Kidney Stone Stent Pain: What Nobody Warns You About
Most patients wake up from stone surgery thinking the worst part is over, only to panic when they start peeing blood and feeling a deep ache in their kidney. They think something has gone terribly wrong. The reality is, your surgery went fine—but nobody properly warned you about the ureteral stent they left behind. Here is the honest truth about why your stent hurts, how to tell normal discomfort from a true medical red flag, and how to manage the pain today.

If you are reading this with a kidney stone stent inside you right now, you are almost certainly uncomfortable, slightly alarmed, and wondering whether what you are feeling is normal. Let me answer that directly: kidney stone stent pain is one of the most under-discussed parts of stone surgery, and the symptoms you are experiencing — urgency, a deep ache when you urinate, blood-tinged urine, a low-grade pulling sensation in your flank — are almost always expected, predictable, and manageable. Roughly 80% of patients with a ureteric stent develop some symptoms, and the AUA describes stent-related discomfort as the single most common patient complaint after stone surgery [1]. This article walks through exactly what your stent is doing inside you, why it hurts, what is normal versus what is a red flag, and what you can actually do about it today.
Key Takeaways
- Around 80% of patients with a ureteric stent develop bothersome symptoms — urgency, flank pain on voiding, and hematuria are the three most common, and all are expected.
- Stent pain peaks in the first 48-72 hours after insertion, then plateaus until removal — it rarely gets progressively worse without an underlying complication.
- Tamsulosin 0.4 mg daily reduces stent symptom severity by roughly 30-40% and is the single most evidence-based intervention.
- Fever above 38.5°C, rigors, inability to urinate, or a visible stent at the urethral opening require same-day urology contact or ER attendance.
What a Ureteric Stent Actually Is — And Why You Have One
A ureteric stent — properly called a double-J or pigtail stent — is a soft, hollow silicone tube about 22-30 cm long and roughly the diameter of a thin pencil lead. One coiled end (the “J”) sits inside your kidney’s collecting system. The other coiled end sits inside your bladder. The shaft runs through your ureter, the muscular tube that carries urine from kidney to bladder. The stent holds the ureter open and lets urine drain past any swelling, stone fragments, or surgical inflammation.
Your urologist placed it for one of four reasons: (1) after a ureteroscopy or laser lithotripsy to keep the ureter open while it heals from the instrument trauma, (2) after a PCNL to protect the upper tract during drainage, (3) before stone surgery to passively dilate the ureter so the scope can fit, or (4) as an emergency drainage measure for an obstructed, infected kidney. If you want a fuller picture of how stents fit into the larger stone surgery pathway, the kidney stone surgery comparison guide walks through where each procedure uses one.
The standard dwell time is 1-2 weeks for routine post-ureteroscopy stents, sometimes longer if the ureter was badly injured or if you are waiting for definitive stone surgery. Anything beyond 4-6 weeks risks encrustation — calcium deposits forming on the stent surface — which is why removal timing is non-negotiable.
Why Your Stent Hurts: The Three Mechanisms
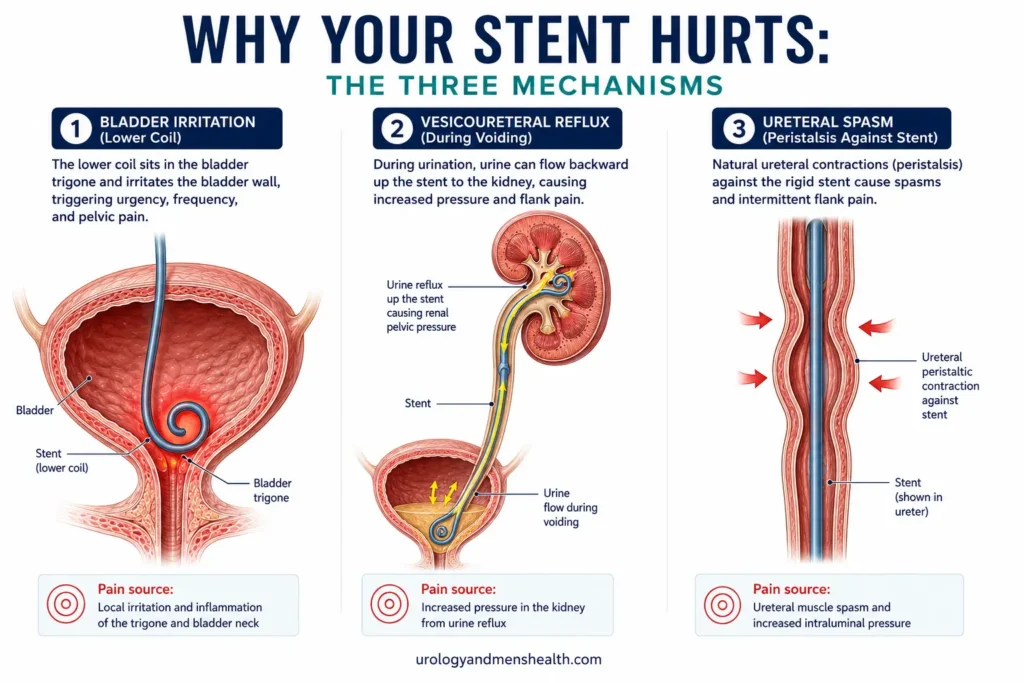
Stent pain is not one sensation. It is three distinct mechanisms producing three different symptom patterns, and understanding which is which helps you target the right management.
