Top 3 Prostate Supplements: Urologist Evidence Review
When struggling with constant nighttime bathroom trips, a patient's first instinct is often to grab whatever "prostate support" bottle has the best reviews at the pharmacy. The medical reality is that this is a three-billion-dollar industry largely built on exaggerated claims, though a few specific compounds do have genuine science behind them. This guide cuts through the marketing to deliver a strict clinical review of saw palmetto, beta-sitosterol, and pygeum, detailing exactly what works and what you should leave on the shelf.


Prostate supplements are a $3 billion-a-year global market, and the shelf in any US drugstore tells you why — every bottle promises better flow, fewer nighttime bathroom trips, and “support” for an organ most men can’t locate on a diagram [1]. As a urologist who treats benign prostatic hyperplasia (BPH) every clinic day, I get asked about these products constantly. Patients want a single answer: do they work, or am I being sold hope in a capsule?
The honest answer is uncomfortable, because it doesn’t match the marketing on either side. A few have modest, real evidence behind them. Most have far less than the labels suggest. And none of them replace evidence-based medical treatment when symptoms have moved past mild. This is a clinical evidence review of the three most-asked-about products — saw palmetto, beta-sitosterol, and pygeum — examining what the randomized controlled trials actually show, where the evidence holds up, and where it falls apart under modern scrutiny.
Key Takeaways
- Saw palmetto is the world’s best-selling prostate supplement, but the two largest, most rigorous US trials (STEP 2006 and CAMUS 2011) showed no benefit over placebo at any dose — even at triple the standard 320 mg dose [2][3]
- Beta-sitosterol has the strongest evidence of the three: a Cochrane review of 519 men found a 4.9-point IPSS reduction and a 3.91 mL/s peak flow improvement versus placebo [4]
- Pygeum shows possible modest symptom benefit in older trials, but the evidence base is dated, small, and methodologically weak — no NIDDK-quality modern trial exists [5]
- No prostate supplement reduces prostate volume, prevents prostate cancer, or replaces tamsulosin or finasteride for moderate-to-severe symptoms
- Supplements are regulated as food, not drugs — up to 25% of herbal products do not contain the labeled ingredient at the claimed dose [7]
- Phytosterol-containing supplements can artifactually lower PSA, potentially masking early prostate cancer — always tell your doctor before a PSA test
The Supplement Problem: Why “Natural” Doesn’t Mean “Proven”
Before looking at any individual product, you have to understand a regulatory gap that explains nearly everything about why supplement evidence is so inconsistent. It is not that researchers are biased against supplements. It is that the products themselves vary, often dramatically, from bottle to bottle.
Prescription BPH medications — tamsulosin, finasteride, dutasteride — go through Phase I, II, and III trials involving thousands of patients before a US doctor can prescribe them. Every tablet contains a chemically defined active compound at exactly the dose on the label. The FDA verifies this. Long-term safety is monitored continuously after approval.
Dietary supplements are regulated as food in both the US (under DSHEA) and most international markets. Manufacturers do not need to prove a product works before it can be sold. They only need to avoid making explicit disease-treatment claims, though “supports prostate function” and similar phrases skirt that line by design. There is no requirement for standardized extraction methods, consistent active-ingredient concentrations, or third-party purity testing.
This means two bottles of “saw palmetto 320 mg” from different manufacturers can contain wildly different concentrations of the putative active compounds — fatty acids and phytosterols. Independent DNA-barcoding analyses of North American herbal supplements found that up to 25% did not contain the labeled ingredient at the claimed dose, and several contained undeclared substitutes [7]. You may genuinely be paying for what is essentially a placebo — even when the original ingredient does have evidence behind it.
Supplement #1: Saw Palmetto (Serenoa repens)
What it is
An extract from the berries of the American dwarf palm tree, native to the southeastern US. Standard formulations are theoretically standardized to 80–90% fatty acids and sterols. It is the world’s best-selling prostate supplement, with annual US sales over $700 million. You will see it sold under brand names like Super Beta Prostate, Prostagen, and Walgreens Prostate Health, often combined with other ingredients.
