Varicocele in Adults: When to Treat (Urologist Guide)
When a man finds a "bag of worms" in his scrotum or gets one flagged on an ultrasound, the real question isn't what it is — it's whether to leave it alone. Here's the framework I use to decide which adult varicoceles get treated and which don't.

A varicocele in adults is a tangle of dilated veins above the testicle, and the question I’m asked most about it isn’t what is it — it’s do I have to do anything about it. Most of the time the honest answer is no. About 15% of adult men have a varicocele and the majority never need treatment. But there are four specific clinical situations where leaving one alone is the wrong call: persistent scrotal pain, shrinking testicle, abnormal semen parameters when you’re trying to conceive, and symptomatic low testosterone. This guide walks through how I decide, drawing on AUA and EAU guidance and patterns I see weekly in clinic. For the wider context on male reproductive anatomy and conditions, see the full Sexual Health Hub.
Key Takeaways
- Roughly 15% of adult men have a varicocele; most are left-sided and most never need treatment.
- Treatment is indicated for persistent pain, documented testicular atrophy, abnormal semen analysis in a man trying to conceive, or symptomatic hypogonadism with a clinical varicocele.
- Microsurgical subinguinal varicocelectomy has the lowest recurrence (1-2%) and complication rate — it’s the gold standard for most adults.
- A new right-sided varicocele in an adult, or one that does not decompress when lying flat, is a red flag for retroperitoneal pathology and needs urgent imaging.
What a Varicocele Actually Is
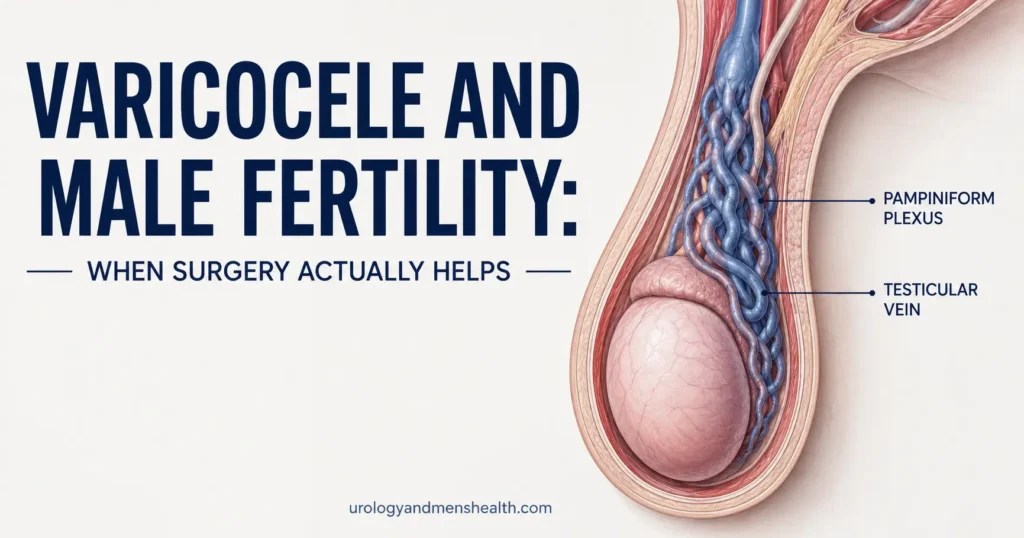
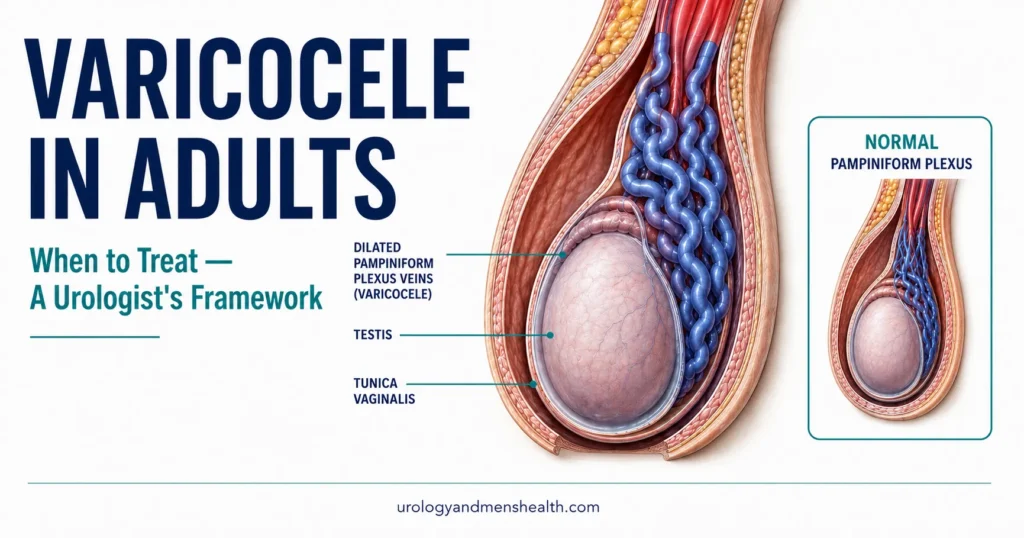
A varicocele is varicose veins of the scrotum. The drainage system for each testicle is a small network called the pampiniform plexus — think of it as a sponge of thin veins that wraps around the testicular artery and helps cool the blood before it reaches the testis. When the one-way valves inside the testicular vein fail, blood pools backward into that plexus and the veins balloon out. The result is what most patients describe as a “bag of worms” they can feel sitting above the testicle, usually worse when standing and softer when lying down.
About 85-90% of varicoceles are on the left side. The reason is plumbing, not coincidence: the left testicular vein drains into the left renal vein at a right angle, against gravity, while the right testicular vein drains more directly into the inferior vena cava. That extra column of pressure on the left is enough to break the valves over time. A purely right-sided varicocele in an adult is genuinely unusual and changes the workup — I cover why later under red flags.
