Varicocele Surgery: When It Helps Fertility (& When Not)
Most men with a varicocele will never need surgery. The ones who do are a narrow group — and the technique they get matters more than most patients realize. Here's how I decide who to operate on.

A varicocele is a tangle of dilated veins above the testicle — and the question I get asked most in clinic is whether varicocele surgery will fix a low sperm count. The honest answer is: sometimes yes, often no, and the difference comes down to four specific criteria that most patients are never told about. About 15% of all men have a varicocele, but only a fraction of them will ever benefit from an operation. The rest are better served by observation, a partner workup, or treatment of the actual fertility bottleneck — which may not be the varicocele at all. This guide walks through who genuinely benefits from surgery, which technique gives the lowest recurrence rate, and what realistic results to expect at three, six, and twelve months. For a wider overview of male fertility, see our full Sexual Health Hub.
Key Takeaways
- Varicocele surgery only improves fertility when the varicocele is palpable on physical exam — subclinical varicoceles found on ultrasound alone do not warrant surgery per AUA-ASRM 2024.
- Realistic results: sperm concentration improves by roughly 9-12 million/mL and spontaneous pregnancy rates roughly double — from 15-17% to 33-37% at 12 months.
- Microsurgical subinguinal varicocelectomy has a recurrence rate of 1-2%, compared with 4-15% for laparoscopic, open, and embolization approaches.
- A sudden right-sided varicocele in an older man requires urgent imaging — it can signal a retroperitoneal mass obstructing the inferior vena cava.
What a Varicocele Actually Is — and Why It Affects Sperm
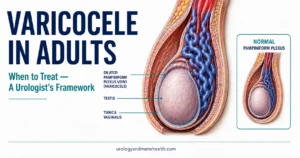
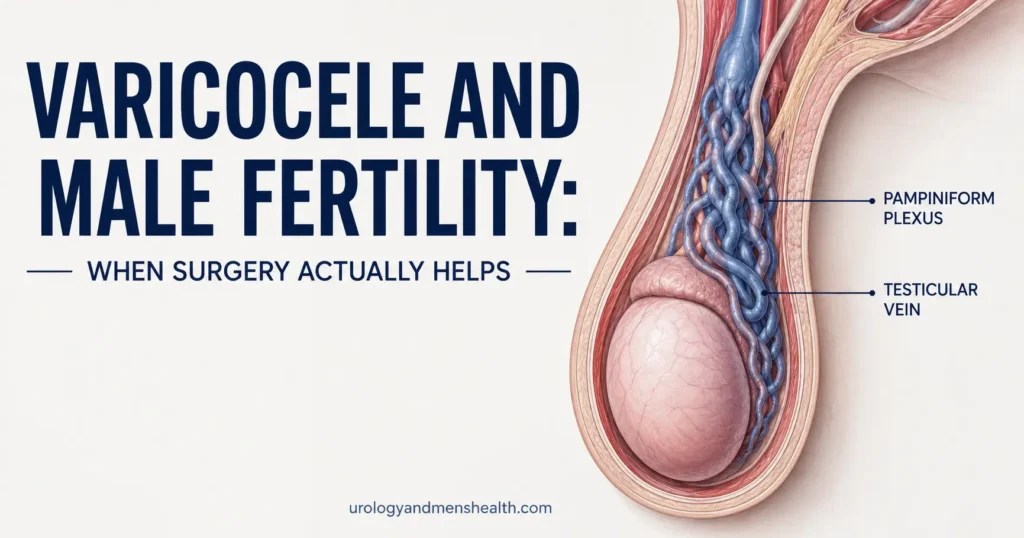
A varicocele is the same problem as varicose veins in the legs, just located in the scrotum. The veins draining the testicle — collectively called the pampiniform plexus — have one-way valves that should prevent blood from pooling backward. When those valves fail, blood backs up, the veins dilate, and you end up with what surgeons describe as a “bag of worms” feeling above the testicle.
About 90% of varicoceles occur on the left side, for an anatomical reason: the left testicular vein drains into the left renal vein at a sharp 90-degree angle, while the right testicular vein drains directly into the inferior vena cava at a gentler slope. That anatomy makes the left side mechanically prone to valve failure.
The fertility impact isn’t from the dilation itself — it’s from what the pooled blood does to the testicle. Three mechanisms matter: scrotal temperature rises by 0.5-1°C (sperm production is exquisitely temperature-sensitive), oxidative stress damages sperm DNA, and countercurrent heat exchange from refluxing renal vein blood disrupts the cooling system the testicle relies on. Together these produce the classic semen analysis picture: low concentration, poor motility, abnormal morphology, and elevated DNA fragmentation.
Most men with a left-sided varicocele have had it since their teens and have no idea. I find them on routine exams in patients who came in for something else entirely — a hydration question, a PSA discussion, a screening visit. The varicocele isn’t the problem they walked in with, and most of the time it doesn’t need to become one.