What the marketing claims
Reduces enlarged prostate symptoms, improves urinary flow, decreases nocturia (nighttime urination), and “supports prostate health.” Some product pages claim it works similarly to finasteride by inhibiting 5-alpha reductase — the enzyme that converts testosterone to dihydrotestosterone (DHT), the hormone that drives prostate growth.
What the evidence actually shows
Early small trials in the 1990s and early 2000s suggested modest benefit, which drove saw palmetto to bestseller status. But the two definitive trials — large enough and rigorous enough to provide a reliable answer — both found no benefit over placebo.
The STEP trial (NEJM 2006) was an NIDDK-funded, double-blind, placebo-controlled randomized controlled trial of 225 men with moderate-to-severe BPH symptoms. After 12 months on saw palmetto 320 mg/day, there was no significant improvement in AUASI symptom score, peak urinary flow, prostate size, post-void residual, or quality of life compared to placebo [2].
The CAMUS trial (JAMA 2011) was an even larger NIDDK-funded RCT designed to test whether the issue was simply dose. Investigators escalated saw palmetto to 960 mg/day — three times the standard dose — over 72 weeks in 369 men. The result: no improvement at any dose. Even at triple dose, saw palmetto matched placebo on every prespecified outcome [3].
A 2012 Cochrane review pooling 32 trials and over 5,600 men reached the same conclusion: Serenoa repens was not more effective than placebo for treatment of urinary symptoms consistent with BPH [8]. The American Urological Association (AUA) BPH guidelines reflect this — saw palmetto is not recommended as evidence-based therapy [6].
The clinical verdict
Not recommended. The highest-quality evidence consistently shows no benefit over placebo. The earlier positive trials that drove its commercial success were small, methodologically weaker, and likely affected by publication bias. If saw palmetto were submitted to the FDA today as a new BPH drug, it would not receive approval based on this evidence profile.
➡️ Check your IPSS prostate symptom score before deciding on any treatment — supplement or prescriptionSupplement #2: Beta-Sitosterol
What it is
A plant-derived sterol (phytosterol) found naturally in fruits, vegetables, nuts, and seeds. It is chemically similar to cholesterol and is the active ingredient in cholesterol-lowering functional foods like Benecol and certain margarines. For prostate use it is sold as a concentrated capsule, typically dosed at 60–130 mg/day.
What the evidence actually shows
Beta-sitosterol has the strongest evidence profile of any prostate supplement — though that ranking still places it well below prescription BPH medication.
A 2000 Cochrane review analyzed four RCTs involving 519 men and found that beta-sitosterol significantly improved urinary symptom scores — a weighted mean reduction of 4.9 points on the IPSS — and improved peak urinary flow by 3.91 mL/s compared to placebo [4]. These are clinically meaningful changes. An IPSS reduction of 4 to 5 points typically represents a noticeable shift in how a patient describes their symptoms.
However, four caveats apply, and they are not minor:
- The trials were small (largest was 200 patients) and short — the longest follow-up was 6 months
- Long-term data beyond 18 months is essentially absent
- Beta-sitosterol does not reduce prostate size — it likely improves symptoms through anti-inflammatory and smooth-muscle relaxation effects rather than through volume reduction (the mechanism finasteride uses)
- There is no evidence it slows BPH progression or prevents prostate cancer
The clinical verdict
The best evidence of the three. May reasonably be considered for men with mild BPH symptoms (IPSS under 8) who prefer a non-pharmaceutical first step, provided they understand the limitations and have had baseline urological assessment. It should not substitute for tamsulosin or finasteride in moderate-to-severe symptoms (IPSS 8 or above), and it should not delay urological evaluation for significant lower urinary tract symptoms.
Supplement #3: Pygeum (Prunus africana)
What it is
An extract from the bark of the African cherry tree, used for decades in French and Italian urological practice and prescribed in those countries before being repackaged as a supplement in the US and UK. It contains a mixture of phytosterols, pentacyclic triterpenes, and ferulic acid esters. Typical dose is 100–200 mg/day.
What the evidence actually shows
A 2002 Cochrane review of 18 RCTs involving 1,562 men found that men taking pygeum were more than twice as likely to report symptomatic improvement compared to placebo. Modest improvements in peak urinary flow (+2.5 mL/s) and a reduction of about 0.75 nocturia episodes per night were reported [5].
