Blood Pressure Medication and ED: Which Pills Cause It, Which Don’t
Most men blame their blood pressure medication for ED, but only two drug classes reliably cause it — and switching, not stopping, usually fixes the problem. Here's how I sort it out in clinic.

The link between blood pressure medication and ED is one of the most common worries I hear in clinic — and one of the most misunderstood. A man notices his erections have weakened a few weeks after starting a new pill, connects the dots, and quietly stops taking it. The problem is that high blood pressure itself is a leading cause of erectile dysfunction, so it is genuinely hard to know whether the drug, the disease, or simple worry is to blame. The good news is that only two drug classes reliably cause erectile problems, several are completely neutral, and at least one may actually improve erections. Stopping treatment is almost never the right move and can be dangerous. For the broader picture, see our Blood Pressure & Kidney Hub. This article walks through exactly which pills are the culprits, which are safe, and what to ask your doctor for.
Key Takeaways
- Only two antihypertensive classes are consistently linked to ED: older beta-blockers (propranolol, atenolol) and thiazide diuretics (hydrochlorothiazide).
- ACE inhibitors, ARBs, and calcium channel blockers are ED-neutral; the ARB class and the beta-blocker nebivolol can preserve or even improve erections.
- In a landmark trial, the same beta-blocker caused ED in 3% of men told nothing versus 31% warned of the side effect — expectation is a powerful driver.
- Never stop a BP medication on your own; switching the class under medical supervision usually fixes the problem while keeping your pressure controlled.
Can Blood Pressure Medication Really Cause ED?
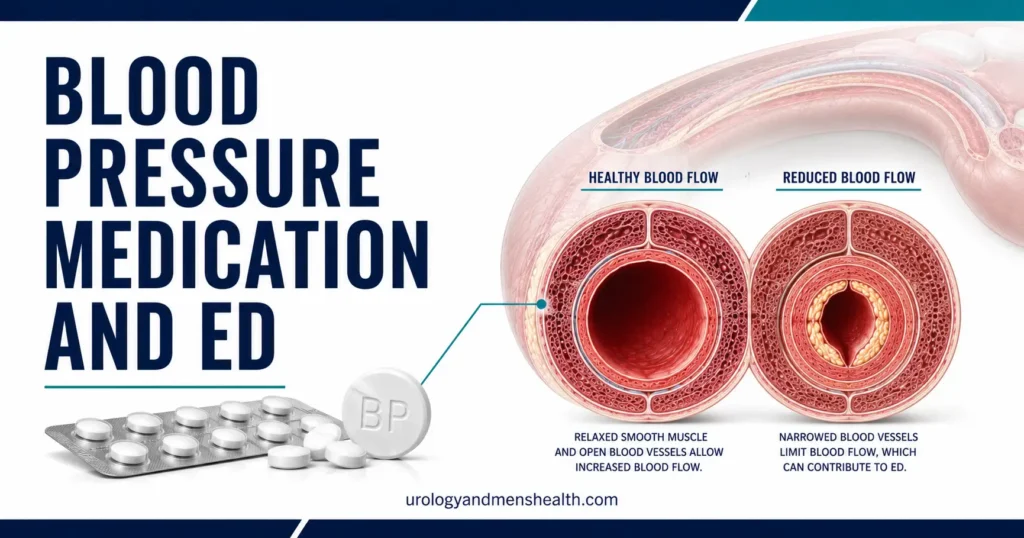
Yes — but far less often than men assume, and not from the drugs most people fear. To understand why, you have to know how an erection actually works. An erection is a vascular event: nerve signals trigger the release of nitric oxide, which relaxes the smooth muscle lining the penile arteries so blood can rush in and stay trapped. Anything that narrows those arteries or blunts that nitric-oxide signal weakens the result.
Here is the part that catches men off guard. Untreated high blood pressure is itself one of the most powerful causes of ED, because years of elevated pressure damage the delicate lining (endothelium) of those small arteries — the same way it quietly scars the blood vessels feeding your kidneys. So a man with hypertension often already has reduced penile blood flow before he ever opens a pill bottle. When erections falter, the medication gets the blame, but the disease was setting the stage long before.
