How to Pass a Kidney Stone Fast: A Urologist’s Protocol
When a kidney stone hits, the immediate reflex is to chug gallons of water and just pray it flushes out by morning. In reality, whether a stone passes depends entirely on its exact size and location, and blindly toughing it out at home can sometimes lead to dangerous blockages. This guide strips away the internet myths to give you my actual clinical protocol for passing a stone safely, managing the severe pain, and recognizing when you need to stop trying at home.

If you’re searching for how to pass kidney stone fast, you’re probably in real pain right now. The kind that makes you pace the room, curl up on the floor, or seriously consider going to the emergency room at 3 a.m. If you’ve been told you have a kidney stone and you want this thing out of you as quickly as possible, this is what I tell my patients.
I’m not going to pretend there’s a magic trick that makes a stone vanish instantly. There isn’t. But there is a structured protocol that maximizes your chances of passing the stone quickly, controls your pain, and — critically — helps you recognize when home management is no longer safe and you need intervention.
Roughly 86% of kidney stones pass on their own, but the timeline and likelihood depend almost entirely on two factors: stone size and stone location [1]. Everything in this article is built around those two variables.
📋 Key Takeaways
- Stones under 5 mm (about ⅕ inch) have a ~90% chance of passing spontaneously. Stones 5–10 mm: ~50%. Over 10 mm: very unlikely without intervention [2]
- NSAIDs (diclofenac/ibuprofen) are superior to opioids for kidney stone pain — they reduce ureteric spasm, not just mask the pain
- Tamsulosin 0.4 mg once daily increases spontaneous passage by 44% for stones 5–10 mm in the distal ureter — ask your doctor about it [5]
- Hydration helps, but flooding yourself with excessive water during acute colic can worsen pain by increasing pressure above the obstruction
- Fever above 100.4°F (38°C) with flank pain is a urological emergency — stop home management and go to the ER immediately
- Always strain your urine and catch the stone — composition analysis determines your entire prevention strategy going forward
In This Guide:
First: Will Your Stone Actually Pass on Its Own?
Before committing to days of home management, you need a realistic picture of whether your stone is likely to pass spontaneously. The data is clear on this:
By size
- Under 4 mm (about ⅙ inch): ~90% pass spontaneously within 1–2 weeks. These are the “grin and bear it” stones
- 4–5 mm: ~70–80% pass, but may take 2–3 weeks. Medical expulsive therapy helps
- 5–7 mm (about ¼ inch): ~50% pass. This is the gray zone where active medical management significantly improves the odds
- 7–10 mm: ~20–30% pass. Intervention is usually needed. Waiting beyond 4 weeks risks kidney damage
- Over 10 mm (about ⅖ inch): Passage is extremely unlikely. Surgical intervention (URS, PCNL, or ESWL) is standard of care [2]
Want to estimate your own odds? Try our kidney stone passage calculator — it uses your stone size and location to give you a realistic spontaneous-passage probability.
By location
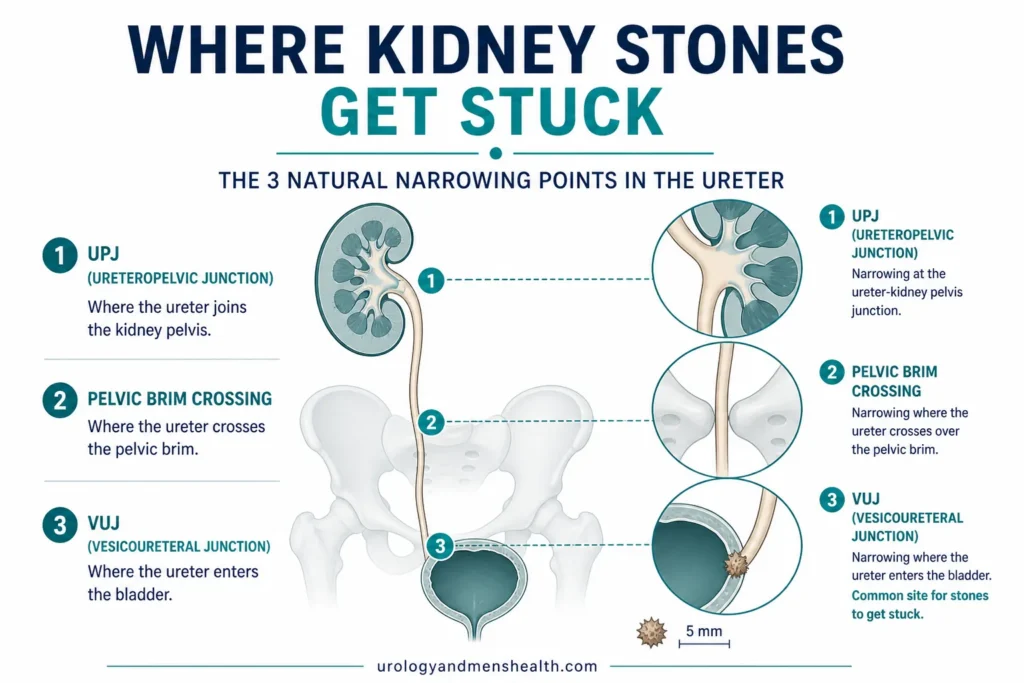
