HoLEP vs TURP: Which Prostate Surgery Wins? | Urologist
Discover why clinical guidelines now favor HoLEP over TURP for large prostates. Compare side effects, recovery times, and long-term outcomes.

When a man asks me whether HoLEP vs TURP is the better choice for his enlarged prostate, what he’s really asking is a more honest question: which surgery gives me the best chance of fixing this once, with the fewest side effects, and the shortest recovery? After 11 years of doing both procedures, my answer has shifted. TURP used to be the default. Today, for any prostate over 80 mL, or any man on blood thinners, or any man who simply does not want to come back for a second surgery in ten years, holmium laser enucleation of the prostate (HoLEP) is the better operation. That’s not marketing — that’s what the AUA 2024 guidelines, EAU 2024 guidelines, and a decade of head-to-head trials now say. For the wider picture on when surgery becomes the right call, see our complete Prostate Health Hub. The catch is that HoLEP is harder for surgeons to learn, so it is not yet offered everywhere. This article walks you through what each procedure actually does, where the evidence is unequivocal, and where you should push back if your urologist hands you a one-size answer.
Key Takeaways
- HoLEP and TURP both relieve BPH obstruction, but HoLEP removes more tissue and produces lower retreatment rates at 5-10 years (around 1-2% vs 7-15% for TURP).
- For prostates larger than 80 mL, HoLEP is the procedure of choice per AUA 2024 — TURP becomes technically difficult and bloody above this size.
- HoLEP is safe to perform on men taking aspirin, clopidogrel, or warfarin without stopping them — TURP requires stopping anticoagulants and carries a 2-9% transfusion risk.
- Retrograde ejaculation (dry orgasm) happens in 60-85% of men after either procedure — this is the side effect men consistently underestimate before consenting.
- The most important question is not “HoLEP or TURP” but “is the surgeon I’m being sent to high-volume in the procedure they’re recommending?”
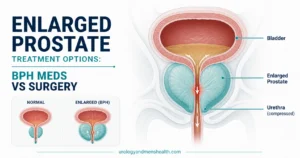
Why an Enlarged Prostate Needs Surgery in the First Place
The prostate is a walnut-sized gland that sits below the bladder and wraps around the urethra — the tube urine exits through. From your mid-40s onwards, the inner zone (the transition zone) of the prostate slowly enlarges in most men. We call this benign prostatic hyperplasia (BPH). The gland is not cancerous, but as the inner tissue swells, it pinches the urethra like a hand closing around a garden hose.
Most men manage BPH for years with medication — typically tamsulosin or finasteride. Surgery enters the conversation when one of four things has happened: medication has stopped working, the bladder is no longer emptying (urinary retention), kidney function is being affected by back-pressure, or quality of life has collapsed because of constant trips to the bathroom. If you’re at the earlier end of this journey, our overview of enlarged prostate (BPH) treatment covers when surgery becomes the right call.
Once surgery is on the table, the question becomes: which surgery? For decades, the answer was almost always transurethral resection of the prostate (TURP). Since the early 2000s, that monopoly has been challenged by holmium laser enucleation — HoLEP — which the AUA now calls a “size-independent” alternative with better long-term outcomes.[1]
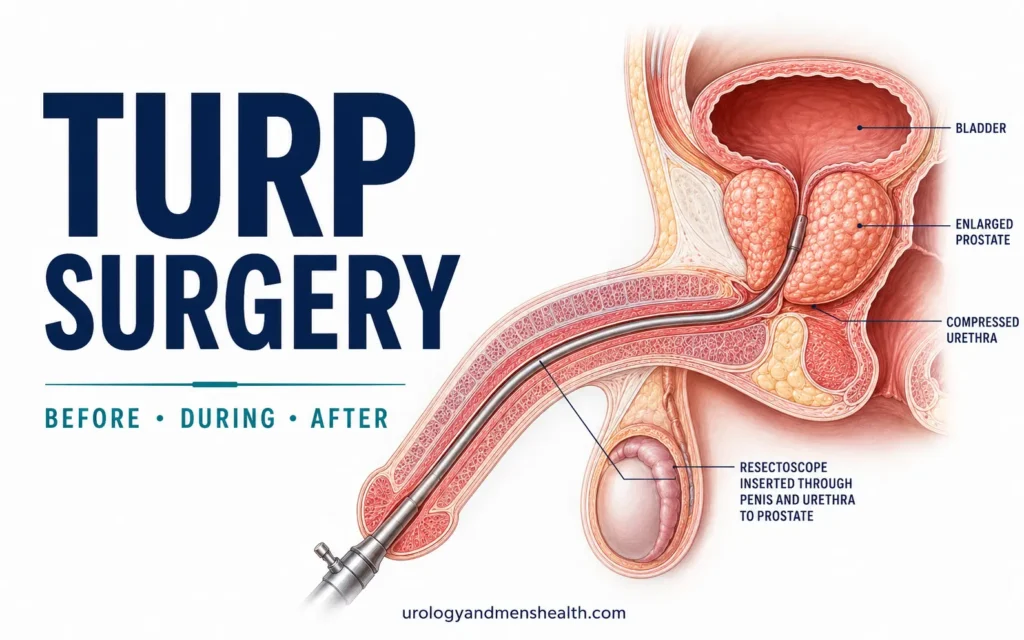
What Is TURP, and How Does It Actually Work?
