Adrenal Incidentaloma: When CT Findings Matter | UMH
The radiologist found a small mass on your adrenal gland that nobody was looking for. Most are harmless — but a few are hiding a hormone problem or an early cancer. Here's exactly how I work them up in clinic, and which findings make me pick up the phone.

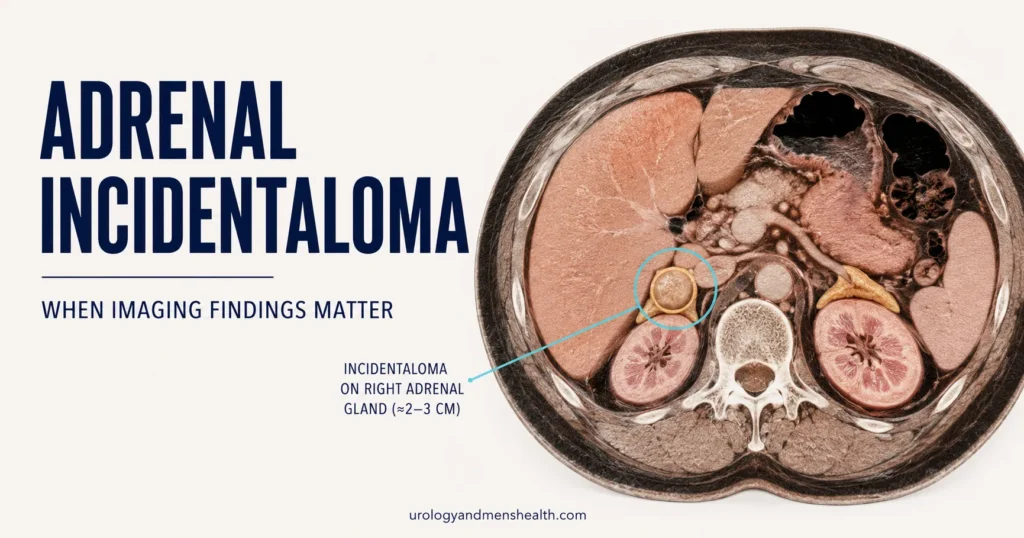
An adrenal incidentaloma is a mass on your adrenal gland that nobody was looking for. Someone scanned your belly for kidney stones, back pain, or a check-up — and the radiology report mentions a “1.8 cm nodule on the right adrenal, likely benign adenoma, recommend correlation.” That sentence sends thousands of men to my clinic every year, most of them terrified the scan has found a cancer. The truth is more interesting and much more reassuring. The majority of these masses are harmless. A small but important minority are quietly producing a hormone that is wrecking your blood pressure, your sleep, your bones, or your heart — and you would never know without the right tests. A smaller minority again are early cancers that need to come out. Your job, and mine, is to sort which one you’ve got. For the full overview of how a urologist thinks about screening tests at your age, see our complete Men’s Wellness Hub. This guide walks you through exactly how I work up an adrenal incidentaloma, what the imaging numbers mean, and when surgery is the right answer.
Key Takeaways
- Around 4-7% of abdominal CT scans pick up an adrenal incidentaloma; the rate rises sharply after age 50, and most are benign non-functioning adenomas.
- Every adrenal incidentaloma needs two things checked: imaging features (size, density, washout) and hormone function (cortisol, metanephrines, aldosterone).
- A mass that is under 4 cm, smooth, and measures < 10 Hounsfield units (HU) on non-contrast CT is almost certainly a benign adenoma.
- Surgery is the right answer when the mass is hormonally active, larger than 4 cm, or has suspicious imaging features — regardless of symptoms.
What an Adrenal Incidentaloma Actually Is
You have two adrenal glands. They sit like small triangular caps on top of each kidney, weigh about 5 grams each, and are responsible for an outsized share of your daily physiology. The outer layer (cortex) makes cortisol (your stress hormone), aldosterone (which controls your blood pressure and potassium), and a small amount of sex hormones. The inner core (medulla) makes adrenaline and noradrenaline. Almost every adrenal incidentaloma arises from the cortex.
The word “incidentaloma” is a clinical mash-up — incidental + adenoma. It means a mass found by accident on imaging done for some other reason, typically a CT for abdominal pain, back pain, kidney stones, or trauma. Modern CT scanners are so sensitive that they now find a nodule on roughly 4-7% of adult scans, and closer to 10% in men over 70.[1] Most are not new — they have been sitting there silently for years.
