Andropause vs Late-Onset Hypogonadism: Real or Hype?
Men keep asking me if "male menopause" is real, and the honest answer is more complicated than yes or no. Andropause is a marketing term — late-onset hypogonadism is a measurable medical diagnosis, and only one of them earns treatment.

“Doc, do I have andropause?” I get asked this in clinic at least twice a week, and the honest answer is more nuanced than most men want to hear. Andropause vs late-onset hypogonadism is not just a semantic argument — it’s the difference between a marketing term used to sell testosterone gels and a real medical diagnosis with strict biochemical criteria. One of them describes a fuzzy collection of midlife complaints. The other names a measurable hormone deficiency that, when properly diagnosed, genuinely responds to treatment. Men in their 40s and 50s deserve to know which is which, because the wrong label leads to the wrong intervention — and the wrong intervention (unnecessary lifelong testosterone) carries real risks. In this article I’ll walk you through what andropause actually is (and isn’t), how late-onset hypogonadism is diagnosed by EAU and Endocrine Society criteria, which symptoms actually point to low testosterone, and who genuinely benefits from treatment.
Key Takeaways
- Andropause is a popular term, not a medical diagnosis — it has no biochemical threshold and no agreed criteria.
- Late-onset hypogonadism (LOH) requires both specific symptoms and a confirmed low morning total testosterone, typically below 12 nmol/L (350 ng/dL), on two separate mornings.
- Most men with vague midlife fatigue do not have LOH — obesity, sleep apnea, alcohol, opioids and chronic illness suppress testosterone and are reversible.
- Specific symptoms (reduced morning erections, fewer sexual thoughts, hot flushes, small testes) carry far more diagnostic weight than fatigue or low mood alone.
- Testosterone replacement therapy (TRT) is appropriate only when biochemical LOH is confirmed and reversible causes have been addressed first.
Andropause vs. Late-Onset Hypogonadism: The Real Difference
Let me start by being blunt: “andropause” is not a recognized medical diagnosis. You won’t find it in the ICD-11. The EAU doesn’t define it. The Endocrine Society doesn’t either. It’s a popular shorthand — borrowed from “menopause” — that suggests men go through an equivalent abrupt hormonal cliff in midlife. They don’t.
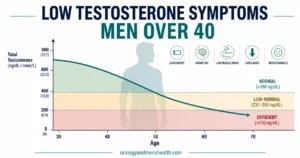
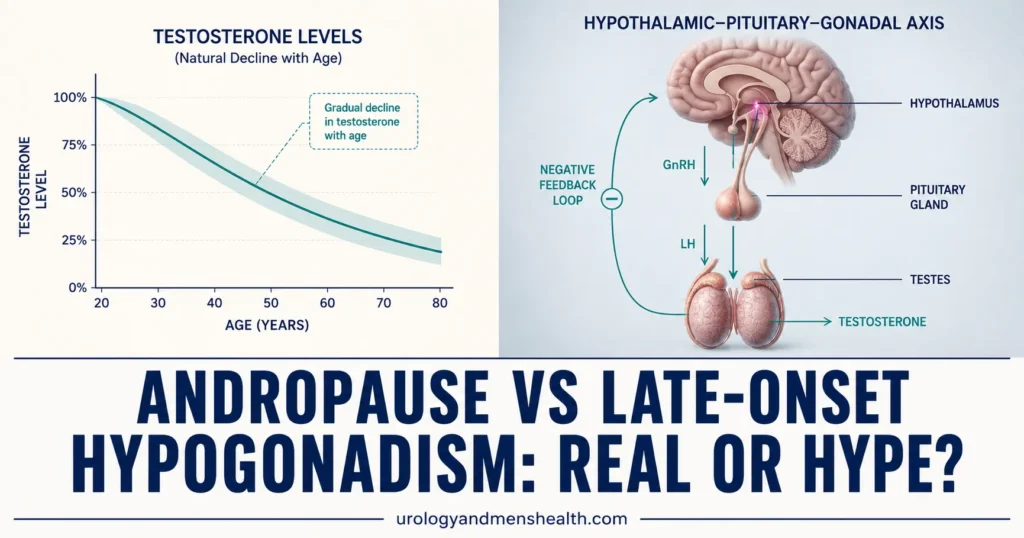
Female menopause is a defined biological event: ovarian estrogen production stops, periods end, and the change is universal and sharp. Male testosterone, by contrast, declines slowly — roughly 1-2% per year after age 30 [1]. Most men in their 60s still have testosterone levels within the normal adult male range. The decline is real, but it is gradual and highly individual.