The problems with this evidence are substantial:
- Most trials were published before 2000, used inconsistent dosing and extraction methods, and had short follow-up (30–120 days)
- Many trials were small (under 100 participants) and would not meet modern methodological standards
- The Cochrane review itself concluded the evidence was limited by short trial duration and small sample sizes
- No large, modern, NIDDK-quality trial has ever been conducted, and the demand for one is unlikely to be met
The clinical verdict
Insufficient evidence for a confident recommendation. The existing data suggests possible modest benefit, but the evidence base is dated and methodologically weak. If a modern large-scale trial were conducted, pygeum might prove genuinely effective — or it might follow saw palmetto into the category of supplements that looked promising in small trials and failed under rigorous testing. Without that data, I do not recommend it.
➡️ Read next: Enlarged Prostate (BPH) — When Medication Fails and Surgery Becomes the Answer→ Related Read: The same evidence test applied to creatine.The PSA Warning: How Supplements Can Mask Cancer
This is the safety concern the marketing conveniently omits. Some prostate supplements — particularly those containing phytosterols and saw palmetto — can artificially lower PSA levels [9]. While that may sound like a feature, it is a clinical danger.
PSA is the primary blood-based screening biomarker for prostate cancer. If a supplement suppresses your reading, the result is a false sense of security — your PSA appears reassuring while a clinically significant cancer continues to grow undetected. This is not theoretical. Case reports exist of men on prostate supplements whose cancer diagnosis was delayed because their PSA was artifactually lowered, and the cancer progressed in the meantime.
If you take any prostate supplement, tell your doctor before having a PSA test, every single time. Specifically, ask whether you should discontinue the supplement for a 4 to 6 week washout period before testing, or whether your reported PSA needs to be adjusted upward in interpretation. Do not assume a “normal” PSA is reliably normal while you are on these products.
➡️ Read next: Prostate Cancer Screening — The Age-by-Age Guide Every Man NeedsWhat About Zinc, Selenium, and Lycopene?
These three nutrients are routinely included in “prostate formula” multi-supplements sold in US drugstores. Their evidence profiles are worth knowing because two of the three are not just unhelpful — they may carry real risk.
Zinc. The prostate naturally contains the highest zinc concentration of any organ in the body, and zinc-deficient prostate tissue has been observed in cancer specimens. This biological observation drove the supplement industry. But zinc supplementation has not been shown to prevent prostate cancer or treat BPH. Worse, the Health Professionals Follow-Up Study found that supplemental zinc intake above 100 mg/day was associated with a 2.3-fold increased risk of advanced prostate cancer [10]. Get zinc from food — meat, shellfish, legumes — at the RDA of 11 mg/day. Skip the high-dose capsules.
Selenium. The SELECT trial — a massive randomized study of 35,533 men — found no benefit of selenium supplementation for prostate cancer prevention. Worryingly, men with high baseline selenium levels who took supplements showed a non-significant trend toward increased prostate cancer [11]. Selenium supplementation specifically for prostate health is not recommended.
Lycopene. The carotenoid that gives tomatoes, watermelon, and pink grapefruit their color. Observational studies suggest men with higher dietary lycopene intake have a modestly lower prostate cancer risk. But interventional trials with lycopene supplements have not reproduced that benefit — a pattern common in nutrition research, where whole-food effects do not transfer to extracted capsules. Eating tomato-based foods (sauce, soup, salsa) several times a week is reasonable advice. Buying lycopene capsules is not.
→ Related Read: The evidence on zinc, selenium, and lycopene specifically➡️ Use the Evidence-Based Supplement Matcher to see what (if anything) actually fits your urological profileWhen Supplements Become Dangerous: The Delay-of-Treatment Problem
The biggest risk of prostate supplements is not what they contain. It is what they replace. I regularly see men in clinic who delayed seeking medical attention for worsening urinary symptoms because they were “trying natural options first.” By the time they present, the prostate has grown significantly, the bladder has developed compensatory changes — trabeculation, diverticula, sometimes a chronically distended detrusor that no longer contracts well — and the condition now requires more aggressive intervention than it would have eighteen months earlier.