1. Bladder Coil Trigone Irritation
The lower coil of your stent sits inside your bladder, resting against the trigone — the triangular area at the bladder base that is densely packed with stretch receptors. Every time your bladder fills and empties, that coil rubs the trigone. This produces the classic stent triad of urinary urgency, frequency, and that uniquely uncomfortable sensation of needing to urinate immediately after you just did. It feels like a UTI, but it is mechanical, not infectious. This symptom usually accounts for around 60-70% of the day-to-day discomfort patients describe.
2. Vesicoureteric Reflux on Voiding
Normally, the ureter has a one-way valve where it enters the bladder. Your stent props that valve open. When you urinate, the high pressure inside your contracting bladder pushes urine backward up the stent and into your kidney. The result: a sharp pulling or stabbing pain in your flank on the same side as the stent, every time you void. This is the symptom that frightens patients most because it feels exactly like the kidney pain that brought them to surgery in the first place. It is not the stone. It is reflux. It stops the moment the stent comes out.
3. Ureteral Peristalsis Against a Rigid Tube
Your ureter is a muscular tube that squeezes rhythmically to push urine downward. With a stent in place, the ureter is contracting against a rigid object. This produces a deeper, lower-grade aching sensation along the path of the ureter — often described as a dull pulling between the kidney and the groin, intermittent rather than constant. It is the symptom most responsive to alpha-blockers like tamsulosin.
In My Practice
I had a patient last year — a 38-year-old engineer, very fit, low pain tolerance only in the sense that he was extremely vigilant about anything feeling “wrong” with his body. Three days after a routine ureteroscopy for a 7 mm stone, he called the on-call line convinced he had developed a second stone in the same kidney. The pain on voiding was identical to his original colic. He had not been warned about reflux.
Most stent symptoms are not complications — they are predictable physiology that nobody bothered to explain in the discharge summary, and the gap between expectation and reality is where the panic lives.
The Symptom Timeline: What to Expect Day by Day
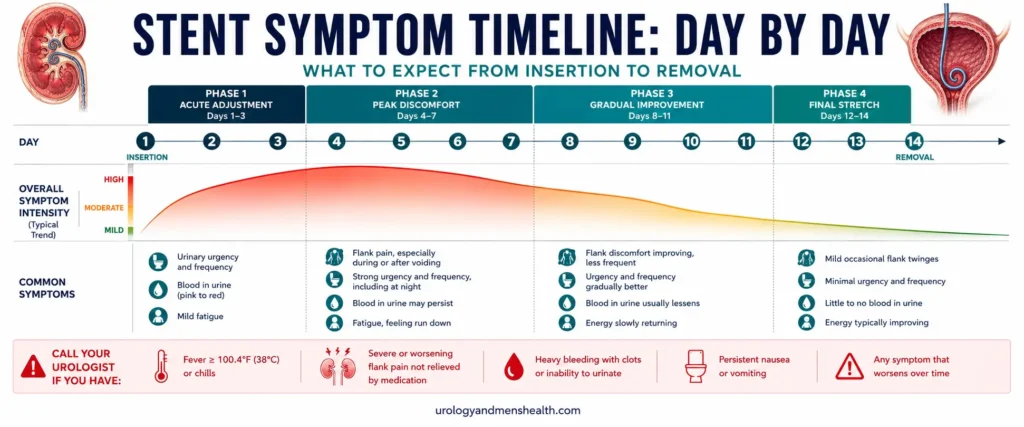
Stent symptoms follow a predictable arc. Knowing the curve helps you tell whether what you are feeling is on-track or off-track.