Late-onset hypogonadism (LOH) is the actual medical term. The European Association of Urology defines it as “a clinical and biochemical syndrome associated with advancing age” requiring both characteristic symptoms and a confirmed deficiency of testosterone [2]. Two ingredients, not one. A man with a low testosterone level but no symptoms does not have LOH. A man with classic symptoms but a normal testosterone level does not have LOH either. Both must be present.
This distinction is not academic. If you accept “andropause” as a diagnosis, you accept that age alone justifies testosterone treatment — and that’s exactly how a lot of “low T” clinics market themselves. If you accept LOH, you accept that age alone is not enough and that the diagnosis requires a specific workup. For a full overview of male testosterone biology and symptoms, see our Sexual Health Hub.
What Testosterone Actually Does (And Why Decline Matters)
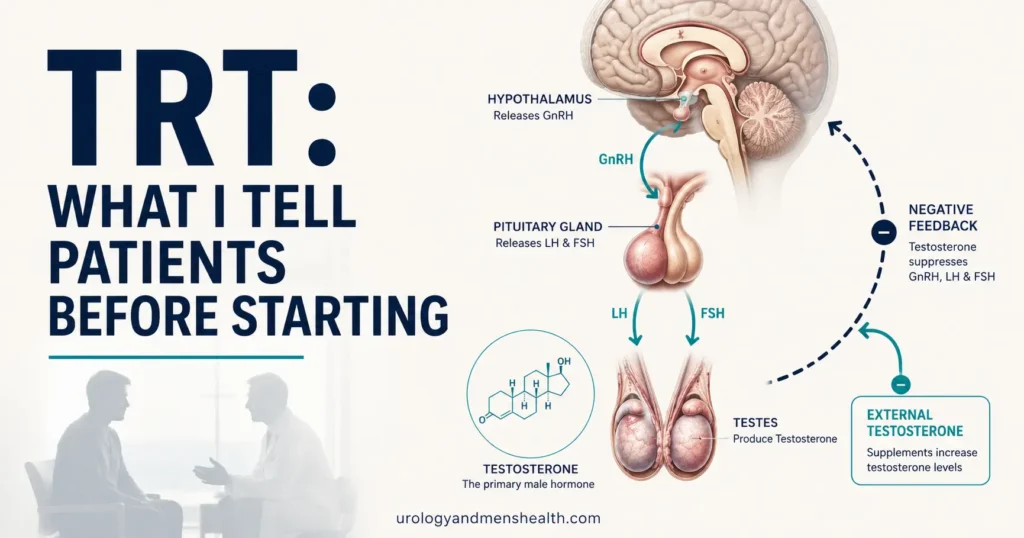
Testosterone is regulated by a feedback loop called the hypothalamic-pituitary-gonadal (HPG) axis. The hypothalamus releases GnRH, which tells the pituitary to release LH and FSH, which in turn tell the Leydig cells in the testes to make testosterone. When testosterone is high enough, it signals back to the brain to slow down — a thermostat. When this loop is intact, testosterone stays in a healthy range without intervention.
What testosterone does in adult men is broader than most patients realize:
- Libido and erection quality — testosterone drives sexual desire and supports the nitric oxide pathway that produces erections.
- Muscle and bone — it maintains lean mass and bone mineral density; chronic deficiency causes osteoporosis in men.
