Phimosis and Paraphimosis in Adults: Causes & Treatment
The hardest part of treating phimosis and paraphimosis is knowing which one you have — one is a slow problem you manage over weeks, the other is a clock-ticking emergency. Here's how a urologist tells them apart and treats each.

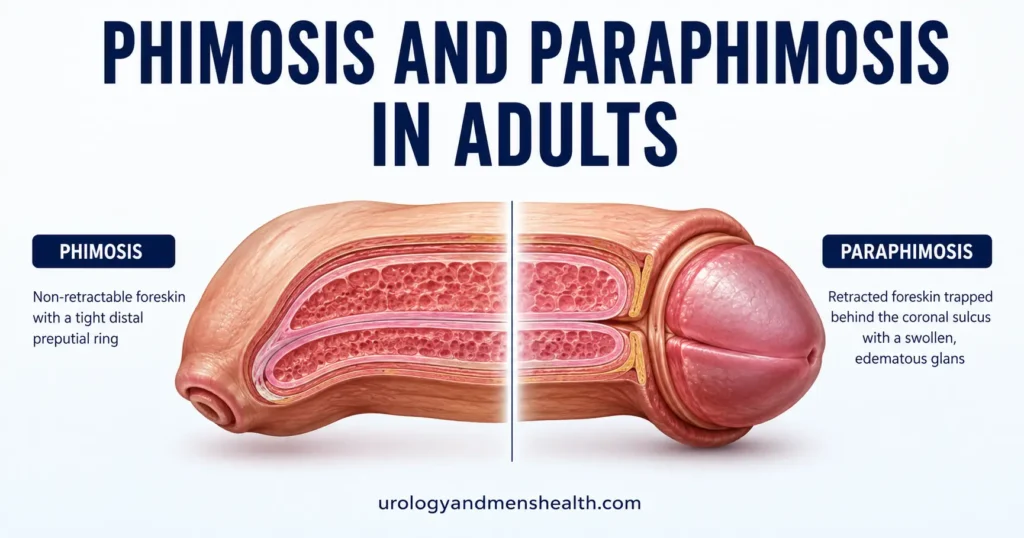
Phimosis and paraphimosis are two foreskin problems that get confused constantly — including, sometimes, in the emergency room. They are almost opposites. Phimosis is a foreskin that will not pull back off the head of the penis. Paraphimosis is a foreskin that has been pulled back and now will not go forward again, trapping the glans (the head) in a tightening ring. The first is usually a slow, manageable issue you can treat over weeks. The second is a genuine emergency where the trapped glans can lose its blood supply within hours. I see both in clinic, and the single most useful thing I can teach you is how to tell them apart — because the right response to one is “book an appointment,” and the right response to the other is “go to the emergency room now.” For the full picture of foreskin and penile surgery, see our Urological Surgery & Recovery hub.
Key Takeaways
- Phimosis is a non-retractable foreskin; paraphimosis is a retracted foreskin stuck behind the glans — and paraphimosis is a time-sensitive emergency.
- In adults, a foreskin that newly stops retracting is not “just tight” — it usually means scarring, infection, or a skin condition called BXO that needs a doctor.
- Topical steroid cream plus gentle daily stretching resolves most non-scarred adult phimosis, with reported success rates of roughly 65–95% across trials, avoiding surgery.
- Circumcision is the definitive fix when steroids fail, when scarring (BXO) is present, or after a paraphimosis episode — and it prevents recurrence.
Phimosis vs. Paraphimosis: The Difference That Matters Most
Think of the foreskin as a sleeve. In phimosis, the cuff of that sleeve is too narrow to slide back over the head of the penis. It stays forward, covering the glans. This is often painless and may only show up as ballooning during urination, difficulty cleaning underneath, or splitting and soreness during erections.
In paraphimosis, that same narrow cuff has been pulled back behind the ridge of the glans (the coronal sulcus) and now acts like a tourniquet. Blood can flow into the glans but struggles to drain out, so the head swells, which tightens the ring further, which worsens the swelling. It is a vicious cycle, and it is painful, visibly alarming, and progressive. Left untreated, the loss of blood flow can damage the tissue of the glans.