- Day 1 (insertion day): Mild burning on urination, pink-tinged urine, some general post-anesthetic grogginess. Pain at the surgical site dominates over stent symptoms.
- Days 2-3: Peak stent symptoms. Urgency, frequency, flank pain on voiding all reach maximum intensity. Hematuria is common and can look alarming. This is when most patients call the urology office.
- Days 4-7: Plateau. Symptoms persist at a manageable but bothersome level. Most patients can return to desk-based work by day 5-7.
- Days 7-14: Symptoms remain steady. Hematuria becomes intermittent — typically triggered by physical activity, straining, or constipation. Some patients adapt psychologically and rate the same symptom intensity as less bothersome simply because it has become familiar.
- Removal day: The procedure itself takes 30 seconds in clinic via flexible cystoscopy. Mild burning for 24 hours afterward, then resolution. Symptoms typically clear within 48 hours of removal.
The key pattern: symptoms should plateau or improve, not progressively worsen. A stent that was tolerable on day 3 and is unbearable on day 6 is a stent that needs a phone call to your urologist.
Managing Stent Pain: The Layered Approach
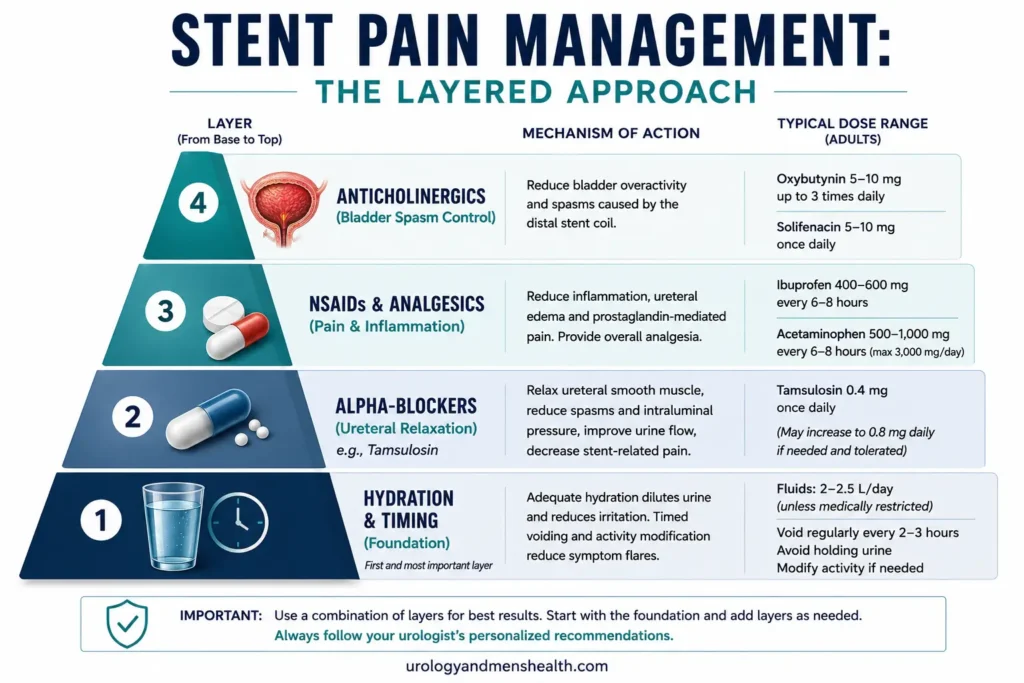
There is no single drug that eliminates stent pain. Effective management means layering interventions that each target a different mechanism.