- Red blood cell production — it stimulates erythropoiesis, which is why TRT raises hematocrit.
- Mood and cognition — modest effects on energy, drive, and spatial memory.
- Fat distribution — low testosterone shifts fat to abdominal stores, which themselves further suppress testosterone (the obesity-testosterone vicious cycle).
The reason age-related decline matters clinically is not the average — it’s the tail. Most men age into their 70s with workable testosterone levels. A minority drop into a deficient range and develop genuine symptoms. That minority is who LOH is meant to identify.
In My Practice
A 52-year-old IT executive came to me convinced he had “male menopause.” He had read about andropause online, ordered an at-home testosterone test that came back at 11 nmol/L, and wanted a prescription for testosterone gel. When I sat with him, the story unfolded differently: he was 30 lbs heavier than five years ago, snored badly enough that his wife slept in another room, drank four beers most evenings, and had stopped exercising. We did a proper morning testosterone (10.8 nmol/L), confirmed it on a second sample (11.4 nmol/L), and got a sleep study (moderate OSA, AHI 22). Eight months later — CPAP nightly, 22 lbs lost, alcohol cut to weekends — his testosterone was 16.2 nmol/L. He never needed TRT.
The clinical takeaway: in men under 60 with borderline-low testosterone and lifestyle red flags, treating the reversible causes first usually fixes the number — and protects future fertility, hematocrit, and prostate health that TRT would put at risk.
Symptoms That Actually Suggest Low Testosterone
Here’s where most “andropause” articles mislead readers. They list every vague midlife symptom — fatigue, irritability, weight gain, brain fog, low motivation — and call it a hormone problem. The reality is that those symptoms have very poor diagnostic value for low testosterone. They overlap with depression, sleep deprivation, deconditioning, hypothyroidism and a dozen other conditions.
The EAU and Endocrine Society both distinguish between specific symptoms (high predictive value for genuine testosterone deficiency) and non-specific symptoms (low predictive value, common in many other conditions) [2][3].
Specific symptoms (these actually point to low testosterone)
- Reduced spontaneous and morning erections — the strongest single symptom.
- Decreased sexual thoughts and desire — not just performance issues, but lower drive itself.
- Loss of body and pubic hair — slow, often unnoticed until pointed out.
- Hot flushes and sweats — uncommon, but highly suggestive when present.
- Small or shrinking testes — testicular volume below 15 mL on examination.
- Gynecomastia — breast tissue development, especially when new.
Non-specific symptoms (low diagnostic value alone)
- Fatigue, low energy
- Low mood, irritability
- Poor concentration, “brain fog”
- Sleep disturbance
- Decreased muscle mass or strength
- Increased body fat, especially abdominal
If you have several specific symptoms together, a workup is reasonable. If you have only non-specific symptoms, the probability that low testosterone is the actual cause is low — and a testosterone test on its own is more likely to mislead you than help. Two validated questionnaires — the ADAM and AMS — try to formalize this, but both have high false-positive rates and should be used as a screen, not a diagnosis. You can try one yourself with our low testosterone symptom quiz before deciding whether bloodwork makes sense.
Wondering whether your symptoms point to low testosterone — or something else?
Enter your email below to receive Dr. Khalid’s complete Evidence-Based ED Action Plan as a free, printable PDF — covering testosterone testing, vascular causes, and what to do before asking for a prescription.
How Late-Onset Hypogonadism Is Actually Diagnosed
A proper diagnosis of LOH follows a defined sequence. Here is what should happen, and what often doesn’t.
Step 1: Morning total testosterone, fasting
Testosterone follows a strong circadian rhythm — it peaks in the early morning and drops by 30-40% by late afternoon. A testosterone test drawn at 3 PM is essentially uninterpretable. The blood should be taken between 7 and 11 AM, fasting, and ideally not during an acute illness or after a sleepless night, both of which artificially lower the value.
