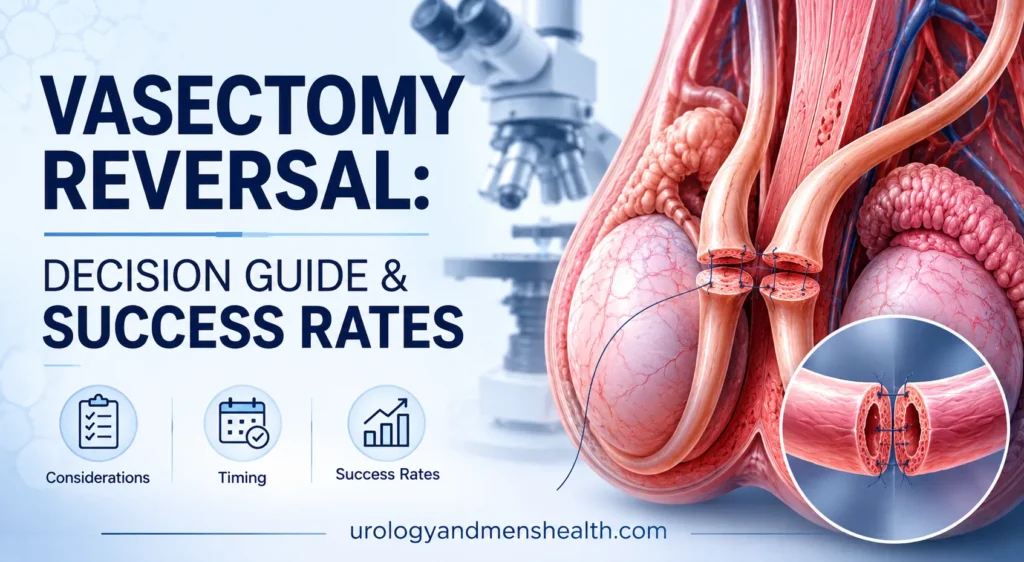
Vasectomy Reversal: Decision Guide & Success Rates
Every week a man asks me whether a vasectomy reversal will actually work — and the honest answer depends less on the surgery and more on how many years have passed. Here is how I walk patients through the decision.

A vasectomy reversal is one of the most rewarding operations I perform — and one of the most misunderstood. Men walk in expecting a quick fix and walk out with a far better understanding of why the answer depends on years, anatomy, and their partner’s fertility as much as on the surgery itself. Some are ideal candidates; others would be far better served by sperm retrieval and IVF. The decision is rarely about whether reversal can work — it almost always can, technically — and almost always about whether it is the best path to a baby for this couple, in this year, at this cost. For the wider topic, see our full Sexual Health Hub. This guide gives you the honest framework I use in clinic.
Key Takeaways
- Vasectomy reversal patency rates remain above 90% when performed within 3 years of the vasectomy, but fall to roughly 70% beyond 15 years.
- Pregnancy rates lag patency rates by 20-30 percentage points because the partner’s age and fertility matter as much as the surgery.
- Vasoepididymostomy is technically harder than vasovasostomy and is needed in 20-40% of reversals more than 10 years out — choose a microsurgeon who performs both.
- Sperm retrieval plus IVF is the better choice when the female partner is over 38, has a tubal or ovulatory factor, or when more than 20 years have passed since the vasectomy.
What a Vasectomy Reversal Actually Does
A vasectomy cuts and seals the vas deferens — the muscular tube that carries sperm from each testicle to the ejaculatory ducts. A reversal reopens that pipeline by surgically rejoining the two cut ends under an operating microscope, restoring continuity so sperm can once again reach the ejaculate.
There are two operations under the same umbrella term, and the distinction matters more than most patients realize.
Vasovasostomy: rejoining vas to vas
This is the standard reversal. The surgeon trims back the scarred ends of the vas deferens until healthy tissue is visible under the microscope, then sutures them together in two layers — an inner mucosal layer and an outer muscular layer — using sutures finer than a human hair. A well-performed two-layer vasovasostomy takes 2-4 hours in skilled hands.
Vasoepididymostomy: rejoining vas to epididymis
Sometimes the pressure built up behind the vasectomy site over the years causes a blowout — a rupture in the delicate tubules of the epididymis (the coiled storage organ behind the testicle). When that happens, simply rejoining the vas to itself is pointless because sperm cannot get past the blockage upstream. The surgeon must instead connect the vas deferens directly to a tubule within the epididymis. This is technically much harder, takes longer, and has lower success rates — but skipping it when it is needed guarantees failure.