The condition is common. Population estimates put prevalence at around 15% of all adult men, rising to roughly 35-40% of men evaluated for primary infertility and up to 80% of men with secondary infertility[1]. Most are picked up either because the patient noticed a swelling, a partner did, or because a scrotal ultrasound ordered for another reason flagged it. The presence of a varicocele alone is not a diagnosis that requires treatment — what surrounds it does.
How Do You Know You Have One?
Most adult varicoceles are diagnosed in clinic, not by imaging. I examine the patient standing in a warm room — cold or supine positioning collapses the veins and can hide the diagnosis. The classic finding is a soft, compressible mass above the testicle that feels like a bundle of cooked spaghetti or a small bag of worms. I then ask the patient to perform a Valsalva maneuver (bear down as if straining): a varicocele will engorge visibly under your fingers.
From there, varicoceles get a clinical grade — and this grade matters because it predicts which ones cause measurable trouble:
- Subclinical: not visible, not palpable, only seen on scrotal ultrasound (typically vein diameter >2.5-3 mm with reflux on Valsalva). These are usually incidental findings and almost never need treatment in isolation.
- Grade 1: palpable only with Valsalva. You can’t see it through the skin; you can only feel it when the patient bears down.
- Grade 2: palpable at rest without Valsalva, but still not visible. The veins are clearly there when you examine the patient standing.
- Grade 3: visible through the scrotal skin without palpation. The “bag of worms” appearance is obvious on inspection.
Higher grade correlates with higher likelihood of impacting semen parameters and testicular size. Grade 3 varicoceles are the ones most consistently linked to atrophy and abnormal semen analysis in studies[2]. Subclinical varicoceles, by contrast, have not been convincingly shown to benefit from treatment in randomized trials, which is why ultrasound-only findings rarely get operated on.
If the exam is equivocal, or if I’m planning treatment, I order a scrotal Doppler ultrasound. It confirms vein diameter, documents reflux during Valsalva, and gives me a baseline testicular volume on each side. Testicular volume is the single most useful number in this whole conversation — a difference of more than 20% between the two sides is the threshold for documented atrophy.
In My Practice
A 28-year-old came in last year worried he had testicular cancer. His wife had felt “something weird” during sex. On exam, standing, I could see a clear grade 3 left varicocele the moment he dropped his shorts — the bag-of-worms look, soft, compressible, completely gone when he lay down. He had no pain, no infertility plans yet, testes were equal in size on ultrasound. We did nothing. He still sends me a Christmas card.
A varicocele you can see across the room is alarming to a patient — but how it looks tells you almost nothing about whether it needs treating.