Step 2: Confirm on a second morning sample
A single low result is not enough. Up to 30% of men with one low reading have a normal repeat sample due to day-to-day biological variation [3]. The EAU and Endocrine Society both require confirmation on a second morning specimen before diagnosing biochemical hypogonadism.
Step 3: Interpret the number properly
The thresholds most guidelines agree on:
- Total testosterone < 8 nmol/L (230 ng/dL) — clear deficiency.
- 8-12 nmol/L (230-350 ng/dL) — equivocal zone. Need free testosterone, SHBG, LH, FSH, prolactin to clarify.
- > 12 nmol/L (350 ng/dL) — LOH unlikely; look for another cause of the symptoms.
Some labs in the US report normal ranges down to 264 ng/dL based on the Endocrine Society’s 2017 harmonization data [4]. Don’t get fixated on the exact cutoff — what matters is consistency on two morning samples plus the clinical picture.
Step 4: Distinguish primary from secondary hypogonadism
If LH and FSH are high with low testosterone → the problem is at the testes (primary hypogonadism — e.g. post-orchitis, Klinefelter syndrome, prior chemotherapy).
If LH and FSH are low or inappropriately normal with low testosterone → the problem is upstream at the pituitary or hypothalamus (secondary hypogonadism — needs prolactin, MRI of the pituitary, and assessment for other pituitary hormone deficiencies). This matters because a pituitary adenoma producing prolactin will suppress testosterone and is treatable with medication, not testosterone replacement.
A 2024 systematic review by the Endocrine Society reaffirmed that testosterone deficiency should never be diagnosed on a single sample, never on an afternoon sample, and never without LH/FSH to localize the problem [5].
Who Actually Benefits From Treatment (And Who Doesn’t)
Once biochemical LOH is confirmed and reversible causes are addressed, testosterone replacement therapy (TRT) can be genuinely helpful — but only for the right patient. The 2024 TRAVERSE trial, which followed 5,246 men with confirmed hypogonadism on TRT vs placebo for an average of 33 months, demonstrated that TRT did not increase cardiovascular events in men with confirmed deficiency — settling a long-running safety question [6]. But it also showed increased rates of atrial fibrillation, pulmonary embolism, and acute kidney injury — so the safety profile is not blank.
TRT may genuinely help
- Men with confirmed biochemical LOH (two morning samples) plus specific symptoms (reduced morning erections, low libido, hot flushes, small testes).
- Men whose reversible causes have been addressed — weight, sleep apnea, alcohol, opioids — and whose levels remain low.
- Men with primary testicular failure (high LH, low T) for whom no reversible cause exists.
- Men with documented osteoporosis or fragility fractures in the setting of low testosterone.
TRT is not indicated for
- “Andropause” without lab confirmation — age plus vague symptoms is not a diagnosis.
- Vague fatigue alone when testosterone is in the normal range — TRT will not fix tiredness caused by sleep, stress, or deconditioning.
- Men with active or recently treated prostate cancer (relative contraindication; specialist input required).
- Untreated severe sleep apnea — TRT worsens it.
- Men planning fertility within the next 12-24 months — exogenous testosterone suppresses sperm production, often for many months after stopping.
- Men with hematocrit above 54%, severe heart failure, or breast cancer.
For the specific clinical and monitoring details of starting TRT — formulations, dose adjustments, follow-up labs, prostate and cardiovascular surveillance — I cover that fully in my guide to TRT. The decision to start should never be casual; it is, in most cases, a lifelong commitment because the testes shrink and stop producing endogenous testosterone once exogenous testosterone is supplied.
What to Do Before You Ask About TRT
The single most useful thing I tell men who think they have low testosterone is: address the reversible causes first. Five conditions account for the vast majority of mildly low testosterone in men under 60, and all five are modifiable.