Here is the breakdown of what these masses turn out to be, drawn from the largest published series and the 2023 European Society of Endocrinology / ENSAT guideline:[2]
- ~80% benign non-functioning adenomas — silent, harmless, no treatment needed.
- ~10% functioning adenomas — making cortisol, aldosterone, or catecholamines in excess.
- ~5% pheochromocytomas — medullary tumors releasing adrenaline.
- ~2-5% adrenocortical carcinoma or metastasis — the cancer fraction, almost always in masses over 4 cm.
Your odds are weighted heavily toward the benign 80%. But that does not mean you skip the workup. The whole point of finding the mass is to identify which 20% you might be in.
The Imaging Features That Change Everything
The single most useful number in your CT report is the density of the mass on non-contrast CT, measured in Hounsfield units (HU). Hounsfield units measure how much radiation a tissue absorbs — water is 0 HU, fat is around –100 HU, and most solid tissue is between 30 and 50 HU. Benign adrenal adenomas are full of lipid, so they read low on non-contrast CT.
A mass measuring less than 10 HU on non-contrast CT is nearly always a benign adenoma — the specificity is around 98%.[3] If your report mentions “lipid-rich adenoma” or “HU < 10,” your urologist will visibly relax. If it does not include a non-contrast measurement, ask for one. A contrast-only CT cannot make this distinction reliably.
The other imaging features I look for in a radiology report:
- Size. Under 4 cm is reassuring. Over 4 cm raises the cancer risk meaningfully — about 6% of masses 4-6 cm and 25% of masses over 6 cm are carcinoma.[2]
- Border. A smooth, round, well-circumscribed mass favors adenoma. Irregular margins favor malignancy.
- Homogeneity. Uniform internal texture favors benign. Necrosis, calcifications, or heterogeneous patches raise suspicion.
- Washout. If you’ve had a contrast CT, the radiologist can calculate absolute washout: how quickly contrast leaves the mass. Over 60% absolute washout (or over 40% relative washout) means adenoma. Slow washout means it could be a pheochromocytoma, carcinoma, or metastasis.
- Growth. A stable size over 12 months strongly favors benign. Growth of more than 0.5 cm in a year is a red flag.
If the non-contrast CT is equivocal — say 12 or 15 HU — the next step is usually an adrenal MRI with chemical shift imaging, which detects intracellular lipid that CT can miss. Adrenal MRI is the most accurate test we have short of histology.
In My Practice
The most common pattern I see in clinic is a man in his fifties referred because a CT done for a possible kidney stone mentioned a 1.5 cm right adrenal nodule. He arrives convinced he has cancer and has read three forum threads at 2am. I pull up the images, point to the HU value of 6, walk through the math: 80% chance benign on prevalence alone, multiplied by a 98% specific imaging feature. By the end of the visit he understands why I am going to spend the rest of our time on the hormone tests, not the mass itself.
The lesion is rarely the threat — what the lesion is doing hormonally is.
The Three Hormone Tests You Actually Need
Every adrenal incidentaloma — even a small, lipid-rich one that looks textbook-benign — needs a hormone workup. The reason is that “non-functioning” on imaging is not the same as “non-functioning” biochemically. Roughly 10-15% of incidentalomas that look benign on CT are quietly producing excess cortisol, and another 1-5% are pheochromocytomas hiding in plain sight.[4] Both can damage your cardiovascular system for years before they’re identified.
The three tests I order on the first visit:
1. Overnight 1 mg dexamethasone suppression test (cortisol excess)
You take 1 mg of dexamethasone (a synthetic steroid) at 11 pm and have your blood cortisol checked at 8 am the next morning. A healthy adrenal will see the dexamethasone and shut down its own cortisol production overnight — your morning level should be suppressed below 50 nmol/L (1.8 mcg/dL). If your cortisol fails to suppress, that adrenal mass is autonomous — it is making cortisol regardless of what your brain tells it to do. This is called mild autonomous cortisol secretion (MACS) and it raises your risk of hypertension, type 2 diabetes, osteoporosis, and cardiovascular events.[2]
2. Plasma free metanephrines or 24-hour urine metanephrines (pheochromocytoma)
This screens for a pheochromocytoma — a medullary tumor releasing adrenaline and noradrenaline in bursts. Symptoms classically include episodic pounding headaches, sweating, palpitations, and high blood pressure that comes in spikes, but a third of patients have no symptoms at all. Catching one before surgery matters: operating on an undiagnosed pheochromocytoma can trigger a fatal hypertensive crisis on the table. The test is the same regardless of symptoms — order it on every incidentaloma.