TURP has been the reference standard for BPH surgery since the 1960s. A rigid scope called a resectoscope is passed up the urethra under spinal or general anesthetic. At the tip is a heated electrical wire loop. The surgeon repeatedly slices small curls of obstructing prostate tissue from inside the gland, like coring out the inside of an apple while leaving the outer skin intact. The chips are flushed into the bladder, then collected and sent for histology.
The chipping is slow. For a prostate of average size (40-60 mL), TURP takes 60-90 minutes. For an 80 mL prostate it can take two hours. Above 100 mL, surgeons increasingly run into TUR syndrome — a dangerous fluid overload from the irrigation solution being absorbed into the bloodstream. This is the reason most urologists set 80-100 mL as the practical upper size limit for TURP.
Modern TURP uses bipolar energy and saline irrigation, which has reduced (but not eliminated) the TUR syndrome risk. It’s a good, well-understood operation for the right patient — typically a prostate under 80 mL, a man not on anticoagulants, with no urgent need to avoid retreatment a decade later. For a detailed walkthrough of the procedure itself, see our piece on TURP surgery: before, during, and after.
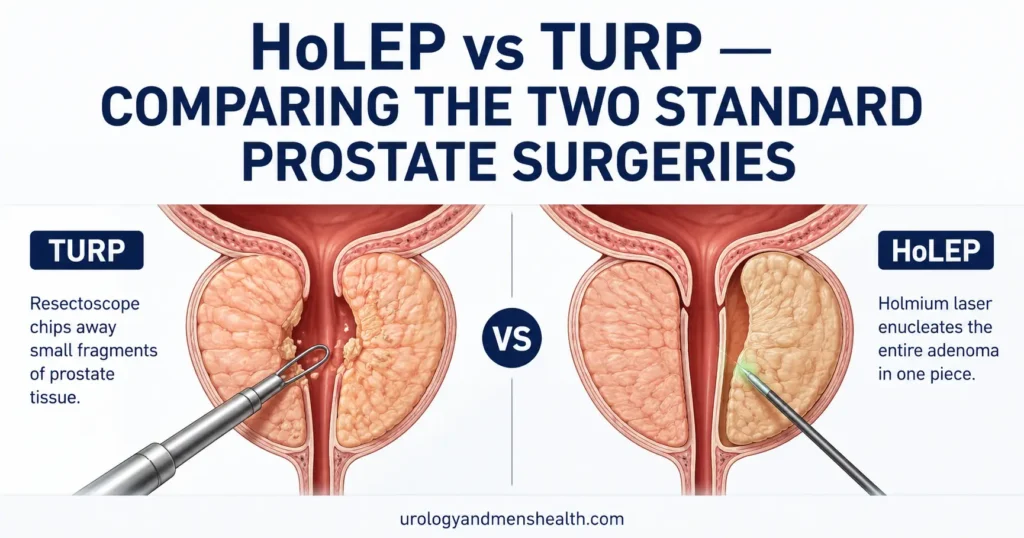
What Is HoLEP, and Why Is It Different?