When a Varicocele Actually Needs Treatment
This is the only section of this article that really matters. AUA 2024 guidance and EAU 2024 sexual and reproductive health guidelines converge on four indications for treating a varicocele in adults[3][4]. If you don’t fall into one of these buckets, observation is the right answer.
1. Persistent scrotal pain that hasn’t responded to conservative measures
Varicocele pain is typically described as a dull, dragging ache on the affected side, worse at the end of the day and after standing for hours, and relieved by lying down. It is rarely sharp and never sudden — sharp, sudden testicular pain is something else (see the red flags section). I ask patients to try a structured 3-month trial first: scrotal support during the day, NSAIDs as needed (ibuprofen 400 mg up to 3 times daily with food), avoiding long stretches of standing, and elevating the scrotum when resting. If a documented varicocele is still painful enough to interfere with work or daily life after that trial, varicocelectomy reliably relieves pain in around 75-90% of properly selected patients.
2. Documented testicular atrophy on serial ultrasound
This is the indication where I’m most aggressive. If your varicocele-side testis is more than 20% smaller than the other side on ultrasound — or has shrunk on serial scans over 6-12 months — that is biological damage in progress. Adolescent and young adult data are clearest, but the principle holds in adulthood: a varicocele that’s shrinking your testis is one that’s actively impairing it, and waiting longer means losing more functional tissue. Repair stops or reverses the trend in most patients.
3. Abnormal semen analysis in a man actively trying to conceive
If you and your partner are trying for a baby, you have a clinical varicocele (grade 2-3), and at least one semen parameter is abnormal on two separate analyses, varicocele repair is on the table. Meta-analyses show varicocelectomy improves sperm concentration, motility, and morphology in this population and increases spontaneous pregnancy rates compared with observation[5]. The specific decision is best made together with a fertility specialist after a full evaluation — this article focuses on the varicocele decision, but the fertility workup is broader. The full picture is in my guide to male infertility and the fertility-specific surgical decision in Varicocele and Male Fertility. You can also screen your own results with the Semen Analysis Interpreter before the conversation.
4. Symptomatic low testosterone with a clinical varicocele
This indication is newer and worth understanding. Multiple studies now show varicocele repair can produce a meaningful rise in serum testosterone in men who have both a clinical varicocele and biochemical hypogonadism — typically a total testosterone in the 200-350 ng/dL range with symptoms[6]. The average bump is around 100 ng/dL, which is enough to move many men out of the low range and improve symptoms. This is not a guarantee, and it’s not a substitute for testosterone replacement in men with severe deficiency. But for the 35-year-old with a grade 3 varicocele, a testosterone of 280 ng/dL, and the typical low-T symptoms, repair is a legitimate first step before starting TRT. If you’re not sure whether your symptoms fit the picture, the Low Testosterone Symptom Quiz is a useful starting point before requesting bloodwork.
Worried your symptoms add up to more than just a varicocele?
Enter your email below to receive Dr. Khalid’s complete Evidence-Based ED Action Plan as a free, printable PDF — including the bloodwork to ask for, the vascular and hormonal causes most often missed, and the questions to bring to your urology appointment.
Surgical and Non-Surgical Treatment Options
If you meet one of the four indications above, you have three reasonable options. They are not equivalent.
Microsurgical subinguinal varicocelectomy (the gold standard)
A 2-3 cm (about 1 inch) incision below the inguinal canal, using an operating microscope to identify and ligate every dilated internal spermatic vein while preserving the testicular artery, vas deferens, and lymphatics. Done by an experienced microsurgical urologist, this technique has the lowest recurrence rate (1-2%), the lowest hydrocele rate (around 0.5%), and the lowest risk of testicular artery injury[7]. Operative time is around 60-90 minutes per side. Recovery is faster than older open techniques because the inguinal canal isn’t opened. This is what I recommend to nearly every patient who needs treatment.
Laparoscopic varicocelectomy
Three small abdominal port incisions, ligating the testicular vein high in the retroperitoneum. Reasonable for bilateral cases done in one sitting, but the recurrence rate runs higher (5-10%) because not all collateral veins are ligated, and the postoperative hydrocele rate is higher because lymphatics are harder to spare from that angle. General anesthesia is required. I rarely choose this over microsurgical now.