A stone’s position in the ureter matters as much as its size. The ureter has three natural narrowing points where stones get stuck:
- Ureteropelvic junction (UPJ) — where the kidney meets the ureter. Stones that lodge here cause flank pain and can take longest to move. Passage rate: lower
- Pelvic brim crossing — where the ureter crosses the iliac vessels. A common hang-up point
- Vesicoureteral junction (VUJ) — where the ureter enters the bladder. This is the narrowest point but once a stone reaches here, it’s closest to the exit. Passage rate: highest. Tamsulosin is most effective for stones at this location [3]
If your CT scan says “4 mm stone at the VUJ” — that’s the best-case scenario. High likelihood of passage with conservative management. If it says “8 mm stone at the UPJ” — that’s unlikely to pass, and you should be discussing intervention with your urologist.
→ Related Read: Kidney Stones — Complete Guide from a UrologistThe Protocol: How to Pass Kidney Stone Fast at Home
If your stone is in the passable range (under 7 mm, ideally under 5 mm), here’s the structured approach I give patients. Follow all four steps simultaneously — they work together, not independently.
Step 1: Pain management — NSAIDs first, always
Kidney stone pain (renal colic) is caused by two things: the stone physically scraping the ureter wall, and the ureter going into spasm around the stone, creating intense waves of pain. This is why the pain comes and goes in waves rather than being constant.
NSAIDs are the first-line treatment for renal colic — not acetaminophen (paracetamol), not opioids. Here’s why:
- Diclofenac (75 mg intramuscular or 50–100 mg oral/rectal) — the gold standard for acute renal colic. Reduces ureteric spasm, decreases inflammation around the stone, and provides analgesic effect. A meta-analysis of 50 trials found NSAIDs superior to opioids for renal colic, with fewer side effects and less need for rescue analgesia [4]
- Ibuprofen (400–600 mg every 6–8 hours) — available over the counter in most countries. Take with food. Maximum 2,400 mg/day for short-term use
- Ketorolac — a powerful injectable NSAID often used in emergency departments. Highly effective but short-term use only
Why NSAIDs beat opioids: Opioids (morphine, tramadol, codeine) mask pain but do nothing to reduce ureteric spasm — and they cause nausea, constipation, and drowsiness that make home management harder. NSAIDs actually address the pathophysiology (spasm and inflammation) while providing pain relief. Opioids are reserved as rescue analgesia when NSAIDs alone are insufficient [4].
Acetaminophen (paracetamol) can be used as an adjunct — 1,000 mg every 6 hours alongside NSAIDs — but on its own it’s insufficient for moderate-to-severe renal colic.
Cautions: NSAIDs should be avoided if you have impaired kidney function (eGFR <30), active peptic ulcer disease, pregnancy, or heart failure. If you fall into these categories, ask your doctor about alternatives.
Step 2: Medical expulsive therapy — tamsulosin
Tamsulosin 0.4 mg once daily is the most commonly prescribed medical expulsive therapy (MET) for kidney stones. Originally designed for prostate enlargement (BPH), tamsulosin relaxes the smooth muscle in the distal ureter, widening the channel and allowing the stone to pass more easily.
