Priapism: When an Erection Becomes a Medical Emergency
Most men assume a long erection is a good problem to have. When a patient arrives in the ER hours into a painful, unwanted one, I have to explain that priapism can scar the penis permanently — and that the clock started ticking hours ago.


Priapism is an erection that lasts more than four hours and has nothing to do with arousal — and despite how it sounds, it is one of the few genuine emergencies I deal with in men’s health. The blood that should drain away after an erection gets trapped, the tissue starves of oxygen, and every hour that passes raises the risk of permanent scarring and lasting erectile dysfunction. I have seen men wait overnight out of embarrassment, only to lose function that earlier treatment would have saved. The hard truth is that a rigid, painful erection at hour five is not a bedroom problem — it is a race against tissue death. This guide walks you through what priapism actually is, what causes it, what happens when you reach the emergency room, and the exact point at which you stop waiting and go. For the wider picture of erectile and penile conditions, see our complete Sexual Health Hub.
Key Takeaways
- An erection lasting more than 4 hours is ischemic priapism until proven otherwise — go to the ER, do not wait it out.
- Ischemic (low-flow) priapism is painful and starves penile tissue of oxygen; non-ischemic (high-flow) priapism after trauma is usually painless and less urgent.
- The most common triggers I see are ED injection therapy (Trimix), sickle cell disease, and certain psychiatric medications.
- First-line ER treatment is aspirating trapped blood and injecting phenylephrine; surgery is reserved for erections that don’t resolve.
What Is Priapism? Ischemic vs. Non-Ischemic
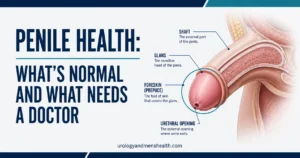
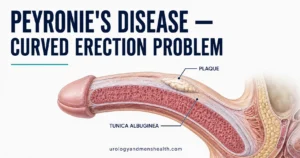
Priapism is a persistent erection that continues for hours beyond — or entirely unrelated to — sexual stimulation. A normal erection works like a sponge filling with blood and then squeezing it back out once arousal fades. In priapism, the squeeze-out step fails: blood enters the two main erection chambers (the corpora cavernosa) but cannot drain, so the penis stays rigid long after any desire has gone.
There are two very different types, and telling them apart changes everything about urgency. Ischemic (low-flow) priapism is the dangerous one. Trapped venous blood loses its oxygen, the tissue becomes acidic, and the erection is usually rigid and increasingly painful. Non-ischemic (high-flow) priapism usually follows a blow to the penis or perineum that tears a small artery, flooding the chamber with oxygenated blood. It is typically only partially rigid and not painful.
The reason this distinction matters: the AUA/SMSNA 2022 guideline treats prolonged ischemic priapism over four hours as a medical emergency, because the oxygen-starved tissue behaves like a limb with a tourniquet on it [1]. Non-ischemic priapism, by contrast, is not an emergency and is sometimes managed with observation alone. A urologist confirms which type you have with a corporal blood gas — a small sample of blood drawn from the penis that shows immediately whether the blood is oxygen-rich or oxygen-starved.
What Causes Priapism?
In my clinic, the single most common cause is treatment for the opposite problem: penile injection therapy for erectile dysfunction. Drugs like Trimix and papaverine work by forcing the erection chambers open, and occasionally they work too well. This is why I counsel every patient starting injections on the four-hour rule before they ever take the first dose. You can read how injections fit into the wider treatment ladder in our guide to penile injections when ED pills stop working.
Sickle cell disease is the leading cause in younger men and boys. The abnormally shaped red cells clump and block the small veins that should drain the penis, so episodes can be recurrent and start in childhood. Certain medications are another frequent trigger — particularly some antidepressants (notably trazodone), antipsychotics, and blood-pressure drugs. Because several blood-pressure and ED medications overlap here, it is worth understanding how blood pressure medication affects erections.
Other causes include recreational drugs (cocaine, cannabis, excess alcohol), blood disorders such as leukemia, pelvic or spinal cord injury, and trauma to the penis or perineum — the classic source of the non-ischemic type. In a meaningful minority of cases no clear cause is ever found, which is frustrating but does not change the emergency response.
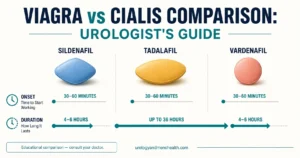
Why the oral ED pill fear is mostly misplaced
Many men worry that Viagra or Cialis will cause priapism. In reality, prolonged erections from standard oral doses are rare. The far higher-risk scenario is injection therapy or combining ED drugs with recreational substances. If your pills have stopped working and you are tempted to double up or add injections, that is a conversation to have with a urologist first — our article on what to do when Viagra stops working covers the safer next steps.
In My Practice
A man in his thirties once came in at 2 a.m., eleven hours into a rigid, painful erection after his second-ever Trimix injection. He had spent the evening hoping it would settle and the night too embarrassed to call. By the time we aspirated and injected phenylephrine, the blood gas already showed the dark, acidic pattern of oxygen starvation — and although we resolved the erection, he was left with reduced rigidity months later.
If an erection passes the four-hour mark, the embarrassment of an ER visit is nothing next to the cost of waiting — the tissue damage that matters is happening silently while you hesitate.
On ED injections or pills? Know exactly when a long erection becomes an emergency.
Enter your email below to receive Dr. Khalid’s complete Evidence-Based ED Action Plan as a free, printable PDF.
What Happens at the Hospital
The first thing a urologist does is work out which type of priapism you have, because conservative measures like ice packs or cold showers will not fix the ischemic type and only waste time [1]. Expect a focused history, an examination of the penis and perineum, and a corporal blood gas drawn directly from the erection chamber. Dark, acidic blood confirms ischemic priapism and the clock-driven pathway begins immediately.