That distinction matters because the fix is completely different. If the disease is the problem, controlling your pressure protects you. If a specific drug is the problem, switching it solves it. A quick ED vascular risk screener can help you gauge how much of your difficulty is likely vascular versus drug-related before your appointment.
The Blood Pressure Pills Most Likely to Cause ED
Two classes carry the real reputation, and a third is worth knowing about.
Older beta-blockers — propranolol and atenolol in particular — are the classic offenders. They blunt the sympathetic nervous system to slow the heart, but in doing so they can reduce penile blood flow and dampen the signals that initiate an erection. A 2024 review in Endocrine confirmed that this effect is real but concentrated in the older, non-vasodilating drugs of the class [5].
Thiazide diuretics such as hydrochlorothiazide are the second class historically tied to ED, thought to act by reducing blood flow to the penis. Notably, more recent analyses have softened this verdict — the same 2024 review found that newer evidence does not consistently confirm a strong thiazide effect [5]. The risk is likely smaller than the textbooks of twenty years ago suggested.
Spironolactone, a potassium-sparing diuretic used in resistant hypertension, deserves a separate mention. It blocks androgen receptors, so at higher doses it can cause reduced libido, ED, and breast tenderness in men. This is a hormonal effect, not a blood-flow one, and it is dose-dependent.
Worried your blood pressure pills are affecting more than your numbers?
Enter your email below to receive Dr. Khalid’s complete Blood Pressure & Kidney Protection Guide as a free, printable PDF.
The Blood Pressure Pills That Are Safe — or Even Help
This is the part most men never hear, and it is the most useful. Several blood pressure drug classes have no meaningful effect on erections, and a couple appear to protect them.
ACE inhibitors (lisinopril, ramipril) and ARBs (losartan, valsartan, telmisartan) are ED-neutral and may be mildly beneficial. A double-blind study by Fogari and colleagues compared valsartan with atenolol and found that the ARB preserved sexual activity and plasma testosterone while the beta-blocker reduced both [4]. If a man with ED needs his pressure controlled, an ARB is often my preferred starting point.
Calcium channel blockers like amlodipine are consistently neutral — they lower pressure without interfering with the erection pathway.
The standout is nebivolol, a newer beta-blocker that also stimulates nitric-oxide release in the vessel wall — the very molecule that drives erections. In the MR NOED study, nebivolol left erectile function intact while metoprolol measurably reduced it over the first eight weeks of treatment [3]. So a man can stay on a beta-blocker, if he needs one, and still protect his sex life.
In My Practice
A 54-year-old patient came to me convinced his “blood pressure tablets had ended things.” He had been started on atenolol four months earlier and had quietly cut his dose in half — his pressure was creeping back up. We didn’t add an ED drug first. We simply switched him from atenolol to nebivolol and kept his dose honest. Six weeks later his erections had returned and his readings were back under target, and he was almost annoyed at how simple it had been.
Before assuming a blood pressure pill has permanently caused ED, the first question is whether a same-class or cross-class switch can solve it — it very often can.
The Nocebo Effect: When Worry Becomes the Problem
One of the most striking findings in this whole area has nothing to do with chemistry. Silvestri and colleagues gave newly diagnosed men the exact same beta-blocker (atenolol) but told three groups different things. Among men told nothing about the drug, 3% reported ED. Among those told they were taking a beta-blocker, that rose to 16%. Among those told it was a beta-blocker and warned ED was a possible side effect, 31% reported it [2].
Same molecule, same dose, tenfold difference — driven entirely by what the men expected. This is the nocebo effect: the opposite of placebo, where the expectation of harm produces real symptoms. It does not mean the ED is “imaginary.” The anxiety it creates raises sympathetic tone, which genuinely makes erections harder to achieve. It does mean that some of the ED blamed on BP pills is set in motion by the warning itself, and that anxiety is treatable.
What to Do If Your Blood Pressure Medication Is Causing ED
Here is the practical sequence I use with patients.
- Do not stop your medication. Stopping antihypertensives can spike your pressure and, with some drugs, cause a dangerous rebound. Whatever you change, change it with your doctor.
- Pin down the timeline. Did the ED begin within a few weeks of starting or increasing a specific pill? Bring the exact drug name and start date — that single detail often identifies the culprit.