The evidence:
- A Cochrane review of 67 trials found that alpha-blockers increase spontaneous stone passage by 44% for stones 5–10 mm in the distal ureter [5]
- They also reduce the time to passage by approximately 3–5 days
- They reduce the number of pain episodes and hospitalizations during the waiting period
- The benefit is clearest for stones 5–10 mm in the distal ureter. For stones under 5 mm, the evidence is weaker (most pass quickly anyway)
How to take it: Tamsulosin 0.4 mg once daily, preferably 30 minutes after a meal. Continue until the stone passes or for a maximum of 4–6 weeks. If the stone hasn’t passed by then, intervention is needed.
Side effects: Dizziness (especially when standing up quickly), nasal congestion, retrograde ejaculation (temporary, resolves after stopping). Generally very well tolerated for the short duration used in stone management.
Tamsulosin requires a prescription. Do not skip this step — if your stone is 5 mm or larger, the difference between taking tamsulosin and not taking it can be the difference between passing the stone at home and needing surgery.
Step 3: Hydration — important but misunderstood
You’ve probably been told to “drink lots of water” to flush the stone out. That’s partially correct, but there’s an important nuance most advice misses:
During acute colic (when you’re in pain): Do NOT force excessive fluids. Over-hydration during an obstructive episode can increase pressure upstream of the stone, worsening the distention and pain. Drink normally — 2 to 2.5 liters (about 70–85 fl oz, or 8–10 cups) through the day — but don’t try to “flood” the stone out by drinking 5 liters. The physics don’t work that way.
Between pain episodes (when you’re comfortable): This is when higher fluid intake helps. Aim for 2.5–3 liters (about 85–100 fl oz, or 10–12 cups) of water daily. The increased urine flow helps push the stone downstream during the periods when the ureter isn’t in spasm. Adding lemon juice to your water is beneficial — the citrate inhibits further crystal formation around the existing stone.
Temperature matters: Warm fluids may help relax the ureter slightly. There’s no strong clinical evidence for this, but many patients report that warm water or herbal tea is more comfortable during episodes than cold water.
→ Related Read: Hydration and Kidney Health — The Water Myth vs. What Science ShowsStep 4: Activity and positioning
This is where evidence is limited, but clinical experience and patient reports consistently point in the same direction:
- Stay active. Walking and light movement help the stone migrate distally. Bed rest during pain episodes is understandable, but prolonged bed rest doesn’t help stone passage
- Gravity helps. Being upright is better than lying flat for stone migration
- Stair climbing — anecdotally recommended by many urologists. The vertical jolting motion may help dislodge stones at the pelvic brim or VUJ. No randomized trial has tested this (and probably never will), but it’s harmless and many patients report passage shortly after periods of stair climbing or brisk walking
- Heat application: A warm compress or hot water bottle applied to the affected flank provides genuine relief. It doesn’t move the stone, but it relaxes surrounding muscle and reduces spasm perception — one of the most underrated home measures
The Critical Step Everyone Forgets: Strain Your Urine
When the stone passes, it often happens with surprisingly little fanfare. You might feel a brief sharp pain followed by a sense of relief, or you might pass it without any noticeable sensation. Either way, you need to catch it.
How to strain: Urinate through a fine mesh strainer, cheesecloth, or a commercially available urine straining bag (available at pharmacies and on Amazon). Do this every time you urinate until the stone is confirmed passed. The stone may be tiny — some are the size of a grain of sand — so you need a fine mesh.
Why this matters: The stone needs to be sent for chemical composition analysis. This tells you whether it’s calcium oxalate, uric acid, cystine, or another type — and that determines your entire prevention strategy going forward. Without stone analysis, your urologist is guessing about prevention. I cannot overstate how often this step is skipped, and how much it compromises long-term management.
Once you catch the stone, place it in a clean dry container (not in water, not in formalin) and bring it to your urologist or primary care doctor for analysis.
→ Related Read: The Kidney Stone Diet — My Clinical Protocol for PreventionDownload Your Free Clinical Action Plan
Enter your email below to download Dr. Khalid’s complete 7-Day Kidney Stone Prevention Meal Plan as a free, printable PDF.
The Timeline: How Long Will This Take?
This is the question every patient asks, and the honest answer is: it depends. But here are evidence-based averages [2]:
- Stones under 2 mm: Average passage time: 8 days
- 2–4 mm: Average: 12 days. Most pass within 2 weeks
- 4–6 mm: Average: 22 days. May take up to 4 weeks
- 6–8 mm: Average: 30+ days. High chance of needing intervention
These are averages — some stones pass in 24 hours, others take weeks. The key timeframe: if a stone hasn’t passed within 4–6 weeks of confirmed diagnosis, intervention should be considered regardless of size. Prolonged obstruction beyond this window risks permanent kidney damage, even if you’re not in pain [6].
