Ureteric Reflux in Adults: Symptoms & Diagnosis
Most people are told reflux is a childhood problem that disappears with age. When I see ureteric reflux in adults, it usually arrives disguised as a stubborn kidney infection that keeps coming back — and the kidney is the thing quietly paying the price.

Ureteric reflux in adults is one of those diagnoses most people assume can’t apply to them. Reflux — urine flowing backward from the bladder up toward the kidney instead of draining one way — is framed as a childhood condition that’s outgrown by school age. Often it is. But it doesn’t always vanish, and in some adults it was never caught at all. I usually meet it wearing a disguise: a man in his 30s or 40s with kidney infections that keep returning no matter how many antibiotic courses he finishes. For the full picture of how the urinary tract is meant to drain, see our complete Kidney Health Hub. The reason reflux matters isn’t the infection itself — it’s what years of pressure and bacteria do to the kidney behind it. This article explains what adult reflux is, how it’s diagnosed, and when it actually needs treatment versus watchful monitoring.
Key Takeaways
- Ureteric reflux in adults is uncommon, but when present it most often shows up as recurrent kidney infections (pyelonephritis), not bladder infections alone.
- The damage that matters is reflux nephropathy — focal kidney scarring that can quietly lower kidney function over years even when symptoms are mild.
- A voiding cystourethrogram (VCUG) is the test that confirms reflux and grades it from I to V; ultrasound alone can miss low-grade reflux.
- Low-grade adult reflux with normal kidneys is often managed conservatively, while high-grade reflux with scarring or breakthrough infections may need surgical correction.
What Ureteric Reflux Actually Is
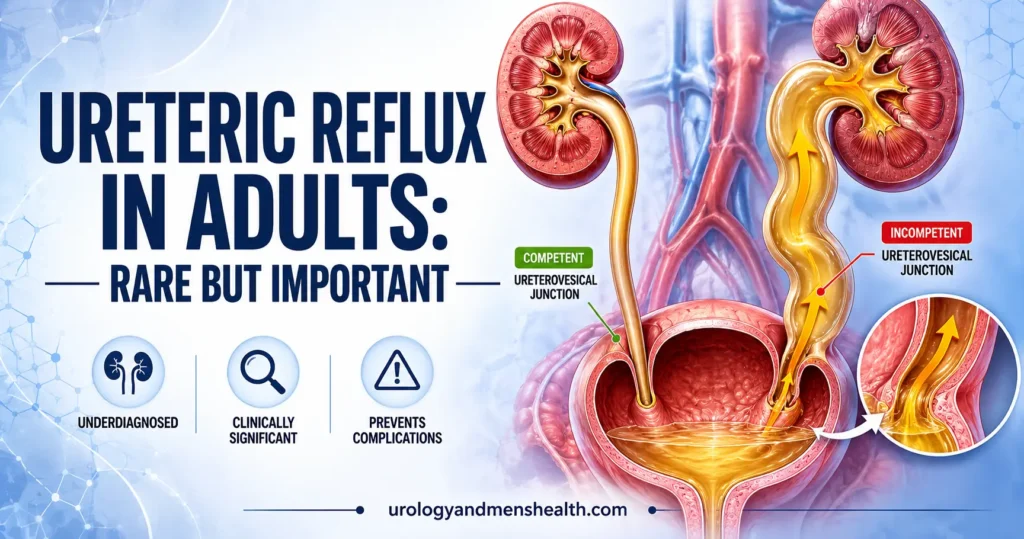
Your ureters are the two muscular tubes that carry urine from the kidneys down to the bladder. Where each ureter enters the bladder, it doesn’t just open through a hole — it tunnels at an angle through the thick muscular bladder wall for about a centimeter. That oblique tunnel works as a one-way flap valve. When the bladder fills and squeezes to empty, the rising pressure presses the tunnel shut, so urine is forced out through the urethra and not back up toward the kidney.
Vesicoureteral reflux happens when that valve fails. If the tunnel is too short or too straight, bladder pressure can no longer pinch it closed, and a jet of urine tracks backward up the ureter — sometimes all the way to the kidney. In children this is usually a congenital problem with how the junction formed. In adults, it’s either a milder congenital reflux that simply never resolved, or it’s secondary reflux: the valve is overwhelmed by high bladder pressures from another problem, such as a neurogenic bladder, severe bladder outlet obstruction, or prior pelvic surgery.
That distinction matters more in adults than in kids. Primary reflux is a plumbing defect at the junction. Secondary reflux is a pressure problem upstream — and if you only fix the valve without fixing the pressure, the reflux comes straight back.
