Premature Ejaculation: Why It Happens & What Works
Stop relying on willpower. Understand the biology of premature ejaculation and explore a full ladder of proven treatments that actually work.

Most men who come to me about premature ejaculation have already spent years thinking they’re broken, weak, or just bad in bed. They are none of those things. Premature ejaculation is the most common male sexual dysfunction worldwide — affecting roughly 1 in 3 men at some point — and it is a medical condition with a defined neurobiology, a clinical diagnosis, and treatments that genuinely work. The problem is that almost nobody is told this. Men try to “last longer” through willpower and shame, then quietly give up. In this guide I want to walk you through what premature ejaculation actually is, why it happens (lifelong PE and acquired PE are different conditions with different fixes), how a urologist diagnoses it, and the full treatment ladder — from behavioral techniques to SSRIs to topical sprays. For a wider overview of male sexual function, you can also see our complete Sexual Health Hub.
Key Takeaways
- The AUA/SMSNA 2020 guideline defines lifelong premature ejaculation as ejaculation within about 2 minutes of penetration, present since sexual debut, with poor control and distress.
- Lifelong PE is largely neurobiological — daily SSRIs work in roughly 60-80% of men, with IELT improvements typically 3-8x baseline within 4-6 weeks.
- Acquired PE almost always has a treatable cause underneath: ED, anxiety, prostatitis, or thyroid disease. Treat the cause first; the PE often resolves with it.
- Topical lidocaine-prilocaine spray is the most underused first-line option in the US — it works in days, not weeks, and has minimal systemic side effects.
- If your IELT is under 2 minutes and bothering you, a urologist visit is appropriate. This is treatable, and you don’t need to live with it.
What Premature Ejaculation Actually Is (and Isn’t)
The first thing I tell patients is that premature ejaculation is a clinical diagnosis, not a self-judgment. The American Urological Association and the Sexual Medicine Society of North America jointly published the most rigorous current definition in 2020, and it has three components that all must be present [1].
First, poor ejaculatory control — you cannot meaningfully delay ejaculation once you want to. Second, associated bother — it distresses you, your partner, or both. Third, ejaculation within about 2 minutes of vaginal penetration for lifelong PE, or a markedly reduced ejaculatory latency time (IELT) compared with your prior baseline for acquired PE. Without all three, the label doesn’t apply.
That 2-minute threshold matters because the 2020 guideline extended it from the older 1-minute cutoff. The reason is that men with an IELT between 1 and 2 minutes are clinically more similar to PE patients than to men without it — they share the same distress, the same partner dissatisfaction, and respond to the same treatments [1].
Here is what PE is not. It is not “sometimes finishing quickly when you’re excited.” It is not “finishing in 5 minutes” if neither you nor your partner is bothered. It is not a sign that you don’t love your partner. And it is not a moral failing or a sign of weak masculinity — a phrase I unfortunately hear from patients more often than I should.
Lifelong vs. Acquired Premature Ejaculation: Why The Distinction Matters
This is the most clinically useful split, and most men don’t know it exists. Whether your PE is lifelong or acquired completely changes what’s causing it and what will fix it.
Lifelong (Primary) PE
This means you’ve had it since your first sexual experiences. You’ve never had a “normal” baseline. The best current evidence suggests lifelong PE is largely neurobiological — a difference in how the serotonin system regulates the ejaculation reflex. The original work by Marcel Waldinger and colleagues in the 1990s established that lifelong PE clusters in families and responds powerfully to drugs that raise central serotonin (SSRIs) [2]. There may also be genetic variation in the serotonin 5-HT1A and 5-HT2C receptors.
Practically, this means lifelong PE rarely responds to “just relax” advice or short-term behavioral techniques alone. The wiring is the wiring. SSRIs, topical anesthetics, and combination therapy are the proven routes.
Acquired (Secondary) PE
This is the one that catches men in their 30s, 40s, and beyond. You had normal ejaculatory control for years, and then it changed. Acquired PE almost always has an underlying driver, and finding it is half the treatment. The most common ones I look for in clinic are:
- Erectile dysfunction — when a man senses he’s losing his erection, he rushes to finish before it goes away. This is so common that I always screen for ED first in any acquired PE case. See our guide on ED and heart disease to understand the vascular link.
- Performance anxiety — particularly with new partners or after a prior bad experience.
- Chronic prostatitis / CPPS — pelvic floor hypertonicity and prostatic inflammation can shorten the reflex arc. See our piece on chronic prostatitis and pelvic pain syndrome.
- Hyperthyroidism — overactive thyroid measurably shortens IELT in a non-trivial subset of men. A simple TSH catches this.
- Low testosterone — less common as a driver, but worth checking, especially if libido has also fallen. Our guide to low T in men over 40 covers the symptom pattern.
- Relationship distress — not as a euphemism, but as a real physiologic stressor.
The reason the lifelong-vs-acquired split matters is this: if I put a man with hyperthyroid-driven acquired PE on daily paroxetine, I’ve masked his thyroid disease and given him sexual side effects he didn’t need. Treat the cause first. The PE usually follows.
A 37-year-old came to me last year convinced he had “broken” after his second child was born — he’d gone from 10-minute IELT to under 90 seconds over six months. He was about to start an SSRI he’d read about online. I checked a TSH on a hunch because his pulse was 96 sitting. He was frankly hyperthyroid, TSH suppressed. Three months on antithyroid medication, his IELT was back to baseline without a single sexual drug.