The decision between vasovasostomy and vasoepididymostomy is made during the operation, not before, based on what the surgeon sees when fluid is examined from the testicular end of the vas. If the fluid contains sperm, vasovasostomy works. If it is thick, pasty, and sperm-free, vasoepididymostomy is required on that side. This is why choosing a microsurgeon who can perform both procedures — not just vasovasostomy — is the single most important decision you will make. If you are still researching the original vasectomy, the anatomy explanation there will help you visualize what the reversal is undoing.
Vasectomy Reversal Success Rates: What the Numbers Actually Mean
Two numbers matter, and most patients confuse them. Patency is whether sperm reappears in the ejaculate after surgery. Pregnancy rate is whether a couple actually conceives. Patency is a surgeon outcome; pregnancy is a couple outcome — and the second number is always lower because it depends on the partner’s fertility, the couple’s frequency of intercourse, and time.
The largest single dataset remains the Vasovasostomy Study Group’s analysis of 1,469 procedures [1]. The pattern it established has been confirmed by every subsequent series. Time since vasectomy is the dominant variable.
- Less than 3 years since vasectomy: patency around 97%, pregnancy around 76%.
- 3 to 8 years: patency around 88%, pregnancy around 53%.
- 9 to 14 years: patency around 79%, pregnancy around 44%.
- 15 years or more: patency around 71%, pregnancy around 30%.
Newer microsurgical series report somewhat better numbers in expert hands, particularly for vasovasostomy performed within the first decade, but the time-dependent pattern holds. The American Urological Association’s 2024 vasectomy guideline acknowledges this gradient explicitly when counseling reversal candidates [2]. The reason is mechanical: the longer the vas has been obstructed, the more pressure builds in the epididymis, and the higher the chance of a blowout that forces a vasoepididymostomy. Vasoepididymostomy patency rates run 60-85%; pregnancy rates trail at 30-45%.
In My Practice
One of the most consistent patterns I see is the man in his early forties who had a vasectomy in his late twenties after a first marriage. He remarries, his new partner is in her mid-thirties, and he comes in expecting the same 95% success rate his friend got after a reversal at year five. I have to walk him through the actual data — that at 14 years out his patency will be closer to 80%, and his pregnancy rate closer to 40%, and that his partner’s age is now the rate-limiting factor.
The honest framing — surgery numbers plus partner fertility plus time — is what lets couples make a decision they will not regret, regardless of which path they choose.
Reversal vs. Sperm Retrieval and IVF: The Real Comparison
For couples whose only fertility problem is the vasectomy, there are two legitimate paths. Reversal restores natural conception over months or years. Sperm retrieval — usually TESE (testicular sperm extraction) or PESA (percutaneous epididymal sperm aspiration) — bypasses the vasectomy entirely and feeds sperm directly into an IVF cycle with intracytoplasmic sperm injection (ICSI).
Reversal usually wins on three counts: it is a one-time intervention; the couple can try repeatedly for natural pregnancy over 1-2 years; and once patent, it stays patent in roughly 90% of cases for at least 5 years. IVF wins on speed — a baby in 9-12 months from decision rather than 2-3 years — and on independence from time since vasectomy.
The decision pivots on the female partner’s age and fertility. A 2014 meta-analysis comparing reversal and IVF outcomes found that for women under 35 with no fertility issues, reversal produced higher cumulative live-birth rates per couple, while for women over 38, IVF outperformed reversal in time-to-pregnancy [3]. When male infertility from other causes is also suspected, IVF with ICSI becomes more attractive because it sidesteps multiple barriers in one cycle.
Cost matters too. Reversal is a single out-of-pocket charge in most US markets. IVF with ICSI runs per cycle and most couples need 1-3 cycles. The math flips based on insurance, state mandates, and how many children the couple wants. Two or more desired children almost always favors reversal economically; one child with a partner approaching 40 almost always favors IVF.
Thinking about reversal? Get my full ED & Fertility framework first.
Enter your email below to receive Dr. Khalid’s complete Evidence-Based ED Action Plan as a free, printable PDF. It covers the vascular, hormonal, and post-surgical fertility checks every man over 35 should run before a reversal decision.
What to Expect: Recovery Week-by-Week
A vasectomy reversal is outpatient surgery, typically 2-4 hours, performed under general anesthesia or a deep regional block. You go home the same day in a snug scrotal supporter with ice packs ready.