Pain is not a reliable indicator of whether the stone is still obstructing. A stone can silently obstruct the kidney without causing colic — this is why follow-up imaging (ultrasound or CT) matters if the stone hasn’t confirmed passage within 4 weeks.
Curious about your long-term recurrence odds? Use our 5-year kidney stone risk profiler to estimate your personal risk and identify the most impactful prevention steps for your situation.
What Doesn’t Work (Despite What the Internet Says)
“Olive oil and lemon juice flush”
This is one of the most persistent home remedy myths. Olive oil is absorbed in the small intestine — it never reaches your urinary tract. The citrate in lemon juice is beneficial for long-term prevention (it inhibits new crystal formation) but it cannot dissolve an existing calcium oxalate stone. The only stone type that can be dissolved medically is uric acid, and that requires alkalinizing the urine with potassium citrate over weeks, not drinking lemon juice for a day.
“Apple cider vinegar dissolves stones”
There is zero clinical evidence for this. Apple cider vinegar is acidic — if anything, acidifying the urine promotes uric acid stone formation, not prevents it. The idea that ingesting an acidic liquid will dissolve a hard mineral deposit in your kidney is a fundamental misunderstanding of human physiology. Your stomach acid is already far stronger than apple cider vinegar, and it has no effect on kidney stones.
“Beer flushes kidney stones out”
Beer temporarily increases urine output but causes net dehydration through alcohol’s diuretic effect. It also raises uric acid and promotes further stone formation. Drinking beer to pass a kidney stone is counterproductive.
“Chanca piedra (stone breaker herb)”
Phyllanthus niruri (chanca piedra) has some preliminary in-vitro evidence suggesting it may inhibit calcium oxalate crystal aggregation [7]. However, in-vitro effects don’t translate reliably to clinical outcomes. There are no large, well-designed human trials showing it passes existing stones. Relying on it during an acute stone episode instead of proven treatments (NSAIDs + tamsulosin) is not advisable.
💡 In My Practice
The most common scenario I see in my emergency practice is a man who’s been “drinking lots of water and waiting” for 2–3 weeks with a 7–8 mm proximal ureteric stone. Nobody prescribed tamsulosin. Nobody arranged follow-up imaging. He’s exhausted from pain, dehydrated from vomiting, and his creatinine is starting to rise. That stone was never going to pass on its own, and the delay has now compromised his kidney function.
On the other end, I see patients who rush to the emergency department with a 3 mm distal stone in absolute panic. After reassurance, proper pain control with diclofenac, a prescription for tamsulosin, and clear instructions on when to return, most of these patients pass their stone within a week and are grateful they avoided an unnecessary procedure.
The mistake I see most often is patients not straining their urine. They pass the stone, feel relief, and flush it away — losing the single most important piece of information for preventing the next stone. I now make patients demonstrate back to me how they’ll strain their urine before I discharge them from clinic.
⚠️ When to See a Doctor — Urgently
- Fever (temperature above 100.4°F / 38°C) with flank pain — this is a urological emergency. An infected obstructed kidney (obstructive pyelonephritis) can progress to urosepsis within hours. You need urgent drainage (ureteric stent or nephrostomy), IV antibiotics, and hospital admission. Do not wait
- Pain uncontrolled by oral medication — if NSAIDs and acetaminophen aren’t managing the pain, you need parenteral analgesia in the emergency department
- Persistent vomiting — if you can’t keep fluids or medications down, you’ll become dehydrated and unable to take oral pain relief. IV hydration and anti-emetics are needed
- No urine output for more than 12 hours — may indicate complete bilateral obstruction or obstruction of a solitary kidney. Urgent assessment required
- Visible blood in urine that is getting progressively worse — mild hematuria (blood in the urine) is expected, but worsening gross hematuria with clots needs evaluation
- You have one kidney — any obstruction of a solitary kidney requires close monitoring and a lower threshold for intervention
These red flags are non-negotiable. I’ve seen patients delay presentation with infected obstruction because they thought the fever was “just the flu.” By the time they arrived, they had septic shock and required ICU admission. An infected stone is one of the few true emergencies in urology — don’t gamble with it.