1. Excess weight
Obesity is the single biggest reversible suppressor of testosterone. Adipose tissue produces aromatase, an enzyme that converts testosterone to estradiol — so the more abdominal fat a man carries, the lower his testosterone runs. A BMI above 30 is associated with a 25-30% lower total testosterone compared to lean men of the same age [7]. Losing 10% of body weight typically raises testosterone by 2-3 nmol/L (60-90 ng/dL) — often enough to move a man out of the deficient range entirely. The mechanism is detailed in my article on the obesity-testosterone-ED link. Check your own metabolic risk profile with the BMI and metabolic syndrome calculator.
2. Obstructive sleep apnea
Untreated OSA disrupts the nighttime LH surge that drives morning testosterone production. Men who snore loudly, wake unrefreshed, or have witnessed apneas should get a sleep study before being labeled hypogonadal. Treating moderate-to-severe OSA with CPAP raises testosterone in a meaningful proportion of men — and untreated OSA also worsens cardiovascular risk and is a contraindication to TRT.
3. Alcohol, opioids, and anabolic steroid use
Daily alcohol intake above 2 standard drinks suppresses Leydig cell function. Chronic opioid use (including prescribed long-term pain medication) suppresses GnRH at the hypothalamus and produces profound secondary hypogonadism — often missed because the symptoms are blamed on the underlying pain condition. Past or current anabolic steroid use shuts down the entire HPG axis and may take 6-18 months to recover after cessation. Always disclose these honestly when your doctor asks.
4. Chronic illness and medications
Type 2 diabetes, chronic kidney disease, HIV, and chronic inflammatory conditions all suppress testosterone. So do common medications: glucocorticoids, finasteride, spironolactone, ketoconazole, some chemotherapy agents, and certain antidepressants. If your testosterone is borderline and you’re on any of these, that’s the conversation to have — not whether to add TRT on top.
5. Sleep, stress, and acute illness
One week of sleep restricted to 5 hours/night lowers testosterone by 10-15% in healthy young men. Acute illness, recent surgery, or major psychological stress can drop testosterone by 30% or more — a level drawn in those windows is not your baseline. Wait 6-8 weeks after any acute event before testing.
Vascular health also matters — many men I see for “low T” actually have a vascular ED that improves with cardiovascular treatment rather than hormones. If your symptoms are mainly about erections, run our ED vascular risk screener before assuming testosterone is the cause. And because vascular ED and hypertension share the same biology, see also my article on how high blood pressure damages the kidneys and vasculature — the link to sexual function is direct.
Once these are addressed, retest. If your testosterone has normalized and your symptoms have improved, you never had LOH — you had reversible suppression. If it remains low and symptoms persist, then a proper LOH diagnosis is on the table, and TRT becomes a reasonable conversation.
When to See a Urologist or Endocrinologist Promptly
Some patterns of low testosterone are not “andropause” and not LOH — they need urgent investigation:
- Sudden onset of symptoms (loss of libido, fatigue, gynecomastia) in a previously normal man — could indicate a pituitary tumor, particularly if accompanied by headaches or visual changes.
- Galactorrhea (milky nipple discharge) with low libido — suggests prolactinoma; needs prolactin level and pituitary MRI.
- Severe testicular pain, swelling, or sudden shrinkage — needs same-day urology evaluation.
- Symptoms in a man under 40 — congenital, genetic (Klinefelter), pituitary or post-treatment causes are more likely than age-related decline.
- Infertility plus low testosterone — needs semen analysis and a careful workup before considering any treatment, because conventional TRT will worsen fertility.
Frequently Asked Questions
Is andropause vs late-onset hypogonadism just a difference in name?
No — they’re fundamentally different concepts. “Andropause” is a popular term implying an inevitable, universal hormone drop that justifies treatment by age alone. “Late-onset hypogonadism” is a medical diagnosis requiring both specific symptoms and a confirmed low morning testosterone on two separate samples. Most men labeled with “andropause” do not meet criteria for LOH, and the distinction matters because it determines whether you actually need treatment. You can review the diagnostic logic in our low testosterone in men over 40 guide.
At what age does “male menopause” typically start?