HoLEP uses a holmium:YAG laser delivered through a thin fiber inside a similar scope. But the technique is fundamentally different. Instead of chipping away tissue from the inside, the surgeon uses the laser to find the natural plane between the obstructing inner prostate (the adenoma) and the outer surgical capsule. We then peel the entire adenoma off in one or two large lobes — like separating segments of an orange from the rind.
The freed lobes drop into the bladder. A device called a morcellator is then passed up to chop and aspirate them out through the scope. The end result is that almost all of the obstructing tissue is gone in one operation — the same anatomical result you’d get from open prostatectomy (the old “make a cut in the lower abdomen” operation), but done entirely through the urethra with no external incision.[2]
This is the central reason HoLEP outperforms TURP at long follow-up. TURP leaves behind tissue. HoLEP removes the whole adenoma. Ten years later, that residual TURP tissue is what regrows and causes the second surgery.
I remember a 71-year-old patient who came to see me three years ago, frustrated. He’d had a TURP at age 60 for a 70 mL prostate and was happy for about eight years. Then his stream slowed again, he started getting up four times a night, and his post-void residual had climbed to 280 mL. His imaging now showed a regrown gland of about 95 mL — large enough that doing another TURP would be technically difficult. We took him for HoLEP. Final tissue weight from the morcellator: 64 grams. He’s now two years out, voiding at 22 mL/sec with a residual under 30 mL. His comment afterwards stays with me: “Why didn’t they just do this the first time?”
The honest answer is that HoLEP wasn’t widely available a decade ago. Today, for any prostate above 80 mL — and arguably for most prostates above 60 mL — it’s the operation I recommend first.
HoLEP vs TURP: The Head-to-Head Numbers
The two procedures have now been compared in dozens of randomized trials and several Cochrane reviews. The pattern is consistent. HoLEP wins on bleeding, catheter time, hospital stay, and long-term retreatment. TURP wins on surgeon availability and learning curve. They tie on symptom relief at one year — both move the IPSS score from roughly 20 down to around 7-8 in most patients.[3]
Bleeding and Transfusion Risk
The holmium laser cauterizes blood vessels as it cuts. TURP’s electric loop also cauterizes, but less effectively in larger glands with rich blood supply. Pooled data show TURP has a transfusion rate of about 2-9% depending on prostate size. HoLEP’s transfusion rate sits around 0-1%.[3] This matters enormously for men on aspirin, clopidogrel, warfarin, or apixaban. HoLEP can typically be done without stopping these medications. TURP usually cannot.
Hospital Stay and Catheter Time
After HoLEP, most men leave hospital the next morning with the catheter removed within 24-36 hours. After TURP, the average catheter time is 48-72 hours and hospital stay is 2-3 nights. The reason is straightforward — less bleeding means clearer urine sooner, which means the catheter can come out sooner.
Long-Term Retreatment Rate
This is the single most undersold advantage of HoLEP. At 5 years, the chance of needing a second BPH procedure is about 1-2% after HoLEP and 7-15% after TURP. At 10 years, the gap widens further.[4] If you’re 60 years old at the time of your first surgery and you’d like to avoid a second one in your 70s, this number should weigh heavily in your decision.
Prostate Size Suitability
TURP becomes increasingly difficult above 80 mL. HoLEP has been shown effective at 200 mL and beyond — making it the modern transurethral answer to the very large prostate that used to require open surgery.[5] If you don’t know your prostate size, ask your urologist — it’s measured on transrectal ultrasound or MRI. You can also estimate the symptom severity that prompted surgery using the IPSS Prostate Symptom Score.
Choosing Between HoLEP and TURP? Take Dr. Khalid’s BPH & Prostate Screening Guide with You
Enter your email below to receive Dr. Khalid’s complete BPH & Prostate Screening Guide as a free, printable PDF. Covers what to ask before consenting to surgery, how to verify your urologist’s procedure volume, and the recovery checklist most patients are never given.
The Side Effect Men Underestimate: Retrograde Ejaculation
Both surgeries widen the channel through the prostate. That same widening also disrupts the bladder neck muscle that closes during orgasm to push semen forward. When that muscle no longer closes properly, semen takes the path of least resistance — backwards into the bladder, where it mixes with urine and is passed out the next time you urinate. This is retrograde ejaculation. The orgasm itself feels the same. There is just no fluid coming out.