3. Aldosterone-to-renin ratio (primary hyperaldosteronism)
Order this only if your blood pressure is elevated or your potassium is low. Around 1-2% of incidentalomas produce excess aldosterone — Conn syndrome — and the tip-off is hypertension that resists treatment, often combined with low potassium. The screening test is the morning aldosterone-to-renin ratio (ARR), drawn while sitting upright. If positive, an endocrinologist confirms with a salt-loading test. Renal hypertension and primary aldosteronism are the two surgically correctable causes of high BP — both worth catching.
Worried what else your scan might be hiding? Get the Men’s Health Screening Checklist.
Enter your email below to receive Dr. Khalid’s complete Men’s Health Screening Checklist as a free, printable PDF — the urology-led list of which tests to ask for, by age, and which findings actually need acting on.
When the Answer Is Surgery
The surgical treatment for an adrenal mass is adrenalectomy — removing the affected adrenal gland, almost always laparoscopically through three or four small abdominal incisions. Recovery is typically 2-3 weeks. The remaining adrenal gland takes over within hours, so a man with one healthy gland needs no hormone replacement long-term.
I recommend surgery when any one of the following is true:
- The mass is functioning — cortisol-secreting, pheochromocytoma, or aldosterone-secreting — regardless of size. Hormone excess is the indication; the lesion has to go.
- The mass is larger than 4 cm, even if non-functioning and benign-appearing. The risk of underlying carcinoma climbs steeply with size, and the European guideline sets 4 cm as the surgical threshold.[2]
- The mass has suspicious imaging features — irregular borders, density > 20 HU, slow washout, growth on serial scans, or heterogeneous internal texture.
- The mass grows by more than 0.5 cm between follow-up scans.
For a pheochromocytoma, surgery is preceded by 10-14 days of alpha-blockade (typically phenoxybenzamine or doxazosin) to prevent intraoperative hypertensive crisis. This is non-negotiable — taking a man with an unblocked pheochromocytoma to theatre is one of the few situations in urology where you can kill someone in minutes.
If your workup points to surgery, ask the operating surgeon two specific things: how many adrenalectomies they perform per year (volume matters — over 20 per year is the threshold for best outcomes), and whether the case will be discussed at a multidisciplinary meeting with endocrinology before the date is booked.
What Follow-Up Looks Like When We Watch and Wait
If your mass is small (under 4 cm), looks unambiguously benign on CT (< 10 HU, smooth borders), and all three hormone tests are normal, surgery is not on the table. You go into surveillance. The 2023 European guideline simplified the follow-up considerably — earlier guidance had patients returning for scans yearly for five years, which was expensive, anxiety-provoking, and not supported by outcome data.
The current approach for a clearly benign, non-functioning incidentaloma:
- No routine repeat imaging if the mass is < 4 cm and has classic benign features on the initial scan.
- Repeat imaging at 6-12 months only if any imaging feature was equivocal at baseline.
- Repeat hormone screening at 1 year, then only if your blood pressure changes, you develop diabetes, you gain unexplained weight around the trunk, or you develop osteoporosis — any of which could point to a slowly developing cortisol excess.
- Discharge from clinic at 2-5 years if everything has remained stable.
Two practical points men ask me about in clinic. First, you do not need to change your diet, lifestyle, or exercise because of an adrenal incidentaloma — the mass is not affected by what you eat. Second, your kidney function is not at risk from the adrenal mass itself. If your creatinine is rising in parallel, that is a separate issue worth investigating on its own merits (see our guide on what high creatinine means: High Creatinine Levels: Causes and When to Worry).
If you want a more structured read on which screening tests you should already be doing at your age, our 40+ Men’s Health Checklist covers the bigger picture. And for an estimate of how worrisome a specific adrenal nodule is based on your imaging and hormone results, the Adrenal Incidentaloma Risk Stratifier puts the numbers together for you. Many adrenal incidentalomas are also picked up alongside another vascular finding, which is why your urologist will usually want to know your blood pressure history at the same time — the BP & Kidney Damage Risk tool is the quickest way to gauge whether your readings are tracking into the danger zone.
Red Flags: When to Push for a Faster Answer
Red Flags — Do Not Wait for a Routine Appointment
If you have been told you have an adrenal incidentaloma AND any of the following, contact your doctor or attend the emergency room the same day:
- Sudden severe headache with sweating, pale skin, and pounding heart — possible pheochromocytoma crisis. Call emergency services.
- Blood pressure spiking above 180/110 mmHg, especially with chest pain, severe headache, or visual changes.