Percutaneous embolization
Performed by an interventional radiologist through a small puncture in the groin or neck vein. A catheter is threaded up to the testicular vein and the vein is blocked with coils or sclerosant. No incision in the scrotum, faster return to work (often 1-2 days), no general anesthetic. The trade-off is a technical failure rate of 5-15% (vein anatomy doesn’t always cooperate with the catheter), exposure to contrast and radiation, and the recurrence rate is higher than microsurgical repair. It is a reasonable choice for patients who want to avoid an incision, who have a recurrence after previous open surgery, or who have contraindications to general anesthesia.
There is no medication that fixes a varicocele. Supplements, herbal remedies, scrotal cooling devices, and the various online “natural cures” do not reverse venous incompetence. What conservative measures can do is reduce pain enough that surgery isn’t necessary — and for the majority of varicoceles, that’s the goal.
What Recovery Actually Looks Like
Microsurgical varicocelectomy is a same-day discharge procedure in most centers. You go home a few hours after surgery wearing a scrotal support, and most patients are off prescription pain medication within 3-4 days.
- Week 1: Scrotal support 24/7 (including sleep). Ice 20 minutes at a time for the first 48 hours. Expect a dull ache, mild scrotal bruising, and some swelling — this is normal. No lifting heavier than 5 kg (about 11 lb). Walking is encouraged.
- Week 2: Sutures are typically dissolvable. Return to a desk job is reasonable. Bruising fades. Continue scrotal support during the day; can sleep without it.
- Week 3-4: Light exercise (walking, stationary cycling, light cardio) is fine. Hold off on heavy weight training, contact sports, and sexual activity for now. First follow-up appointment for wound check and exam.
- Week 6: Cleared for full activity — gym, running, sexual activity. The varicocele itself should no longer be palpable; mild residual swelling can persist a little longer.
- Month 3: Repeat semen analysis if fertility was the indication. Sperm parameters take a full spermatogenic cycle (roughly 74 days) to reflect the change, so checking earlier doesn’t help. The Semen Analysis Interpreter is the easiest way to compare your pre-op and post-op numbers.
- Month 6: Repeat morning total testosterone if hypogonadism was the indication. Most of the rise plateaus by 6 months.
Possible complications are real but uncommon in experienced hands: postoperative hydrocele (fluid around the testis from lymphatic injury, around 0.5% microsurgical / 5-10% laparoscopic), recurrence (1-2% microsurgical), testicular artery injury (rare with microsurgical technique, theoretically can cause testicular atrophy), and wound infection (under 1%). Severe complications such as testicular loss are exceedingly rare.
When to See a Urologist About Your Varicocele
For most adult men with an asymptomatic varicocele, routine GP follow-up is enough. But certain features change that — some warrant a scheduled urology appointment, and a few warrant urgent evaluation. If you’re a younger man in your 20s or 30s with new scrotal symptoms, the broader question of when to see a urologist as a young man is worth a read.
Red Flags — Get Seen Urgently
Some scrotal findings are not “just a varicocele” and need same-day or same-week evaluation:
- A right-sided varicocele only, especially new in adulthood — this can signal a retroperitoneal mass (including renal tumor) obstructing the right testicular vein. Needs an abdominal CT or ultrasound.
- A varicocele that does not decompress when you lie flat — competent varicoceles soften when you lie down. One that stays engorged supine raises concern for venous obstruction higher up.
- Sudden onset of a “varicocele” in an adult who never had one — particularly over age 40 — needs imaging to rule out renal vein thrombus or mass.
- Sudden severe testicular pain, with or without a visible varicocele — this is not varicocele pain. Suspect testicular torsion if under 25, or epididymitis at any age. Go to the emergency room.
- A hard, painless lump that does not change with position — that’s not a varicocele. Get it imaged urgently to rule out testicular cancer.
Beyond the red flags, see a urologist on a scheduled basis if you have a known varicocele plus any of the following: persistent scrotal ache for more than 3 months despite scrotal support, a noticeable size difference between your testicles, semen analysis abnormalities while trying to conceive, or symptomatic low testosterone confirmed on morning bloodwork. When you book the appointment, ask specifically for a urologist who performs microsurgical varicocelectomy — not all urologists do, and outcomes are technique-dependent.
Frequently Asked Questions
Can a varicocele in adults go away on its own?