The Symptoms That Bring Adults to a Urologist
Reflux itself causes no sensation. You cannot feel urine moving the wrong way. What you feel is the consequence — and in adults that is almost always infection reaching the kidney. The pattern I watch for is repeated episodes of pyelonephritis (a kidney infection): fever, chills, and a deep ache or tenderness in the flank, the area just below the back of the ribs, rather than the low burning of a simple bladder infection.
Each symptom points to a mechanism. The flank pain reflects the kidney itself becoming inflamed, because reflux delivered bacteria straight up to it. The high fever signals the infection has reached kidney tissue rather than staying in the bladder. And the sheer recurrence — three, four, five infections in a year despite correct treatment — is the clue that something structural is letting bacteria climb back up each time. When kidney infections keep returning in a man, reflux belongs on the list of causes to rule out, which is exactly why a structured workup matters. Our guide to the diagnostic workup for recurrent urinary infections in men walks through that process in detail.
Some adults have no infections at all and are picked up by accident — a dilated ureter or kidney scarring spotted on a scan done for another reason, or high blood pressure traced back to old kidney damage. A smaller group presents with vague, long-standing flank discomfort that worsens when the bladder is full.
In My Practice
The patient who taught me to never assume reflux is “a childhood thing” was a 38-year-old who had been treated for four kidney infections in 18 months, each time with a fresh antibiotic course and no further questions. By the time the VCUG was finally done, he had Grade IV reflux on one side and a kidney that had already lost a third of its function to scarring. Nobody had imaged the drainage because everyone assumed adults don’t reflux.
If kidney infections keep returning despite correct antibiotic treatment, the question is no longer which antibiotic — it’s why the bacteria keep reaching the kidney in the first place.
How Ureteric Reflux Is Diagnosed in Adults
Diagnosis follows a logical order, moving from cheap and non-invasive toward the definitive test only when the picture demands it. The first step is confirming and characterizing the infections with a urine culture, and checking kidney function with a blood creatinine and eGFR (estimated glomerular filtration rate, a measure of how well the kidneys filter). If you want to understand what those numbers mean, our CKD stage calculator shows how eGFR maps to kidney function stages.
Next comes imaging. A renal and bladder ultrasound is the usual starting scan because it’s harmless and shows obvious problems — a dilated ureter, a swollen kidney (hydronephrosis), or thinned, scarred kidney tissue. The catch is that ultrasound can look completely normal in low-grade reflux, because the urine refluxes only intermittently and the scan is a single snapshot. A normal ultrasound does not rule reflux out.
The definitive test is the voiding cystourethrogram (VCUG). A thin catheter fills the bladder with contrast dye, then X-ray images are taken while you urinate. If contrast tracks backward up a ureter, reflux is confirmed and graded on a standard scale from Grade I (urine reaches only the lower ureter) to Grade V (severe reflux with a grossly dilated, tortuous ureter and a swollen kidney). That grade drives every treatment decision that follows.
In selected adults a nuclear medicine scan (a DMSA renal scan) is added to map exactly where the kidney has been scarred and how much working tissue remains. This matters most when deciding whether a kidney is worth protecting surgically or has already been damaged beyond rescue.
Tired of kidney infections that keep coming back?
Enter your email below to receive Dr. Khalid’s complete 7-Day Kidney Stone Prevention Meal Plan as a free, printable PDF — built around the hydration and urine-dilution habits that also help protect a vulnerable kidney.
What Reflux Does to the Kidney Over Time
The condition that gives reflux its importance is reflux nephropathy — the permanent scarring of kidney tissue caused by the combination of backward pressure and recurrent infection. Each episode of infected urine reaching the kidney triggers inflammation, and inflammation that heals leaves a scar. Over years, those focal scars add up, the working filtering tissue thins, and the kidney’s overall function drifts downward.
This is why reflux is not just an infection nuisance. Reflux nephropathy is one of the recognized causes of chronic kidney disease, and in some people it surfaces decades later as unexplained high blood pressure or protein leaking into the urine. If a urine test ever shows protein, that finding deserves its own explanation — our article on what protein in the urine means covers why it can signal early kidney strain.
The damage is cumulative and largely silent, which is the frustrating part. A kidney can lose a meaningful share of its function before any blood test flags it, because the healthy kidney compensates. That’s the mechanical argument for taking adult reflux seriously even when an individual infection feels minor: you are not just treating today’s fever, you are trying to stop the next scar.