- New-onset diabetes or rapid central weight gain with thin arms and legs, purple stretch marks, and easy bruising — possible Cushing syndrome.
- Persistent muscle weakness or cramps with low potassium on a blood test — possible Conn syndrome.
- An adrenal mass that has grown by more than 0.5 cm on a follow-up scan, particularly above 4 cm — pushes the conversation toward surgery.
- Unexplained weight loss, night sweats, or back pain with a known adrenal mass — must rule out adrenocortical carcinoma or metastasis.
Frequently Asked Questions
Is an adrenal incidentaloma likely to be cancer?
For the overwhelming majority of men, no. About 80% of incidentalomas are benign non-functioning adenomas, and only 2-5% are adrenocortical carcinoma or metastasis. The cancer risk is closely tied to size: under 4 cm the cancer rate is around 2%, between 4-6 cm it rises to about 6%, and over 6 cm to around 25%. A small mass with classic benign imaging features (under 10 Hounsfield units on non-contrast CT, smooth borders) is essentially never cancer. See our full Men’s Wellness Hub for context on related screening.
Do I really need hormone tests if the scan says “benign-looking”?
Yes. Around 10-15% of incidentalomas that look completely benign on CT are quietly producing excess cortisol (mild autonomous cortisol secretion), and a separate 1-5% are pheochromocytomas. Both can damage your cardiovascular system for years before becoming clinically obvious. The three first-line tests are an overnight 1 mg dexamethasone suppression test, plasma or urine metanephrines, and — only if your blood pressure is high or potassium is low — an aldosterone-to-renin ratio. Skipping the hormone workup is the single most common mistake I see.
What size of adrenal incidentaloma needs surgery?
The threshold most guidelines use is 4 cm. A non-functioning incidentaloma larger than 4 cm is generally recommended for adrenalectomy because the underlying cancer risk climbs steeply at that size. Below 4 cm, surgery depends on the hormone results and imaging features rather than size alone — a 2 cm mass that is producing cortisol or adrenaline still needs to come out. If the mass grows by more than 0.5 cm between follow-up scans, that also pushes the conversation toward surgery regardless of starting size.
How often will I need follow-up scans for an adrenal incidentaloma?
Far less often than older guidelines suggested. The 2023 European Society of Endocrinology guideline recommends no routine repeat imaging if your initial scan shows a small (under 4 cm), classically benign mass (less than 10 Hounsfield units on non-contrast CT, smooth borders) and all hormone tests are normal. Hormone screening is typically repeated at 1 year, then only if you develop new hypertension, diabetes, weight gain, or osteoporosis. Most men are discharged from clinic at 2-5 years if everything stays stable.
Can an adrenal incidentaloma raise my blood pressure?
Yes — and it is one of the under-recognised surgically correctable causes of resistant hypertension. The two mechanisms are excess cortisol (subclinical Cushing syndrome) and excess aldosterone (primary hyperaldosteronism / Conn syndrome). Both elevate blood pressure independently of lifestyle, and standard antihypertensive medications often fail to fully control it. If you have an adrenal mass and your BP is hard to manage, ask specifically for an aldosterone-to-renin ratio and an overnight dexamethasone test. Our guide on high blood pressure and kidney damage covers the wider picture.
What is the recovery like after adrenalectomy?
For laparoscopic adrenalectomy — the standard approach for benign and most functioning masses — you can expect 1-2 nights in hospital, 2-3 weeks off work for an office job, and 6 weeks before resuming heavy lifting or contact sport. Pain is usually well-controlled with simple analgesia after the first 48 hours. The remaining adrenal gland compensates within hours, so most men do not need long-term hormone replacement. Exceptions are cortisol-secreting adenomas, where temporary steroid tapering is needed while the suppressed opposite gland recovers — usually over 6-12 months.
References
- Bovio S, Cataldi A, Reimondo G, et al. Prevalence of adrenal incidentaloma in a contemporary computerized tomography series. J Endocrinol Invest. 2006;29(4):298-302. PubMed
- Fassnacht M, Tsagarakis S, Terzolo M, et al. European Society of Endocrinology clinical practice guideline on the management of adrenal incidentalomas, in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. 2023;189(1):G1-G42. EJE
- Boland GW, Lee MJ, Gazelle GS, et al. Characterization of adrenal masses using unenhanced CT: an analysis of the CT literature. AJR Am J Roentgenol. 1998;171(1):201-204. PubMed
- Sherlock M, Scarsbrook A, Abbas A, et al. Adrenal incidentaloma. Endocr Rev. 2020;41(6):775-820. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.