No. Once the valves in the testicular vein have failed, the dilated pampiniform plexus stays dilated. A varicocele can look smaller when you lie down because the veins partially decompress, and aggressive weight loss can make a previously invisible grade 2 varicocele easier to see — but the venous incompetence itself does not resolve spontaneously in adults. Treatment is the only durable fix, and the question is whether you need treatment at all. Most men with an asymptomatic varicocele in adults do not. See the Sexual Health Hub for related conditions worth understanding.
Does a varicocele always lower testosterone?
No. Plenty of men with grade 3 varicoceles have completely normal testosterone. The connection is statistical: as a group, men with clinical varicoceles tend to have slightly lower testosterone than men without, and repair produces an average rise of about 100 ng/dL in men who start out low. If your testosterone is normal and you’re not symptomatic, your varicocele isn’t lowering your testosterone in any meaningful way. The Low Testosterone Symptom Quiz can help you decide whether morning bloodwork is worth ordering.
Will varicocele surgery improve my fertility?
For men with a clinical (grade 2 or 3) varicocele and abnormal semen parameters who are actively trying to conceive, yes — meta-analyses show varicocelectomy improves sperm concentration, motility, and morphology, and increases natural pregnancy rates compared with observation. For men with normal semen analysis, surgery does not improve fertility because there is nothing to improve. Subclinical varicoceles also do not benefit from treatment for fertility. The full fertility workup is covered in my male infertility guide.
How long after varicocelectomy can I have sex again?
Six weeks is the standard answer for full clearance after microsurgical varicocelectomy. The wound is healed at that point, scrotal swelling has resolved in most men, and the testicular blood supply has stabilized. Earlier than that and you risk wound discomfort, bleeding into the scrotum, or simply pain that ruins the experience. If you had a percutaneous embolization with no incision, return to sexual activity is usually safe at 1-2 weeks. Always confirm with the surgeon who did your procedure.
Is a varicocele dangerous if I leave it alone?
For most adult men, no. An asymptomatic varicocele that isn’t shrinking your testicle, isn’t dropping your testosterone, and isn’t affecting your fertility plans is not a dangerous condition — it’s an anatomic finding. The exceptions are the red flag presentations above: a new right-sided varicocele in adulthood, a varicocele that doesn’t decompress lying down, or a sudden new varicocele over age 40 — these need imaging to rule out a retroperitoneal cause. A long-standing, well-characterised left-sided varicocele in a man with no symptoms and equal testicular sizes is not an emergency and rarely becomes one.
Will my varicocele come back after surgery?
Recurrence depends heavily on technique. Microsurgical subinguinal varicocelectomy by an experienced surgeon recurs in about 1-2% of cases. Laparoscopic varicocelectomy recurs in 5-10%. Percutaneous embolization fails technically in 5-15% upfront and recurs in another small percentage afterward. If recurrence happens, repair is still possible — embolization is often a good option after a failed open procedure because it approaches the vein from a different direction. This is one reason microsurgery is worth the small extra effort to find a surgeon who does it routinely.
References
- Alsaikhan B, Alrabeeah K, Delouya G, Zini A. Epidemiology of varicocele. Asian Journal of Andrology. 2016;18(2):179-181. PubMed
- Damsgaard J, Joensen UN, Carlsen E, et al. Varicocele is associated with impaired semen quality and reproductive hormone levels: a study of 7035 healthy young men. European Urology. 2016;70(6):1019-1029. PubMed
- American Urological Association / American Society for Reproductive Medicine. Diagnosis and Treatment of Infertility in Men: AUA/ASRM Guideline (2020, amended 2024). AUA Guidelines
- European Association of Urology. EAU Guidelines on Sexual and Reproductive Health 2024 — Male Infertility (varicocele section). EAU Guidelines
- Persad E, O’Loughlin CA, Kaur S, et al. Surgical or radiological treatment for varicoceles in subfertile men. Cochrane Database of Systematic Reviews. 2021;4:CD000479. PubMed
- Li F, Yue H, Yamaguchi K, et al. Effect of surgical repair on testosterone production in infertile men with varicocele: a meta-analysis. International Journal of Urology. 2012;19(2):149-154. PubMed
- Cayan S, Shavakhabov S, Kadioglu A. Treatment of palpable varicocele in infertile men: a meta-analysis to define the best technique. Journal of Andrology. 2009;30(1):33-40. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.