After the Stone Passes: What Happens Next
- Send the stone for analysis. Bring it to your urologist or primary care doctor in a dry container. This determines your stone type and guides prevention
- Get follow-up imaging. A repeat ultrasound or CT 4–6 weeks after the episode confirms the stone has passed and checks for any remaining fragments or hydronephrosis (kidney swelling)
- Start prevention immediately. Don’t wait for the next stone. Start the hydration protocol, dietary modifications, and discuss whether you need a 24-hour urine metabolic evaluation — especially if this is your second stone or you have a family history
- Understand your recurrence risk. Without preventive measures: 50% chance of another stone within 5 years, 80% within 10 years [8]. With proper prevention (hydration + diet + medical therapy where indicated): 10–15%. The difference is entirely within your control
Frequently Asked Questions
Can I go to work with a kidney stone?
It depends on the severity. Between colic episodes, many patients are functional — uncomfortable but able to work, especially with adequate NSAID cover. During acute colic, you will not be able to work or do anything else. If your job involves heavy physical labor, driving, or operating machinery, take time off until the pain pattern is predictable and controlled. A desk job may be manageable with medication and a bathroom nearby — and a strainer if you’re hoping to catch the stone. See our complete kidney stones guide for more on what to expect.
How do I know if the stone has passed?
Usually a combination of: sudden relief of pain (the most common sign), catching the stone in your strainer, or clearance confirmed on follow-up imaging. Some small stones pass without any noticeable sensation. If your pain has completely resolved for 48 or more hours, the stone has very likely passed — but follow-up imaging should confirm this if the stone was above 4–5 mm. You can also estimate your odds with our stone passage calculator.
Is it safe to take ibuprofen for 2–3 weeks?
Short-term NSAID use (2–4 weeks) is generally safe in patients with normal kidney function, no peptic ulcer history, and no heart failure. Take with food or use a gastroprotective agent (omeprazole) if using for more than a week. If your kidney function is impaired — ask your doctor about your eGFR — NSAIDs should be avoided. Use acetaminophen instead and discuss alternatives with your doctor. Read more about kidney health and hydration to support recovery.
Should I go to the ER or wait for a doctor’s appointment?
Go to the ER if: pain is uncontrolled, you have fever, you can’t stop vomiting, or you have no urine output. For everything else, an urgent appointment with your primary care doctor or urologist within 24–48 hours is appropriate — they can prescribe NSAIDs, tamsulosin, and arrange imaging. Not every kidney stone needs an ER visit, but don’t suffer in silence either.
Can kidney stones come back?
Yes, and they frequently do. Without prevention, the recurrence rate is approximately 50% within 5 years. This is why stone analysis, metabolic evaluation, and dietary modification matter so much. A single kidney stone should be treated as a warning signal, not a one-off event. The patients who take prevention seriously almost never come back for a second stone — start with our kidney stone diet protocol.
📚 References
- Preminger GM, Tiselius HG, Assimos DG, et al. 2007 Guideline for the management of ureteral calculi. J Urol. 2007;178(6):2418–2434. AUA — J Urol
- Coll DM, Varanelli MJ, Smith RC. Relationship of spontaneous passage of ureteral calculi to stone size and location as revealed by unenhanced helical CT. AJR Am J Roentgenol. 2002;178(1):101–103. PubMed
- Jendeberg J, Geijer H, Alshamari M, et al. Size matters: the width and location of a ureteral stone accurately predict the chance of spontaneous passage. Eur Radiol. 2017;27(11):4775–4785. PubMed
- Holdgate A, Pollock T. Nonsteroidal anti-inflammatory drugs (NSAIDs) versus opioids for acute renal colic. Cochrane Database Syst Rev. 2005;(2):CD004137. PubMed
- Campschroer T, Zhu X, Vernooij RWM, Lock MTWT. Alpha-blockers as medical expulsive therapy for ureteral stones. Cochrane Database Syst Rev. 2018;(4):CD008509. PubMed
- Skolarikos A, Neisius A, Petřík A, et al. EAU Guidelines on Urolithiasis. European Association of Urology. 2024. EAU Guidelines
- Barros ME, Lima R, Mercuri LP, et al. Effect of extract of Phyllanthus niruri on crystal deposition in experimental urolithiasis. Urol Res. 2006;34(6):351–357. PubMed
- Moe OW. Kidney stones: pathophysiology and medical management. Lancet. 2006;367(9507):333–344. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.