BPH is a progressive condition in many men. Tamsulosin can relieve symptoms within weeks. Finasteride and dutasteride can reduce prostate volume by 20–25% over 6 to 12 months and slow disease progression measurably. Supplements cannot do either of these things. Every month of delayed effective treatment is a month of potential structural change in the bladder that is not always fully reversible once it occurs.
The practical rule I give patients: if your symptoms are mild (IPSS under 8), do not significantly affect your sleep or quality of life, and you have had a proper urological assessment — IPSS scoring, digital rectal exam (DRE), PSA, and post-void residual measurement — then a 3-month trial of beta-sitosterol with symptom monitoring is not unreasonable. But if symptoms are moderate-to-severe, or worsen at any point during a supplement trial, prescription medication should not be further delayed. Ask your urologist specifically about tamsulosin first; if your prostate volume is over 40 mL on ultrasound, ask about adding finasteride or dutasteride.
➡️ Related: The 40+ Men’s Health Checklist — The 5 Tests You Actually NeedIn My Practice
The pattern I see most often is not the man who tries saw palmetto and quietly decides it doesn’t work. It is the man who has been on a “prostate formula” multi-supplement for two or three years before he ever sees me — usually because his wife pushed him in after a particularly bad night of nocturia. By that point his IPSS is 18 to 22, his bladder ultrasound shows trabeculation, and his post-void residual is 150 mL or more. He is not a candidate for a gentle medication trial anymore. He is a candidate for combination therapy or, in some cases, surgery. When I explain this, the response is almost always the same: “But the bottle said it would help.”
The supplement did not cause his BPH. It simply removed the prompt that would have brought him to a urologist eighteen months earlier, when his options were wider and the bladder changes had not yet set in.
Confused about which prostate symptoms warrant a urologist visit? Download Dr. Khalid’s Men’s Health Screening Checklist — the exact 5 tests every man over 40 should ask for.
Enter your email below to receive Dr. Khalid’s complete Men’s Health Screening Checklist as a free, printable PDF.
When to See a Doctor — Urgently
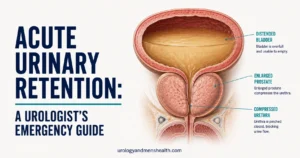
- Complete inability to urinate (acute retention). This is a urological emergency requiring immediate catheterization. Go to the ER. Do not attempt to treat with supplements or wait to “see if it passes.”
- Visible blood in your urine (hematuria). Always requires investigation — a CT urogram or cystoscopy — to rule out bladder or kidney pathology, regardless of prostate symptoms.
- Rapidly worsening urinary symptoms. Significant deterioration over weeks rather than months warrants urgent urological assessment, not a longer supplement trial.
- Recurrent urinary tract infections in a man. May indicate significant residual urine or another complication of untreated BPH. UTIs in men are never normal.
- Symptoms despite 3 months of supplement use. Time to move to evidence-based medical treatment. Further delay risks structural bladder changes that are not always reversible.
Frequently Asked Questions
Can I take prostate supplements alongside prescribed BPH medication like tamsulosin or finasteride?
Generally yes — most prostate supplements have no clinically significant pharmacological interactions with tamsulosin or finasteride. The harder question is what benefit you expect to add. If your prescribed medication is working, the evidence for additive benefit from saw palmetto, beta-sitosterol, or pygeum is essentially absent. The two genuine concerns are PSA interference (phytosterols can artifactually lower readings) and quality variability between products. Always disclose every supplement you take to your urologist, and ask specifically whether to discontinue them before any PSA testing.
Are prostate supplements safe to take long-term, or should I cycle off them?
Most are well-tolerated, with minor and usually temporary side effects — mild GI upset, occasional headache. The safety concern is less about direct toxicity and more about indirect harm: PSA suppression masking cancer, delayed treatment for progressive BPH, and a false confidence that “I’m doing something about my prostate” when that something has not been validated. Quality and contamination issues with unregulated US products are a meaningful additional concern [7]. Cycling off is not necessary if you continue them, but a 3-month trial period with objective re-assessment using your IPSS score is a far better framework than open-ended use.
Why does my pharmacist recommend prostate supplements if the evidence is weak?