Layer 1: Hydration and Voiding Timing
Drink enough that your urine is consistently pale straw — roughly 2.5-3 liters daily (around 85-100 fl oz). Concentrated urine irritates an already inflamed bladder and worsens every stent symptom. Do not, however, gulp 500 mL all at once and then hold it. Frequent small sips are far better than infrequent large ones. The hydration calculator gives a personalized daily target based on body weight and climate.
When you feel the urge to urinate, void promptly. Holding makes reflux worse because a full bladder generates higher pressure on emptying. Many patients also find that leaning slightly forward when voiding reduces flank pain.
Layer 2: Alpha-Blockers
Tamsulosin 0.4 mg once daily (or alfuzosin 10 mg) is the most evidence-based pharmacological intervention. A 2023 meta-analysis of 14 randomised trials showed alpha-blockers reduced stent symptom severity scores by roughly 30-40% and reduced analgesic use by a similar margin [2]. Side effects are mild — orthostatic dizziness in some, retrograde ejaculation in roughly 15% of men (resolves on stopping). Most urologists prescribe this routinely; if yours did not, it is worth asking. For more detail on tamsulosin’s wider use and side effect profile, see the tamsulosin side effects guide.
Layer 3: NSAIDs and Analgesia
Ibuprofen 400 mg three times daily with food, or diclofenac 50 mg three times daily if your kidney function allows, is the analgesic backbone. NSAIDs work better than paracetamol/acetaminophen alone for stent pain because the dominant mechanism is inflammatory. The caveat: NSAIDs reduce renal blood flow, so avoid them if you have CKD, a single functioning kidney, or were given specific instructions to avoid them. Paracetamol 1 g four times daily is the safer alternative in those situations. Short courses of weak opioids (codeine, tramadol) are reasonable for breakthrough pain in the first 48 hours but should not be a primary strategy.
Worried about stone recurrence after your stent comes out? Download Dr. Khalid’s 7-Day Kidney Stone Prevention Meal Plan.
Enter your email below to receive Dr. Khalid’s complete 7-Day Kidney Stone Prevention Meal Plan as a free, printable PDF.
Layer 4: Anticholinergics for Bladder Spasm
If urgency and frequency are the dominant symptoms, an anticholinergic — solifenacin 5 mg daily or oxybutynin 5 mg twice daily — can help. These drugs relax the bladder muscle and reduce the spasms triggered by trigone irritation. Beta-3 agonists like mirabegron 50 mg daily are an alternative with fewer dry-mouth side effects. These are not first-line for everyone but are useful when alpha-blockers and NSAIDs leave urgency untouched. Discuss with your urologist before starting.
Hematuria: What’s Normal and What Isn’t
Almost every patient with a stent has visible blood in their urine at some point during the dwell. The mechanism is simple: a foreign body rubbing against vascular bladder and ureteric mucosa produces minor bleeding, which becomes visible the moment it dilutes into urine. A small volume of blood — perhaps 1-2 mL — can turn 200 mL of urine alarmingly pink.
- Normal hematuria: Pink, rose, or light red urine that comes and goes. Often worse after exercise, straining at stool, or a long car drive. Clears with hydration.
- Borderline — call your urologist: Dark red urine that persists despite hydration, urine that becomes progressively darker rather than lighter over 24 hours, or pinkness that returns reliably with any minor exertion after the first week.
- Red flag — same-day urology contact or ER: Frank, dark-red urine with visible clots, urine the colour of cola, or any difficulty starting to urinate suggesting clot retention.
For a broader breakdown of what different urine colours mean and when each warrants investigation, see the hematuria causes guide — though in the specific context of a fresh stent, the differential is much narrower.