It doesn’t, because male menopause as an event does not exist. Testosterone declines gradually from around age 30 at roughly 1-2% per year. Most men in their 60s and 70s still sit within the normal adult male range. Genuine late-onset hypogonadism — meeting both biochemical and symptomatic criteria — affects roughly 2-5% of men in their 40s and 50s, rising with each decade. So if you’re being told your symptoms at 45 are because of “male menopause,” you’re being given a marketing diagnosis, not a medical one.
What testosterone level confirms late-onset hypogonadism?
The EAU and Endocrine Society agree on these morning total testosterone thresholds: below 8 nmol/L (230 ng/dL) is clearly deficient; 8-12 nmol/L (230-350 ng/dL) is equivocal and needs free testosterone, LH, FSH, SHBG and prolactin to interpret; above 12 nmol/L (350 ng/dL) makes LOH unlikely. The value must be confirmed on a second morning sample drawn between 7 and 11 AM, fasting, away from acute illness. A single afternoon sample is not diagnostic regardless of the result.
Can lifestyle changes raise testosterone enough to avoid TRT?
Often, yes — especially in younger men with borderline-low levels. Losing 10% of body weight typically adds 2-3 nmol/L (60-90 ng/dL) to total testosterone. Treating obstructive sleep apnea, cutting alcohol below 2 standard drinks daily, getting consistent 7-8 hours of sleep, and resistance training all contribute. In men under 60 with testosterone in the 8-12 nmol/L range, I almost always trial 3-6 months of lifestyle changes before retesting. Many men normalize and never need TRT.
Is TRT safe long-term?
The 2024 TRAVERSE trial showed that in men with confirmed hypogonadism, TRT did not increase major cardiovascular events compared to placebo over an average of 33 months — settling a long-standing safety debate. However, TRT did modestly increase atrial fibrillation, pulmonary embolism, and acute kidney injury, and it raises hematocrit (which needs monitoring). TRT is also incompatible with maintaining fertility, suppresses natural testicular function (usually permanently after long use), and requires lifelong monitoring of PSA, hematocrit, and lipids. It is a long-term commitment, not a casual prescription. Read our detailed TRT guide for the monitoring schedule and side-effect profile.
Should I just order an at-home testosterone test to find out?
At-home tests can be a reasonable starting screen if they collect a morning sample and use a reputable lab, but they cannot diagnose late-onset hypogonadism on their own. A diagnosis requires two morning samples, plus LH, FSH, SHBG, prolactin and free testosterone in the equivocal zone, plus clinical correlation. If your at-home test is low, treat it as a signal to see your doctor for proper morning bloodwork — not as a green light to start TRT through an online clinic. The harm of a missed prolactinoma or untreated sleep apnea is real.
References
- Harman SM, Metter EJ, Tobin JD, et al. Longitudinal effects of aging on serum total and free testosterone levels in healthy men. Baltimore Longitudinal Study of Aging. J Clin Endocrinol Metab. 2001;86(2):724-731. DOI
- Salonia A, Bettocchi C, Carvalho J, et al. EAU Guidelines on Sexual and Reproductive Health — Male Hypogonadism. European Association of Urology, 2024. EAU Guidelines
- Bhasin S, Brito JP, Cunningham GR, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744. Endocrine Society
- Travison TG, Vesper HW, Orwoll E, et al. Harmonized Reference Ranges for Circulating Testosterone Levels in Men of Four Cohort Studies in the United States and Europe. J Clin Endocrinol Metab. 2017;102(4):1161-1173. DOI
- Mulhall JP, Trost LW, Brannigan RE, et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. American Urological Association, updated 2024. AUA Guideline
- Lincoff AM, Bhasin S, Flevaris P, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE Trial). N Engl J Med. 2023;389(2):107-117. NEJM
- Grossmann M. Hypogonadism and male obesity: Focus on unresolved questions. Clin Endocrinol (Oxf). 2018;89(1):11-21. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.