Days 0-7: protect the anastomosis
The microsurgical join is fragile for the first week. Strict rules apply: scrotal support 24 hours a day for 7 days, ice 20 minutes on and 20 minutes off for the first 48 hours, no lifting more than 5 kg (about 10 lb), no sex, no ejaculation. Pain peaks at 48-72 hours then drops sharply. Most men take 3-5 days off work for a desk job, longer for physical work.
Weeks 2-3: gradual return to normal
Light walking, desk work, and driving are usually fine by day 10. No running, cycling, gym, or heavy lifting yet. Bruising along the scrotum is normal and may track down into the groin — alarming-looking but harmless.
Week 4 onward: resume sex and exercise
At 4 weeks I clear most patients for sexual activity, light exercise, and a return to all normal daily life. Heavy weight training and high-impact sport wait until 6 weeks.
Month 3 and beyond: semen analyses
The first semen analysis goes at 3 months post-op. Some men have sperm in the ejaculate by then; others take 6-12 months for sperm counts to climb. After vasoepididymostomy it can take longer still. We repeat the test every 3 months until counts stabilize or the surgery is declared a failure (usually at 12-18 months). A formal semen analysis interpreter helps you make sense of the numbers when they come back — concentration, motility, and morphology each tell a different part of the recovery story.
When Reversal Is the Wrong Choice
I turn down reversal candidates more often than people expect. The technical operation may be possible, but the clinical math points the wrong way. Four scenarios change my recommendation toward sperm retrieval plus IVF.
- Female partner over 38 with reduced ovarian reserve. Even with a 90% patency rate, a 24-month window to conceive naturally may not be there. IVF gets the cycle running within months.
- Confirmed tubal factor or severe endometriosis in the partner. Restoring his sperm into ejaculate does not solve the bottleneck. IVF bypasses both his vasectomy and her tubes.
- High levels of anti-sperm antibodies. Roughly 60% of men develop anti-sperm antibodies after vasectomy. Most still conceive after reversal, but very high titers correlate with reduced fertilization rates even with sperm in the ejaculate [4]. IVF with ICSI sidesteps the issue.
- Vasectomy more than 20 years old. The probability of bilateral epididymal blowout climbs sharply, vasoepididymostomy becomes likely, and pregnancy rates drop into the 25-30% range. Many couples in this group are better served by upfront sperm retrieval.
Other men I redirect entirely. If you are weighing this purely on statistics, run your specific numbers (years since vasectomy, partner’s age, partner’s AMH if available) before booking surgery. The decision should match the data, not the hope.
Pre-Operative Workup: What I Order Before Saying Yes
A reversal consultation is not a green light. Before I commit a man to surgery, I want a complete clinical picture. The workup is short but specific.
- Detailed history. Date of vasectomy. Any post-vasectomy complications, sperm granuloma, or chronic pain. Children fathered before vasectomy. Any prior fertility issues in the relationship before vasectomy.
- Physical examination. I palpate both vas deferens through the scrotal skin, looking for the gap from the vasectomy site. I check for sperm granulomas (a small lump where sperm has leaked — often a good sign that the testicular end of the vas remained patent and pressure was relieved). I examine the testicles for size, consistency, and any varicocele.
- Hormonal screen. Total testosterone, LH, and FSH. Elevated FSH suggests primary testicular failure, which would reduce success regardless of plumbing. If symptoms of low testosterone are present, I also use the low testosterone symptom quiz as a structured starting point — and if results are equivocal, I read them alongside our full guide to low testosterone in men over 40.
- Partner fertility workup. Non-negotiable. Age, menstrual regularity, AMH, day-3 FSH, and a pelvic ultrasound. Without this, reversal counseling is incomplete.
- Anti-sperm antibody testing. Optional but useful in men whose vasectomy is 10+ years old, particularly if reversal would be costly or if IVF is also on the table.
For men also considering ED treatment or screening at this life stage, the IIEF-5 erectile function assessment takes two minutes and flags whether erectile function needs attention before fertility treatment begins. I also run men in their forties through a basic midlife check — see our 40+ men’s health checklist for the full screening list. Treating ED alongside reversal recovery is straightforward; ignoring it until after the first failed conception attempt is harder.
When to See a Urologist
Most men contemplating a reversal are not in any medical urgency — the timeline is set by the couple’s family planning, not by symptoms. But certain post-vasectomy presentations need a urologist sooner rather than later.
