate instillation of chemotherapy after transurethral resection with TUR alone in patients with stage pTa-pT1 urothelial carcinoma of the bladder. European Urology. 2016;69(2):231-244. PubMed
- Cumberbatch MGK, Foerster B, Catto JWF, et al. Repeat transurethral resection in non-muscle-invasive bladder cancer: a systematic review. European Urology. 2018;73(6):925-933. PubMed
- Holzbeierlein JM, Bixler BR, Buckley DI, et al. Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Guideline (2024 Amendment). Journal of Urology. 2024. AUA
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.