The practical rule I give patients: if your foreskin won’t go back, that’s phimosis and it can wait for a clinic appointment. If your foreskin won’t come forward and the head is swelling, that’s paraphimosis and it cannot wait.
What Causes Phimosis in Adults?
A non-retractable foreskin is completely normal in young boys and usually resolves by around age 5 to 7 [4]. So in adults, the question is different: why has a foreskin that used to work stopped working? That change is the part that needs explaining, because adult-onset phimosis is rarely “just tightness.”
The most common drivers I see are repeated inflammation and scarring. Recurrent infection or irritation of the glans and foreskin leaves microscopic scar tissue each time, and scar tissue doesn’t stretch. A specific and important cause is balanitis xerotica obliterans (BXO) — also called lichen sclerosus — a chronic skin condition that produces a tell-tale firm, pale, whitened ring at the tip of the foreskin. BXO matters because it does not respond well to stretching and steroids alone and is the clearest reason to choose surgery early.
The other pattern worth flagging is new phimosis in a man over 50, or in anyone with poorly controlled diabetes. High blood sugar feeds recurrent yeast infections of the glans, which drive the scarring cycle. If you have unexplained foreskin tightening alongside frequent thrush-like infections, getting your blood sugar checked is part of the workup, not a side issue.
In My Practice
The men who worry me most are not the ones with a lifelong slightly tight foreskin — they are the ones who tell me their foreskin retracted fine for forty years and then, over a few months, stopped. When I examine them and find that pale, rigid ring of BXO, I know steroid cream alone is unlikely to win, and I’d rather have the circumcision conversation early than after three failed creams. A new-onset tight foreskin in an older adult also earns a careful look at the glans itself, because long-standing phimosis is a recognized risk factor for penile cancer.
Adult-onset phimosis is a symptom to investigate, not a nuisance to ignore — the cause changes the treatment.
Preparing for urological surgery? Download Dr. Khalid’s Urology Surgery Recovery Guide.
Enter your email below to receive Dr. Khalid’s complete Urology Surgery Recovery Guide as a free, printable PDF.
Treatment Options for Phimosis: From Cream to Surgery
Treatment climbs a ladder, and most men never need to reach the top rung. The European Association of Urology recommends topical corticosteroid cream as the first-line treatment for symptomatic phimosis, with a strong rating [1].
Step 1: Topical steroid cream plus stretching
The standard regimen is a moderate-to-high potency steroid cream (for example 0.05% betamethasone or 0.1% triamcinolone) applied to the tight ring once or twice daily for 4 to 8 weeks, combined with gentle daily retraction once the skin softens. The steroid thins and loosens the constricting band; the stretching does the mechanical work. Across randomized trials, reported success rates run from roughly 65% to over 90%, and a 2024 network meta-analysis of 17 trials confirmed that low, moderate, and high potency steroids all significantly outperform placebo [2][3]. What to do: ask your primary care doctor or urologist for a prescription steroid cream and a clear 6-to-8-week plan, and book a review at the end to decide whether it worked.
Step 2: Preputioplasty (foreskin-sparing surgery)
If cream fails but you want to keep your foreskin, preputioplasty is a small operation that widens the tight ring with one or more limited cuts, without removing the foreskin. It is a reasonable middle option for men with a localized tight band and no significant scarring, though it is not suitable when BXO is present.
Step 3: Circumcision (the definitive fix)
Circumcision removes the foreskin entirely and is the definitive treatment when steroids fail, when BXO scarring is confirmed, or after recurrent paraphimosis. It is the one option that essentially eliminates recurrence. If you want to understand exactly when surgery is the right call and what recovery involves, our guide to the medical reasons adults undergo circumcision walks through it, and you can compare procedures side by side with our urology surgery comparison tool.
Paraphimosis Is a Medical Emergency: What to Do
Paraphimosis most often happens when a foreskin is retracted and then forgotten — classically after a catheter is placed, during a medical exam, or after sex or washing — and never pulled forward again. The trapped ring strangles the glans, swelling builds, and the window to fix it easily closes by the hour [5].
The treatment is reduction: firm, steady, circumferential squeezing of the swollen glans for several minutes to push fluid out, then easing the foreskin back forward over the head. In a clinical setting we use a local anesthetic block, cold compression, or osmotic agents like a dextrose-soaked dressing to shrink the swelling first. If manual reduction fails, a small dorsal slit releases the ring, and circumcision is usually recommended afterward to stop it recurring [5].