The clinical question is never “is there a varicocele” — it is “is this varicocele doing measurable harm to this man’s fertility, hormones, or comfort?”
How Varicoceles Are Graded — and Why Subclinical Ones Don’t Count
Grading is done on physical examination — not ultrasound. A urologist examines you standing up, in a warm room, asking you to perform a Valsalva maneuver (bear down as if straining at stool). The grading system in current use:
- Grade I: Vein dilation palpable only during Valsalva. Smallest clinically significant size.
- Grade II: Vein dilation palpable without Valsalva, but not visible through the scrotal skin.
- Grade III: Vein dilation visible through the scrotal skin without palpation — the classic “bag of worms” appearance.
- Subclinical: Not palpable on physical exam, detected only on ultrasound. This does not count clinically.
The subclinical distinction matters enormously. The AUA-ASRM 2024 joint guideline is explicit: surgery for subclinical varicoceles is not recommended[1]. Pooled trial data show no fertility benefit when the varicocele cannot be felt. If you have been told you have a varicocele based on ultrasound alone — without your urologist feeling one on exam — operating on it is unlikely to help you.
This is one of the most common reasons men come to me for a second opinion after a fertility workup. An ultrasound finds dilated veins, a physician recommends surgery, and the partner workup was never completed. Don’t operate on an image — operate on a clinical finding plus a fertility problem.
Who Should Actually Have Varicocele Surgery
The AUA and ASRM jointly require all four of the following criteria before recommending varicocelectomy for infertility[1]:
- The varicocele is palpable on physical examination (Grade I, II, or III).
- The couple has documented infertility — typically 12 months of unprotected intercourse without pregnancy, or 6 months if the female partner is over 35.
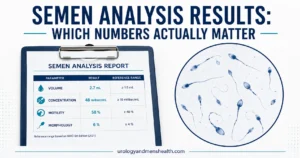
- The semen analysis shows abnormal parameters — low concentration, poor motility, abnormal morphology, or elevated DNA fragmentation. If you don’t know your numbers yet, our Semen Analysis Interpreter walks through what each value means.
- The female partner has been evaluated for tubal patency, ovulation, and age-related factors. Operating on the man without knowing whether the woman has a treatable cause is poor practice.
Three other patient groups also qualify, with slightly different reasoning:
- Adolescents with testicular growth arrest: A boy with a palpable varicocele and a difference in testicular size of more than 20% between sides should be offered surgery, even before fertility is in question. The goal is to preserve future spermatogenic potential.
- Men with low testosterone attributable to the varicocele: Varicocelectomy raises serum testosterone by roughly 100 ng/dL on average in men with pre-operative levels under 400 ng/dL[2]. If you suspect low testosterone alongside a varicocele, our Low Testosterone Symptom Quiz can clarify whether your symptoms fit.
- Men with chronic scrotal pain reproducible by Valsalva and not explained by another cause. About 50-70% of these men get pain relief from surgery — not guaranteed, but the only reliable intervention.
If you do not fit one of these scenarios, observation is the right answer. A palpable varicocele with normal semen parameters in a man with no fertility goals does not need to be removed.
Microsurgical, Laparoscopic, or Embolization — Which Approach Wins
The technique you get matters more than most patients are told. There are four mainstream options, and they are not equivalent.
Microsurgical subinguinal varicocelectomy is the gold standard endorsed by the AUA-ASRM 2024 guideline[1] and the EAU Male Infertility Guidelines 2024[3]. A small incision is made below the external inguinal ring, the spermatic cord is delivered, and under an operating microscope or high-magnification loupes the surgeon individually identifies and ligates every internal spermatic vein while preserving the testicular artery and lymphatics. Recurrence rates are 1-2%. Hydrocele formation (the most common complication) drops to under 1% because lymphatics are spared. Testicular artery injury — which can cause atrophy — is essentially eliminated.
Laparoscopic varicocelectomy uses three abdominal ports to access the spermatic vessels above the inguinal ring. It is faster to learn than microsurgery but has higher recurrence (4-15%) and a 7-12% hydrocele rate because lymphatics are harder to preserve at that anatomical level. It carries general anesthesia risk and rare but serious complications including bowel and vascular injury.
Open retroperitoneal approaches (Palomo, Ivanissevich) are the traditional techniques. They work, but recurrence rates run 5-15% and hydrocele rates 3-30% depending on whether the surgeon attempts artery and lymphatic preservation. Their main appeal today is that they don’t require microsurgical training or laparoscopic equipment — which means they remain common in resource-limited settings.
Percutaneous embolization is performed by an interventional radiologist through a femoral or jugular vein. Coils or sclerosant block the internal spermatic vein. No incision, faster recovery, but recurrence rates 4-11% and a small risk of coil migration. Useful in patients who decline surgery, have had failed prior surgery, or need bilateral treatment in a single setting.