- Ask about switching, not stopping. Ask your doctor directly: “Can we switch me from a beta-blocker or thiazide to an ARB, or from my current beta-blocker to nebivolol, and review my erections in 6 to 8 weeks?”
- Address the pressure itself. Better control through proven lifestyle changes can sometimes reduce your medication burden, which removes the question entirely.
- Consider a PDE5 inhibitor. If switching is not enough, a tablet like sildenafil or tadalafil works well and safely alongside most BP drugs. For the full pathway, see our step-by-step ED treatment protocol.
Never Combine These
One combination is genuinely dangerous and you must know it: PDE5 inhibitors (sildenafil, tadalafil, vardenafil) must never be taken with nitrate medications used for chest pain — including recreational “poppers.” The AUA guideline is explicit that this combination can cause a precipitous, life-threatening drop in blood pressure [1]. Tell every prescriber you take a PDE5 inhibitor, and seek emergency care for chest pain rather than reaching for nitroglycerin.
- Seek urgent care for an erection lasting more than 4 hours (priapism).
- See your doctor promptly if ED appeared suddenly alongside a new medication.
- Get evaluated if ED comes with chest pain, breathlessness, or leg swelling.
Frequently Asked Questions
Which blood pressure medication is least likely to cause ED?
ARBs (such as losartan and valsartan), ACE inhibitors, and calcium channel blockers (such as amlodipine) are the least likely to cause ED, and the beta-blocker nebivolol can actually preserve or improve erections because it boosts nitric oxide. If you need a beta-blocker but are worried about the blood pressure medication and ED connection, nebivolol is usually the smartest choice to raise with your doctor.
Will my erections recover if I switch blood pressure pills?
Usually, yes. When ED is genuinely caused by an older beta-blocker or a thiazide diuretic, switching to an ARB or to nebivolol commonly restores erections within about six to eight weeks. The recovery is not always complete if underlying vascular disease is present, which is why controlling the hypertension still matters. It is worth checking your vascular age to gauge how much is drug-related versus disease-related.
Do thiazide diuretics like hydrochlorothiazide cause erectile dysfunction?
They have historically been blamed, and the older view held that thiazides reduce penile blood flow. However, more recent evidence has not consistently confirmed a strong effect, so the risk is likely smaller than once believed. If your ED began after starting a thiazide, it is reasonable to ask about an alternative, but do not assume the diuretic is automatically the cause.
Can I take Viagra or Cialis with my blood pressure medication?
For most blood pressure drugs, yes — PDE5 inhibitors like sildenafil and tadalafil are generally safe and effective alongside them, with only a mild additive drop in pressure. The critical exception is nitrates, which must never be combined with PDE5 inhibitors. Alpha-blockers also require caution and dose separation, so always tell your doctor every medication you take before starting an ED tablet.
Is the ED from my blood pressure pill permanent?
Rarely. Drug-induced ED typically reverses once the offending medication is switched, because the effect is on blood flow or signaling rather than permanent damage. What can persist is ED driven by the underlying high blood pressure itself, which damages arteries over time. That is why the goal is to switch the pill while keeping your pressure tightly controlled, not to abandon treatment.
References
- Burnett AL, et al. Erectile Dysfunction: AUA Guideline. J Urol. 2018;200(3):633-641 (amended 2024). AUA
- Silvestri A, et al. Report of erectile dysfunction after therapy with beta-blockers is related to patient knowledge of side effects and is reversed by placebo. Eur Heart J. 2003;24(21):1928-1932. PubMed
- Brixius K, et al. Nitric oxide, erectile dysfunction and beta-blocker treatment (MR NOED study): benefit of nebivolol versus metoprolol in hypertensive men. Clin Exp Pharmacol Physiol. 2007;34(4):327-331. PubMed
- Fogari R, et al. Effect of antihypertensive treatment with valsartan or atenolol on sexual activity and plasma testosterone in hypertensive men. Eur J Clin Pharmacol. 2002;58(3):177-180. PubMed
- Anti-hypertensive medications and erectile dysfunction: focus on β-blockers. Endocrine. 2024. Springer
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.