This is not something to manage with online instructions while the clock runs. If you cannot pull a retracted foreskin forward and the head is swelling or darkening, treat it the way you would any condition cutting off blood supply — and note that a single paraphimosis episode is itself a recognized warning sign worth a full check of your overall penile health.
When to Go to the ER Immediately
Paraphimosis is time-critical. Go to the emergency room without delay if you have a retracted foreskin that will not move forward and any of the following:
- The head of the penis is swelling, throbbing, or increasingly painful.
- The glans is turning dark red, blue, or pale — a sign blood flow is compromised.
- You cannot reduce the foreskin yourself within a few minutes of firm compression.
- The episode followed a catheter placement and the foreskin was never returned to position.
When to See a Doctor About a Tight Foreskin
Book a non-urgent appointment with your primary care doctor or a urologist if a foreskin that previously retracted has become tight over weeks or months, if you get recurrent infections under the foreskin, if you see a pale or whitened firm ring at the tip, or if tightness is causing pain or splitting during erections. Ask specifically whether BXO is likely, whether a prescription steroid trial is appropriate, and whether your blood sugar should be checked. If you also have other lower-urinary symptoms, our broader look at what’s normal and what needs review and the site’s symptom checker can help you frame the conversation.
Frequently Asked Questions
What is the difference between phimosis and paraphimosis?
Phimosis and paraphimosis are near-opposites. Phimosis is a foreskin that cannot be pulled back off the head of the penis; it is usually non-urgent. Paraphimosis is a foreskin that has been retracted and is now trapped behind the head, acting as a tourniquet and causing swelling — that is a medical emergency. If the head is swelling and the foreskin won’t come forward, seek urgent care immediately.
Can adult phimosis be treated without circumcision?
Often, yes. For phimosis without significant scarring, a moderate-to-high potency steroid cream applied for 4–8 weeks with gentle daily stretching resolves the majority of cases, with trial success rates reported between roughly 65% and 95%. Circumcision becomes the definitive answer only when creams fail, when BXO scarring is present, or after paraphimosis. You can weigh the surgical routes using our surgery comparison tool.
Why did my foreskin suddenly become tight as an adult?
A foreskin that used to retract and then stops usually points to scarring from repeated inflammation, a skin condition called balanitis xerotica obliterans (BXO), or recurrent infections linked to poorly controlled diabetes. New-onset adult phimosis should be examined rather than ignored, partly because long-standing tightness is a recognized risk factor for penile cancer. Ask your doctor whether BXO is likely and whether your blood sugar needs checking.
Is paraphimosis dangerous if I wait a few hours?
Yes. Paraphimosis cuts off venous drainage from the head of the penis, so swelling worsens by the hour and prolonged constriction can damage the tissue. It is treated by manually reducing the foreskin, often after shrinking the swelling with compression or a dexterous block; if that fails, a minor surgical release is needed. Do not wait it out — go to the emergency room.
Will circumcision fix paraphimosis permanently?
Circumcision removes the foreskin entirely, so once it heals, paraphimosis cannot recur because there is no longer a foreskin to become trapped. That is why urologists usually recommend planned circumcision after a paraphimosis episode, especially a recurrent one. Recovery and indications are covered in our guide to adult circumcision for medical reasons.
References
- European Association of Urology. EAU Guidelines on Paediatric Urology. EAU Guidelines Office. 2023. EAU
- Lygas A, Joshi H. An evaluation of the pharmacotherapeutic options for the treatment of adult phimosis: a systematic review of the evidence. Expert Opin Pharmacother. 2022;23(9):1115-1122. PubMed
- Sridharan K, Sivaramakrishnan G. Effectiveness of low to moderate potency topical corticosteroids for phimosis: a network meta-analysis of randomized clinical trials. Int Urol Nephrol. 2024. PubMed
- Merck Manual Professional Edition. Phimosis and Paraphimosis. Merck Manuals. 2025. Merck Manual
- Bragg BN, Kong EL, Leslie SW. Paraphimosis. StatPearls. NCBI Bookshelf. 2023. NIH
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.