The practical recommendation: if you qualify for surgery and have access to a microsurgically trained urologist, that is the technique to ask for. The lower recurrence and complication profile is not subtle — it is the reason every major guideline body names microsurgery as the preferred technique.
Trying to conceive and unsure if surgery is the right next step?
Enter your email below to receive Dr. Khalid’s complete Evidence-Based ED & Male Fertility Action Plan as a free, printable PDF — covers when to test, when to treat, and when to wait.
What the Numbers Actually Show After Varicocele Surgery
Patients want to know two things: will my sperm count improve, and will my partner get pregnant. The honest answers, drawn from pooled trial data:
Semen parameter improvement is real but modest. Across meta-analyses, sperm concentration rises by an average of 9-12 million per milliliter, total motility by 10-12 percentage points, and morphology by 3-5 percentage points[4]. DNA fragmentation index — increasingly seen as the most fertility-relevant single measurement — drops by about 8-12 percentage points. These changes peak at 6 months post-operatively, which is why no honest urologist will tell you the operation failed at 3 months.
Spontaneous pregnancy rates are the outcome that matters clinically. The Cochrane Review on varicocelectomy for infertility, updated in 2021, found a statistically significant benefit: pregnancy rate at 12 months of roughly 33-37% in surgical groups versus 15-17% in observation groups[5]. That is a doubling of the spontaneous conception rate — not a guarantee, but a meaningful shift.
What surgery cannot do: it cannot create sperm where there are none. Men with non-obstructive azoospermia (zero sperm in the ejaculate) and a varicocele are a special case. Roughly 30-50% will have sperm reappear in the ejaculate after surgery, sometimes enough to attempt natural conception, more often enough to retrieve sperm without a testicular biopsy[2]. The decision in azoospermia cases is made with a fertility specialist alongside the urologist.
When IVF/ICSI is already planned: the data are mixed, but two trends are emerging. First, varicocele surgery before IVF improves live-birth rates in couples with severe oligospermia[4]. Second, it reduces sperm DNA fragmentation, which appears to lower miscarriage rates after ICSI. If you and your partner are starting an IVF cycle, the question of whether to fix the varicocele first is worth asking specifically.
What Recovery Actually Looks Like
Varicocelectomy is a day-case procedure. You go home the same day with a small scrotal support and oral analgesia. The expected timeline:
- Day 1-3: Ice packs for 20 minutes every 2 hours while awake. Scrotal support around the clock. Most men need acetaminophen plus a short course of ibuprofen; opioids are rarely required. Expect bruising and mild swelling — this is normal and not a complication.
- Day 4-7: Return to desk work, walking, light household activity. Driving once you can perform an emergency stop without flinching — usually around day 5-7.
- Week 2: Resume gentle exercise. Avoid heavy lifting (above 10 kg / 22 lb) and impact sports.
- Week 4-6: Full exercise including running and weight training. Intercourse is safe from week 4.
- Month 3: First post-operative semen analysis. Don’t be alarmed if numbers haven’t improved yet — sperm produced today reflects testicular conditions 70-90 days ago.
- Month 6: Peak semen parameter improvement is measured here. This is the reading that tells you whether the surgery worked.
- Month 12: Pregnancy outcome window. If spontaneous conception has not occurred by 12 months post-surgery with optimized semen parameters, escalate to fertility specialist evaluation.
Complications are uncommon but worth knowing about. Hydrocele (fluid collection around the testis) develops in 1-5% of patients depending on technique — lower with microsurgery, higher with open Palomo. Testicular atrophy from inadvertent artery ligation occurs in less than 0.5% of microsurgical cases. Recurrence (varicocele returning) is 1-2% with microsurgery, higher with other techniques. Wound infection is rare given the clean groin/scrotal field. Bowel or vascular injury is essentially confined to laparoscopic approaches.
When a Varicocele Is a Red Flag, Not Just a Nuisance
Most varicoceles are benign and longstanding. A few are not. The pattern that should send you to a urologist within days, not weeks:
Red Flags — Get Seen Within Days
- Sudden onset of a new varicocele after age 40, particularly if it appeared over weeks rather than years.
- Right-sided varicocele only, with no left-sided varicocele present. Because of the anatomy described earlier, isolated right-sided varicoceles are uncommon and can indicate compression of the right testicular vein or inferior vena cava by a retroperitoneal mass.
- Varicocele that does not decompress when you lie down. A normal varicocele empties when supine because gravity is no longer driving the reflux. One that stays full while supine suggests obstruction further upstream.
- Associated abdominal pain, weight loss, hematuria (blood in urine), or palpable abdominal mass.