When Stent Pain Becomes an Emergency
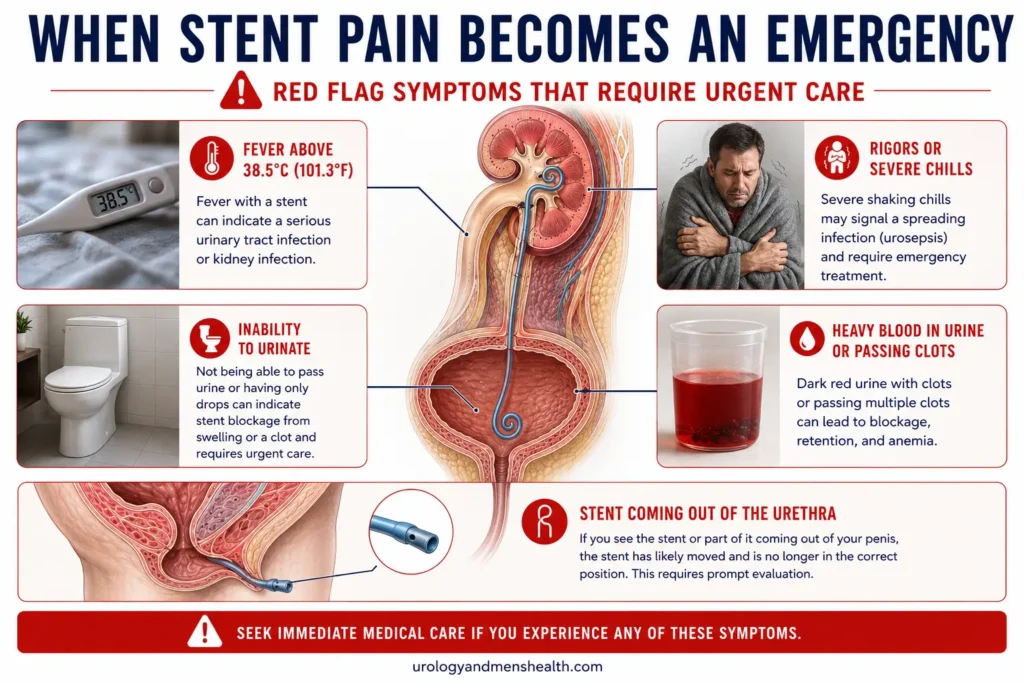
The vast majority of stent symptoms are bothersome but benign. A small subset are not. Knowing which is which prevents both unnecessary ER visits and dangerous delays.
Red Flags: Contact Your Urologist Same-Day or Go to the ER
- Fever above 38.5°C (101.3°F), shaking chills, or rigors — suggests stent-related pyelonephritis, which can progress to sepsis within hours. Do not wait until morning.
- Complete inability to urinate for more than 6-8 hours despite a full bladder — suggests clot retention or stent malposition obstructing the bladder neck.
- The stent visible at the urethral opening — the stent has migrated downward. This needs urology review the same day to assess whether reinsertion is needed.
- Severe, escalating flank pain that does not settle with usual analgesia — suggests the stent may have moved, obstructed, or become blocked by clot or debris.
- Frank red urine with visible clots and difficulty voiding — clot retention is a urological emergency requiring bladder washout.
- Persistent vomiting preventing oral intake or medication — risks dehydration and inability to take antibiotics if infection develops.
If you are unsure, the safer call is always to contact your urology team. Stent-related sepsis is the one complication that costs hours, not days, and it is the single thing I want patients to over-react to rather than under-react to.
Sex, Exercise, and Daily Life with a Stent
The everyday questions patients ask but rarely get answered in clinic:
- Driving: Fine from day 2-3 if you are off opioids and your pain is controlled enough that you could perform an emergency stop. Long drives worsen hematuria.
- Work: Desk-based work is usually feasible from day 5-7. Heavy manual work should wait until after stent removal.
- Exercise: Gentle walking from day 1. Avoid running, cycling, and weight lifting until after stent removal — these all worsen hematuria and bladder irritation. Swimming is reasonable from day 7 if there is no fever or significant bleeding.
- Sex: Penetrative sex is physically safe but often uncomfortable due to bladder irritation. Most men experience some mild burning during ejaculation. No medical reason to abstain, but most patients naturally choose to wait until the stent is out.
- Alcohol: Avoid in the first 48 hours because of anaesthetic clearance and analgesic interactions. After that, in moderation. Alcohol worsens dehydration, which worsens every stent symptom.
- Flying: Most patients can fly from day 3-5 if their pain is controlled. Hydrate aggressively and walk every 1-2 hours. Carry your discharge summary and the urologist’s contact details in case of overseas problems.
Stent Removal: What Actually Happens
The single most common question patients ask me about stent removal is whether it hurts. The honest answer: the procedure itself is uncomfortable but brief — typically 20-30 seconds — and most patients rate it 3-5 out of 10 on the pain scale. Far less than the stent itself has been causing.