Pharmacists in the US and most international markets are permitted to sell and recommend supplements as part of their retail role. Some genuinely believe the products help, drawing on earlier (now superseded) evidence from the 1990s. Others face commercial incentives — supplement margins are higher than prescription medication margins. The pharmacist is not necessarily wrong to offer them, but a retail recommendation is not equivalent to a urologist’s guideline-based clinical advice for symptomatic BPH.
Do prostate supplements prevent prostate cancer?
No prostate supplement has been demonstrated to prevent prostate cancer in a randomized trial. The SELECT study definitively showed no benefit from selenium or vitamin E across 35,533 men [11]. High-dose zinc above 100 mg/day may actually increase the risk of advanced prostate cancer [10]. The dietary approach with the strongest observational evidence is a Mediterranean-style pattern rich in tomatoes, cruciferous vegetables, and oily fish — but the benefit comes from the food, not from extracted supplement capsules. For evidence-based screening guidance, see our age-by-age screening guide.
What actually works for BPH symptoms if supplements don’t?
Evidence-based first-line treatments include alpha-blockers like tamsulosin, alfuzosin, and silodosin for symptom relief — these typically improve flow and reduce nocturia within 1 to 2 weeks. Five-alpha reductase inhibitors (finasteride, dutasteride) reduce prostate volume by 20–25% over 6 to 12 months and are useful when prostate size exceeds 40 mL on ultrasound. Combination therapy is recommended for moderate-to-severe symptoms with significant prostate enlargement. For men who fail medical therapy, surgical options include TURP, HoLEP, UroLift, and Rezum, all with strong evidence in the AUA and EAU guidelines [6]. The key is matching treatment intensity to the severity and structural picture, not symptom guesswork.
I have a strong PSA reading and I take saw palmetto. Should I stop before my next test?
Yes, and this is exactly the conversation to have with your doctor proactively. Phytosterol-containing supplements (which includes saw palmetto and beta-sitosterol products) can artifactually lower PSA readings, which means a “reassuring” result on the supplement may not actually be reassuring. The standard approach is a 4 to 6 week washout before PSA testing, with the next reading interpreted as the truer baseline. If your previous PSAs were taken while you were on a supplement and showed a flat trend, your true PSA velocity may be different — and worth re-evaluating.
References
- Grand View Research. Prostate Health Supplements Market Size Report, 2024–2030. Grand View Research.
- Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354(6):557–566. PubMed
- Barry MJ, Meleth S, Lee JY, et al. Effect of increasing doses of saw palmetto extract on lower urinary tract symptoms: a randomized trial. JAMA. 2011;306(12):1344–1351. PubMed
- Wilt T, Ishani A, MacDonald R, Stark G, Mulrow C, Lau J. Beta-sitosterols for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2000;(2):CD001043. PubMed
- Wilt T, Ishani A, MacDonald R, Rutks I, Stark G. Pygeum africanum for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2002;(1):CD001044. PubMed
- Sandhu JS, Bixler BR, Dahm P, et al. Management of Lower Urinary Tract Symptoms Attributed to Benign Prostatic Hyperplasia: AUA Guideline (2024). American Urological Association. AUA Guidelines
- Newmaster SG, Grguric M, Shanmughanandhan D, Ramalingam S, Ragupathy S. DNA barcoding detects contamination and substitution in North American herbal products. BMC Med. 2013;11:222. PubMed
- Tacklind J, MacDonald R, Rutks I, Stanke JU, Wilt TJ. Serenoa repens for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2012;(12):CD001423. PubMed
- Agbabiaka TB, Pittler MH, Wider B, Ernst E. Serenoa repens (saw palmetto): a systematic review of adverse events. Drug Saf. 2009;32(8):637–647. PubMed
- Leitzmann MF, Stampfer MJ, Wu K, Colditz GA, Willett WC, Giovannucci EL. Zinc supplement use and risk of prostate cancer. J Natl Cancer Inst. 2003;95(13):1004–1007. PubMed
- Lippman SM, Klein EA, Goodman PJ, et al. Effect of selenium and vitamin E on risk of prostate cancer and other cancers: the SELECT trial. JAMA. 2009;301(1):39–51. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.