These features collectively raise the question of a renal tumor, retroperitoneal lymphadenopathy, or another mass effect on the testicular venous drainage. The workup is a CT scan of the abdomen and pelvis with contrast, plus age-appropriate cancer screening including a careful testicular exam to rule out a testicular primary.
What to ask your primary care doctor or urologist if you fit this pattern: request a contrast-enhanced CT abdomen and pelvis within two weeks, and a scrotal ultrasound with Doppler to characterize the venous flow and rule out a testicular mass. If you also have blood in your urine, that combination raises the urgency further.
The good news: the vast majority of varicoceles are not red flags. The pattern matters — slow, longstanding, left-sided, decompresses lying down — and that pattern is reassuring. A new, right-sided, or non-decompressing varicocele is the one that needs imaging this week. For broader men’s screening context, the Men’s Wellness Hub covers the full age-appropriate workup.
Frequently Asked Questions
Will varicocele surgery guarantee my partner gets pregnant?
No. Varicocele surgery roughly doubles the spontaneous pregnancy rate at 12 months — from about 15-17% with observation to 33-37% with surgery — but it is not a guarantee. Surgery improves the underlying sperm quality; conception still requires a healthy female reproductive system and time. If your partner has unevaluated fertility factors, address those in parallel. Our Semen Analysis Interpreter helps clarify whether your numbers fit the profile most likely to benefit.
I have a varicocele but my semen analysis is normal — should I still have surgery?
No. The AUA-ASRM 2024 guideline does not recommend varicocele surgery in men with normal semen parameters who are not actively trying to conceive and have no scrotal pain. A palpable varicocele alone is not an indication for an operation. Observation with periodic semen analysis if you plan future fertility is the appropriate approach. The exception is adolescent boys with significant testicular size discrepancy, who may benefit from early surgery to preserve future spermatogenic potential.
How long after varicocele surgery should we wait before trying to conceive?
Intercourse is medically safe from about week 4 after surgery, but the meaningful improvement in sperm quality takes longer. Sperm produced today reflects testicular conditions from roughly 70-90 days ago, so the first informative post-operative semen analysis is at month 3, and peak improvement is at month 6. Most couples continue trying naturally for 12 months post-surgery before considering escalation. If you are over 35 or your partner is over 35, that timeline tightens — talk to a fertility specialist alongside your urologist.
Is microsurgical varicocelectomy worth the extra cost compared with laparoscopic surgery?
In most cases, yes. Microsurgical varicocelectomy has a recurrence rate of 1-2% versus 4-15% for laparoscopic, plus a hydrocele rate under 1% versus 7-12% laparoscopic. Both guidelines bodies (AUA-ASRM 2024 and EAU 2024) name microsurgery as the preferred technique. If insurance or cost makes microsurgery inaccessible, embolization is a reasonable alternative with similar efficacy, though slightly higher recurrence.
Can a varicocele lower my testosterone level?
Yes, in a meaningful subset of men. Varicocelectomy raises serum testosterone by an average of roughly 100 ng/dL in men whose pre-operative levels were below 400 ng/dL. The mechanism is the same temperature and oxidative-stress damage that affects sperm production, applied to the Leydig cells that produce testosterone. If you have a palpable varicocele plus symptoms of low testosterone — fatigue, low libido, mood changes — the Low Testosterone Symptom Quiz can clarify whether your symptom pattern fits, and a serum testosterone is a reasonable next step.
What does varicocele surgery actually cost in the United States?
Out-of-pocket costs for varicocele surgery in the US range widely. With insurance coverage for infertility indications, copays typically run $500-2,500. Cash-pay costs for microsurgical varicocelectomy at most US urology centers are $4,000-10,000 including facility and anesthesia. Embolization is often slightly less expensive. Many insurance plans require documented 12-month infertility plus an abnormal semen analysis before approving surgery — which aligns with the AUA-ASRM 2024 criteria anyway.
References
- American Urological Association & American Society for Reproductive Medicine. Diagnosis and Treatment of Infertility in Men: AUA/ASRM Guideline. J Urol. 2024;211(1):65-77. AUA Guideline
- Esteves SC, Miyaoka R, Roque M, Agarwal A. Outcome of varicocele repair in men with nonobstructive azoospermia: systematic review and meta-analysis. Asian J Androl. 2016;18(2):246-253. PubMed
- European Association of Urology. EAU Guidelines on Sexual and Reproductive Health. Edn. presented at the EAU Annual Congress 2024. EAU Guidelines
- Birowo P, Rahendra Wijaya J, Atmoko W, Rasyid N. The effects of varicocelectomy on the DNA fragmentation index and other sperm parameters: a meta-analysis. Basic Clin Androl. 2020;30:15. PubMed
- Persad E, O’Loughlin CA, Kaur S, et al. Surgical or radiological treatment for varicoceles in subfertile men. Cochrane Database Syst Rev. 2021;4(4):CD000479. Cochrane
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.