Red Flags After Vasectomy
Book a urology appointment within 2 weeks if any of these apply, and go to the ER if you have fever with scrotal pain:
- Persistent scrotal pain more than 3 months after vasectomy (post-vasectomy pain syndrome — affects 1-2% of men and may influence the reversal decision).
- A painful or growing lump at the vasectomy site (sperm granuloma — usually benign, occasionally needs excision).
- Sudden scrotal swelling, redness, or fever (possible infection or epididymitis — emergency).
- Erectile dysfunction or libido change developing after vasectomy (almost never caused by the vasectomy itself but may unmask a separate vascular or hormonal issue — request testosterone, lipids, and a vascular ED assessment).
For the reversal decision itself, see a urologist who performs at least 25-50 microsurgical reversals a year and who is comfortable with vasoepididymostomy. Volume correlates strongly with patency rates in published series. Ask the surgeon directly: “What percentage of your reversals end up needing vasoepididymostomy on at least one side, and what are your patency rates for each procedure?” A surgeon who cannot answer that question with specific numbers is the wrong surgeon.
Frequently Asked Questions
How long after a vasectomy can you still have a successful vasectomy reversal?
Technically a reversal can be attempted at any interval — I have performed them more than 25 years after vasectomy. The question is not whether the surgery is possible but whether it is the best path. Patency stays above 70% even beyond 15 years in microsurgical series, but pregnancy rates fall below 35% and the probability of needing vasoepididymostomy on at least one side rises sharply. Beyond 20 years, sperm retrieval plus IVF is often the more efficient route.
Does insurance cover vasectomy reversal in the US?
Almost never. Vasectomy reversal is classified as an elective fertility procedure by most US private insurers and is excluded from coverage. A handful of state-mandated infertility insurance laws may apply to IVF but rarely to reversal. Plan for out-of-pocket payment. Some surgeons offer payment plans or package pricing that includes the operating room, anesthesia, and follow-up semen analyses — ask for an all-in quote rather than a surgeon’s fee alone.
Can a vasectomy reversal affect testosterone or libido?
No. The vas deferens carries sperm; it does not carry testosterone. Testosterone is produced by Leydig cells in the testicle and travels in the bloodstream, untouched by either vasectomy or reversal. If libido or erectile function has changed since your vasectomy, the cause is almost always something else — vascular, hormonal, or psychological. I work that up separately with a testosterone panel and a vascular ED screen rather than assuming the vasectomy is to blame.
What is the chance the reversal will fail and I’ll need a redo?
Roughly 5-15% of vasovasostomies and 15-30% of vasoepididymostomies fail to produce sperm in the ejaculate or have sperm initially that disappears within 12 months (so-called late failure or secondary obstruction). A repeat reversal is technically possible but success rates drop with each attempt. If the first reversal fails, most couples switch to sperm retrieval with IVF rather than attempting a second reversal — the math is usually cleaner that way.
Should I freeze sperm at the time of the reversal?
I offer this to every couple where the female partner is over 35 or where the vasectomy is more than 10 years old. During the operation, sperm aspirated from the testicular end of the vas can be cryopreserved as backup. If the reversal succeeds, the frozen sperm is unused. If it fails, you have material ready for IVF without a second procedure. The added cost is small relative to the IVF cycle it spares. Discuss this explicitly with your surgeon before the day of surgery.
How soon after vasectomy reversal can we start trying for a baby?
Sexual activity is usually cleared at 4 weeks post-op. But sperm does not return to the ejaculate immediately. The first semen analysis is at 3 months, and many men show low counts at that point that gradually improve over 6-12 months. Some couples conceive within the first 6 months; others take 18-24 months. If no pregnancy by 12-18 months despite adequate sperm counts, additional fertility workup of the partner is warranted before declaring the reversal a failure.
References
- Belker AM, Thomas AJ Jr, Fuchs EF, Konnak JW, Sharlip ID. Results of 1,469 microsurgical vasectomy reversals by the Vasovasostomy Study Group. J Urol. 1991;145(3):505-511. PubMed
- American Urological Association. Vasectomy: AUA Guideline (2024 Amendment). AUA Guidelines. 2024. AUA
- Herrel LA, Goodman M, Goldstein M, Hsiao W. Outcomes of microsurgical vasovasostomy for vasectomy reversal: a meta-analysis and systematic review. Urology. 2015;85(4):819-825. PubMed
- Patel AP, Smith RP. Vasectomy reversal: a clinical update. Asian J Androl. 2016;18(3):365-371. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.