The published rates are 60-75% after TURP and 70-85% after HoLEP. This is the single most consistent regret I hear in clinic — not because the symptom is dangerous (it isn’t, and it doesn’t affect orgasm pleasure or erection), but because men weren’t warned clearly. If you intend to father children, retrograde ejaculation is a fertility problem and you need to bank sperm before surgery. If your concern is purely sensation and ejaculate volume, this needs to be a frank pre-op conversation. Newer “ejaculation-preserving” HoLEP variants exist but the evidence on whether they reliably preserve antegrade ejaculation is still mixed.[6]
For a fuller picture of what sexual function looks like after prostate surgery — and the recovery timeline for erection quality, which is generally well preserved with both procedures — see our guide to sex after prostate surgery recovery. If your sexual concerns predate the surgery, that may be more about vascular health than the prostate itself; our piece on ED, heart disease, and what morning wood actually tells you covers why that distinction matters.
Which Surgery Suits Which Patient?
Here’s how I think through this in clinic, based on AUA 2024 guidance and my own case mix:
- Prostate under 40 mL, no anticoagulants, no urgency: Either procedure works well. TURP is typically more available and the choice can be made on local surgeon expertise. Minimally invasive options like UroLift or Rezum may also be reasonable here.
- Prostate 40-80 mL: Both procedures perform similarly at one year. HoLEP edges ahead on bleeding and retreatment. Use surgeon expertise as the tiebreaker — a high-volume TURP surgeon is a better choice than a low-volume HoLEP surgeon.
- Prostate 80-150 mL: HoLEP is the procedure of choice if a trained surgeon is available. TURP becomes technically harder and bloodier in this size range.
- Prostate over 150 mL: HoLEP or open simple prostatectomy. TURP is not a reasonable option.
- Any prostate size on anticoagulants: HoLEP. Period. It can usually be done without stopping the drugs.
- Urinary retention with a catheter in place: HoLEP has slightly better catheter-free rates at 6 months. Either procedure is reasonable.
- Concern about retrograde ejaculation: Discuss ejaculation-preserving HoLEP variants, but understand the data is limited. The standard counseling rate is 70-85% retrograde with HoLEP.
If you’re still weighing whether surgery is the right next step versus medication adjustment, our BPH Treatment Finder walks through the decision tree based on your specific symptoms, prostate size, and medication history.
What About Newer Options — Aquablation, UroLift, Rezum?
The BPH surgery world is more crowded than it was a decade ago. Aquablation uses a high-pressure water jet under ultrasound guidance to remove tissue. UroLift uses implants to physically pull the prostate lobes apart without removing tissue. Rezum injects steam to ablate tissue. Each has a role, but none of them have the long-term retreatment data that HoLEP and TURP carry.
UroLift and Rezum preserve ejaculation in most men and have shorter recovery, but their retreatment rates at 5 years are higher (around 10-15%) and they’re best suited to smaller prostates without a significant median lobe. Aquablation has shown promise for medium and large prostates with results approaching HoLEP, though longer-term data is still maturing. If you want a fuller comparison, see our deep dive on aquablation therapy compared to TURP and HoLEP.
Red Flags That Mean You Should Not Delay Surgery
- You have been catheterized and your catheter trial without catheter (TWOC) has failed once or twice.
- Your kidney function (creatinine) is climbing and ultrasound shows hydronephrosis (back-pressure dilation of the kidneys).
- You’ve had recurrent UTIs that resolve with antibiotics and recur within weeks.
- You’re passing visible blood in your urine that isn’t explained by another cause.
- Your bladder shows trabeculation (thickened, worked-up walls) on ultrasound — a sign the bladder muscle is starting to fail from chronic obstruction.
Any of these means surgery is not just an option — it’s the protective intervention. Delay risks permanent bladder damage that surgery can no longer reverse.
Frequently Asked Questions
Is HoLEP better than TURP for everyone, or only for large prostates?
HoLEP outperforms TURP on bleeding, catheter time, hospital stay, and long-term retreatment rate at every prostate size — but the gap is largest above 80 mL. For a prostate under 40 mL, both procedures give similar results at one year, so the choice often comes down to local surgeon expertise. For any prostate larger than 80 mL, or any man on blood thinners, HoLEP is the operation I recommend first. Our BPH Treatment Finder walks through the decision with your specific numbers.