Treatment: When Reflux Needs Action and When It Doesn’t
Treatment is matched to the grade of reflux, the state of the kidneys, and whether infections are breaking through. The goal is always the same: protect kidney function and stop infected urine from reaching the kidney. How aggressively you pursue that depends on the risk.
Conservative management suits low-grade reflux (roughly Grade I–II) with normal kidneys and infrequent infections. This means treating infections promptly, staying well hydrated to keep urine flowing and dilute, emptying the bladder fully and on a regular schedule, and monitoring kidney function with periodic eGFR checks. For adults whose reflux is secondary to a pressure problem, fixing that upstream cause — relieving outlet obstruction, managing a neurogenic bladder — often resolves the reflux without ever touching the valve.
Surgical correction is considered for high-grade reflux (Grade III–V), progressive kidney scarring, or breakthrough kidney infections despite good conservative care. Two main options exist. An endoscopic bulking injection places a small amount of material beneath the ureteric opening through a cystoscope, lifting it into a competent valve — a day procedure with quick recovery, better suited to lower grades. Ureteric reimplantation is the more durable repair: the surgeon detaches the ureter and re-tunnels it through the bladder wall at a proper oblique angle to rebuild the one-way valve, with higher success rates for severe reflux at the cost of a bigger operation.
When to See a Doctor Promptly
Reflux turns dangerous when infection reaches a kidney that can’t drain. Seek same-day medical care or go to the emergency room if you have:
- Fever above 38°C (100.4°F) with pain or tenderness in your flank or back
- Shaking chills alongside any urinary symptoms
- A urinary infection that returns within days of finishing antibiotics
- Nausea, vomiting, and feeling generally very unwell with back pain
- Reduced urine output or visible blood in the urine during an infection
If you suspect reflux is behind your infections, the concrete next step is to ask your urologist directly: “Given how often these kidney infections keep coming back, should I have a VCUG to check for reflux?” Bring a list of every infection with rough dates and which antibiotic was used. If a scan shows scarring or your eGFR has dropped, ask whether a DMSA scan is warranted to map the damage before deciding on treatment — and request a repeat eGFR within three to six months to track whether function is stable.
Frequently Asked Questions
Can ureteric reflux in adults appear if I never had it as a child?
Yes. Some adults have primary reflux that was simply never detected in childhood because it caused no infections until later. Others develop secondary reflux when high bladder pressure — from outlet obstruction, a neurogenic bladder, or prior pelvic surgery — overwhelms a previously competent valve. Either way, the trigger to investigate is usually a pattern of recurrent kidney infections rather than a memory of childhood problems.
Why do I keep getting kidney infections if my bladder infections clear up fine?
That gap is itself a clue. Vesicoureteral reflux lets bacteria from the bladder travel back up to the kidney, so even when antibiotics clear the bladder, the reflux pathway keeps re-seeding the kidney. Recurrent pyelonephritis — fever and flank pain rather than just burning — in a man warrants imaging to look for a structural cause like reflux, obstruction, or stones.
Is a normal ultrasound enough to rule out reflux nephropathy?
No. Ultrasound can show advanced scarring, hydronephrosis, or a dilated ureter, but it frequently looks normal in low-grade reflux because the backflow is intermittent and the scan is a single moment in time. A voiding cystourethrogram is the test that actually confirms or excludes reflux, and a DMSA scan maps scarring that ultrasound underestimates.
Does adult ureteric reflux always need surgery?
No. Low-grade reflux with healthy kidneys and few infections is often managed conservatively with prompt infection treatment, good hydration, complete bladder emptying, and periodic kidney-function checks. Surgery is reserved for high-grade reflux, progressive kidney scarring, or infections that break through despite good conservative care.
Can ureteric reflux cause high blood pressure?
It can, indirectly. Long-standing reflux nephropathy scars the kidney, and scarred kidney tissue can drive up blood pressure through the renin-angiotensin system. This is one reason reflux nephropathy is sometimes first suspected when a younger adult is found to have unexplained hypertension alongside subtle signs of kidney damage on testing.
References
- American Urological Association. Management and Screening of Primary Vesicoureteral Reflux in Children: AUA Guideline (amended 2017). AUA Guidelines. AUA
- European Association of Urology. Paediatric Urology Guidelines: Vesicoureteral Reflux. EAU Guidelines. 2024. EAU
- National Institute of Diabetes and Digestive and Kidney Diseases. Vesicoureteral Reflux (VUR). NIDDK Health Information. NIDDK
- Mattoo TK, et al. Vesicoureteral Reflux and Reflux Nephropathy. Advances in Chronic Kidney Disease. 2011;18(5):348-354. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.