Standard removal happens in clinic under local anaesthetic gel using a flexible cystoscope. The cystoscope passes through the urethra into the bladder, the stent’s lower coil is grasped with forceps, and the entire stent is withdrawn in one smooth pull. You may feel a brief pulling sensation along your flank as the upper coil straightens and exits the kidney. No catheter is needed afterward.
For 24 hours after removal, expect mild burning on urination, possibly some pink urine, and occasionally a brief episode of flank ache as the ureter recovers its normal peristalsis. By 48 hours, the vast majority of patients feel substantially better than they did with the stent in. If you still have any fragments to pass, the kidney stone passage calculator can give you a realistic timeframe based on stone size and location.
Related: How to Pass a Kidney Stone Fast — Evidence-Based Strategies ➔Frequently Asked Questions
How long does kidney stone stent pain last?
Symptoms typically peak at 48-72 hours after insertion, then plateau at a manageable level until removal. The vast majority of patients have full resolution within 48 hours of the stent coming out. If your discomfort is worsening rather than plateauing after day 4, contact your urologist — a progressive worsening pattern is not the expected stent course and may indicate displacement, blockage, or infection. For broader context on the recovery arc after stone surgery, the stone surgery comparison guide covers each procedure’s recovery profile.
Why do I get a sharp pain in my kidney every time I urinate?
This is vesicoureteric reflux: when you urinate, the high pressure in your contracting bladder pushes urine backward up the stent and into your kidney, irritating the renal pelvis. It feels exactly like the original stone pain, which alarms most patients. It is mechanical, not infectious, and disappears immediately when the stent is removed. Leaning slightly forward when voiding and avoiding holding a full bladder both reduce its severity.
Is blood in my urine with a stent dangerous?
Visible hematuria — pink or light red urine — affects almost every stent patient at some point and is rarely dangerous. It results from the stent rubbing against bladder and ureteric mucosa. The red flags are: frank dark-red urine with visible clots, urine the colour of cola, or any difficulty voiding suggesting clot retention. Those require same-day urology contact or ER assessment. Steady mild pinkness that responds to hydration does not.
Can I take tamsulosin if my urologist didn’t prescribe it?
You should ask before starting any new medication, but tamsulosin 0.4 mg daily is so consistently used for stent symptoms that most urologists will prescribe it on request. A meta-analysis of 14 randomised trials showed it reduced stent symptom severity by roughly 30-40%. The main side effects are mild dizziness on standing and, in men, retrograde ejaculation in around 15% of patients — both reversible on stopping the drug.
What happens if my stent is left in too long?
Stents left beyond their recommended dwell time — typically 4-6 weeks for routine stents, longer in specific clinical situations — begin to encrust with calcium deposits. A severely encrusted stent becomes difficult to remove and may require formal endoscopic surgery rather than a simple clinic cystoscopy. If you have lost track of when your stent was placed, contact your urology team immediately. Forgotten stents are one of the few genuinely preventable causes of major urological complications.
Does the stent removal procedure require anaesthesia?
Standard stent removal happens in clinic under local anaesthetic gel only — no general anaesthesia and no sedation. The procedure takes 20-30 seconds using a flexible cystoscope. Most patients rate the discomfort 3-5 out of 10. Encrusted stents, stents with damaged retrieval strings, or patients with anatomical difficulties may require theatre-based removal under spinal or general anaesthesia, but this is the exception.
References
- Joshi HB, Stainthorpe A, MacDonagh RP, et al. Indwelling ureteral stents: evaluation of symptoms, quality of life and utility. Journal of Urology. 2003;169(3):1065-1069. AUA Journal
- Zhou L, Cai X, Li H, Wang KJ. Effects of α-blockers, antimuscarinics, or combination therapy in relieving ureteral stent-related symptoms: a meta-analysis. Journal of Endourology. 2015;29(6):650-656. PubMed
- Assimos D, Krambeck A, Miller NL, et al. Surgical Management of Stones: American Urological Association/Endourological Society Guideline. American Urological Association. 2024 update. AUA Guidelines
- EAU Guidelines on Urolithiasis. European Association of Urology. 2024. EAU
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.