How long does recovery actually take after HoLEP vs TURP?
Catheter is typically out within 24-36 hours after HoLEP and 48-72 hours after TURP. Most men return to desk work in 1-2 weeks and to physical activity at 4-6 weeks. Mild blood-tinged urine and burning on urination can persist for 2-4 weeks after either procedure. Heavy lifting, cycling, and sexual activity are usually restricted for 4-6 weeks. The recovery curve for HoLEP is slightly steeper at the front end (more burning in week 1) but cleaner overall — see our detailed week-by-week guide on TURP recovery, most of which applies to HoLEP too.
Will I still be able to have sex after HoLEP vs TURP?
Erection function is preserved in 90-95% of men after both procedures — neither operation routinely damages the nerves responsible for erection. What changes for most men is ejaculation: 60-85% will experience retrograde ejaculation (a dry orgasm where semen passes into the bladder instead of out the urethra). This doesn’t affect pleasure or erection, but it does affect fertility and ejaculate volume. If fathering children is a goal, bank sperm before surgery.
Can HoLEP be done if I’m on blood thinners like warfarin or apixaban?
Yes — this is one of HoLEP’s clearest advantages. The holmium laser cauterizes blood vessels as it cuts, so HoLEP can usually be performed without stopping aspirin, clopidogrel, warfarin, or apixaban. TURP, by contrast, has a 2-9% transfusion risk and almost always requires stopping anticoagulants pre-operatively — which carries its own cardiovascular risk in men with stents or atrial fibrillation. Always confirm the plan with your cardiologist and urologist together.
How do I find a high-volume HoLEP surgeon? Not every urologist offers it.
HoLEP has a longer learning curve than TURP — surgeons need around 30-50 cases to reach competency and 100+ to reach mastery. Ask your urologist directly: “How many HoLEPs have you personally performed in the last 12 months?” A safe answer is 50 or more. If the number is under 20, ask for a referral to a higher-volume center. The trade-off is real: a high-volume TURP surgeon will produce a better outcome than a low-volume HoLEP surgeon. Volume matters more than the procedure name.
Does HoLEP increase my risk of urinary incontinence?
Permanent stress incontinence after HoLEP is rare — around 1-2% — and similar to TURP. Temporary urgency and occasional leakage in the first 4-8 weeks is common after both procedures (sometimes called “transient urge incontinence”) and almost always resolves with time and pelvic floor exercises. If incontinence persists beyond 3 months, it warrants further assessment. The bladder neck and external sphincter are both anatomically preserved during a properly performed HoLEP.
References
- Sandhu JS, Bixler BR, Dahm P, et al. Management of Lower Urinary Tract Symptoms Attributed to Benign Prostatic Hyperplasia: AUA Guideline Amendment 2023. J Urol. 2024;211(1):11-19. AUA Guideline
- Gilling PJ, Wilson LC, King CJ, et al. Long-term results of a randomized trial comparing holmium laser enucleation of the prostate and transurethral resection of the prostate: results at 7 years. BJU Int. 2012;109(3):408-411. PubMed
- Cornu JN, Ahyai S, Bachmann A, et al. A Systematic Review and Meta-analysis of Functional Outcomes and Complications Following Transurethral Procedures for Lower Urinary Tract Symptoms Resulting from Benign Prostatic Obstruction. Eur Urol. 2015;67(6):1066-1096. PubMed
- Elmansy HM, Kotb A, Elhilali MM. Holmium laser enucleation of the prostate: long-term durability of clinical outcomes and complication rates during 10 years of follow-up. J Urol. 2011;186(5):1972-1976. PubMed
- Kuntz RM, Lehrich K, Ahyai SA. Holmium laser enucleation of the prostate versus open prostatectomy for prostates greater than 100 grams: 5-year follow-up results of a randomised clinical trial. Eur Urol. 2008;53(1):160-168. PubMed
- Gravas S, Gacci M, Gratzke C, et al. EAU Guidelines on the Management of Non-Neurogenic Male Lower Urinary Tract Symptoms (LUTS), incl. Benign Prostatic Obstruction (BPO). European Association of Urology. 2024. EAU Guideline
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.