For ischemic priapism, the AUA/SMSNA 2022 guideline sets out a stepwise plan. First, aspiration: a needle drains the trapped, oxygen-poor blood from the chamber. Next, an injection of phenylephrine directly into the penis, which tells the smooth muscle to contract and let blood drain — your blood pressure and heart rate are monitored throughout because the drug can raise both [2]. These two steps resolve the majority of cases.
If the erection persists despite aspiration and phenylephrine, the next step is a shunt — a small surgical channel that gives the trapped blood a route out. In refractory cases that have gone on long enough to scar, an early penile prosthesis is sometimes the most function-preserving option, because operating into fibrosed tissue later is far harder. The full implant route is covered in our guide to penile implant surgery for severe ED.
Non-ischemic (high-flow) priapism is handled completely differently. Because the tissue is still receiving oxygenated blood, there is no tissue emergency — many cases settle on their own, and treatment, when needed, involves imaging and selectively blocking the leaking artery rather than urgent aspiration.
Red Flags — When to Go to the ER
The rule is simpler than most men want it to be. The damage in ischemic priapism is time-dependent, and waiting “to see if it settles” is the single most common way men lose erectile function from this condition.
When to Go to the ER
Go to the emergency room — do not wait for a clinic appointment — if you have:
- An erection lasting more than 4 hours, whether or not it followed sex or medication.
- A rigid erection that is becoming painful — pain points strongly to the ischemic type.
- A prolonged erection after an ED injection (Trimix/papaverine) or after starting a new psychiatric medication.
- Any prolonged erection in a person with sickle cell disease or another blood disorder.
At the ER, say clearly: “I have had an erection for more than four hours.” That sentence moves you up the triage queue — this is treated as an emergency, not an embarrassment.
One practical instruction I give every patient on injection therapy: if you are not fully resolved by the three-hour mark, do not go to bed hoping — head to the ER then, so a urologist can intervene before you cross the four-hour line. If you have recurrent episodes from sickle cell disease, ask your hematologist and urologist together to write you a personal action plan naming which ER to attend and what to say on arrival. For the broader map of penile and erectile conditions, the Sexual Health Hub links the related guides in one place, and you can gauge your baseline erectile function with our IIEF-5 erectile function self-assessment.
After Priapism: Will Function Recover?
This is the question every man asks once the crisis passes, and the honest answer depends almost entirely on how long the episode lasted. Erections resolved within a few hours usually carry an excellent outlook. Episodes that ran well beyond the four-hour window carry a real risk of erectile dysfunction, because oxygen-starved smooth muscle can be replaced by scar tissue that no longer expands properly.
If you do develop ED afterward, it is treatable, and the same step-up ladder used for other causes applies — starting with oral medication and progressing as needed. Because priapism-related ED also has a vascular dimension worth screening, it is reasonable to ask your doctor whether your overall cardiovascular risk should be checked too; our ED vascular risk screener is a useful starting point, and the link between erections and heart health is explained in why morning erections are a cardiovascular check. For a structured overview of every ED treatment option, see our step-by-step ED treatment protocol.
Frequently Asked Questions About Priapism
How long is too long for an erection before it becomes priapism?
Four hours is the threshold. An erection lasting more than four hours is treated as ischemic priapism until a corporal blood gas proves otherwise, and it warrants an emergency room visit rather than waiting. The risk of lasting damage rises with every additional hour, so if you are on injection therapy and not resolved by three hours, our ED treatment guide advises heading in before you cross the four-hour line.
Can Viagra or Cialis cause priapism?
It can, but prolonged erections from standard oral doses are rare. The far higher risk comes from penile injection therapy such as Trimix, or from combining ED drugs with recreational substances. If your usual pill has stopped working, do not increase the dose yourself — the safer options are covered in our guide on what to do when Viagra stops working.
Why is sickle cell disease such a common cause of priapism?
In sickle cell disease, abnormally shaped red blood cells clump together and block the small veins that should drain the penis after an erection. This makes episodes recurrent and means they often begin in childhood or adolescence. Anyone with sickle cell disease should have a personal action plan naming which emergency room to attend and to state on arrival that they have had an erection for more than four hours.
What does the hospital actually do to treat ischemic priapism?
After confirming the type with a corporal blood gas, the urologist aspirates the trapped oxygen-poor blood and injects phenylephrine to make the chamber drain, monitoring your blood pressure and heart rate throughout. If that fails, a surgical shunt is created, and in long-standing refractory cases an early penile implant may best preserve function — explained further in our penile implant surgery guide.
Will I have erectile dysfunction after an episode of priapism?
It depends mostly on duration. Erections resolved within a few hours usually have an excellent outlook, while episodes lasting well beyond four hours carry a real risk of erectile dysfunction from scarring. If ED does develop it is treatable with the standard step-up approach; assessing your baseline with the IIEF-5 self-assessment helps track recovery.
Is a painless prolonged erection still an emergency?
A painless, only partially rigid erection — often after a blow to the penis or perineum — points to non-ischemic (high-flow) priapism, which is not a tissue emergency and sometimes settles on its own. However, you cannot reliably tell the two types apart at home, so any erection past four hours still needs same-day urological assessment to confirm which type you have before deciding whether to treat or observe.
References
- Bivalacqua TJ, Allen BK, Brock GB, et al. The Diagnosis and Management of Recurrent Ischemic Priapism, Priapism in Sickle Cell Patients, and Non-Ischemic Priapism: An AUA/SMSNA Guideline. J Urol. 2022;208(1):43-52. PubMed
- Scarberry K, Deebel N, Dutta R, et al. Safety and Efficacy of Phenylephrine Administration for the Treatment of Ischemic Priapism. Urology. 2022;169:115-119. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.