This is why acquired PE deserves a workup, not just a pill — the underlying cause is sometimes the easier and safer fix.
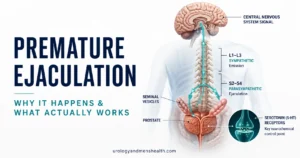
Why Premature Ejaculation Happens: The Neurobiology in Plain English
Ejaculation is a spinal reflex modulated by the brain. Think of it like a stretch reflex with a brake. The brake is largely serotonin. The more serotonin signalling you have at certain receptors in the brainstem and spinal cord, the longer the brake holds the reflex back. The less you have — or the more reactive your reflex is to a given amount of serotonin — the shorter your IELT.
This is why SSRIs work. Drugs like paroxetine, sertraline, fluoxetine, and the newer on-demand dapoxetine all raise serotonin availability at the synapse, which strengthens the brake. They were originally developed as antidepressants, and the ejaculatory delay was first noticed as a “side effect” — except that for men with lifelong PE, that side effect is the therapeutic effect.
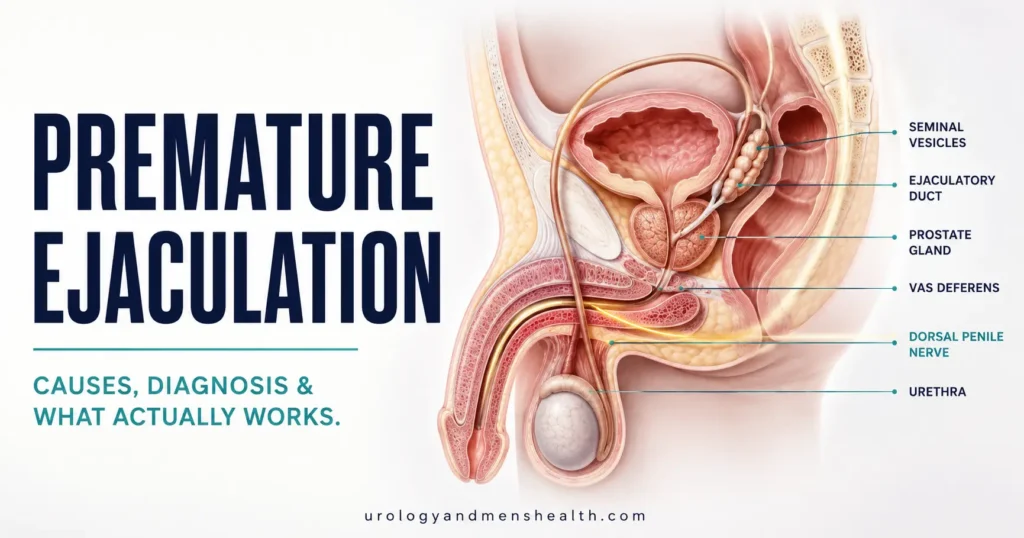
There’s also a peripheral component. The dorsal penile nerve carries sensory input from the glans. If that nerve is unusually sensitive — and there’s emerging imaging evidence that it may be hyperexcitable in some men with lifelong PE — even normal serotonin braking can be overwhelmed. This is the rationale for topical anesthetics: dampen the sensory input slightly, and the central brake holds longer.
How a Urologist Diagnoses Premature Ejaculation
Diagnosis is clinical. There is no blood test or scan that confirms PE. According to the AUA/SMSNA 2020 guideline, the diagnosis is based on medical, relationship, and sexual history plus a focused physical exam [1]. In my clinic, the visit looks like this.
First, I ask three questions: How long is your IELT — measured roughly, in seconds? Has it always been this way, or did it change? Is it distressing you, your partner, or both? Those three answers usually tell me whether we’re dealing with lifelong PE, acquired PE, or natural variation that isn’t actually pathology.
Second, I use the validated Premature Ejaculation Diagnostic Tool (PEDT) — a 5-item questionnaire that scores control, frequency, minimal stimulation, distress, and interpersonal difficulty. A score of 11 or above strongly suggests PE; 9-10 is “probable.” You can take our free PEDT assessment before your visit and bring the printable result.
Third, I screen for comorbid erectile dysfunction with the IIEF-5 (also called the SHIM). The AUA guideline is explicit: treat comorbid ED first or alongside, because the two conditions reinforce each other [1]. Our IIEF-5 self-assessment takes two minutes and will tell you whether ED is in the mix.
Fourth — and this is the part most online “PE quizzes” skip — I do a focused physical exam and check baseline labs when the story suggests acquired PE. That means a TSH (thyroid), a free testosterone if libido is low or ED is present, a urinalysis if there are urinary symptoms, and a careful prostate and pelvic floor exam if there’s pain or perineal discomfort.
Worried you have PE and don’t know what to ask your doctor?
Enter your email below to receive Dr. Khalid’s complete Evidence-Based ED Action Plan as a free, printable PDF — it covers ED, PE, and the diagnostic questions a urologist actually wants you to bring to the consultation.
Premature Ejaculation Treatment: What Actually Works
Here is the treatment ladder I use in clinic, in the order I generally try it. None of these are mutually exclusive, and combination therapy often beats monotherapy.
1. Behavioral Techniques (Free, Always First)
The two best-validated techniques are the stop-start method (Semans technique) and the squeeze technique (Masters and Johnson). Both work by repeatedly bringing arousal close to the point of inevitable ejaculation and then backing off. Over weeks, this raises the threshold. The catch: the evidence base for behavioral therapy alone is modest. A Cochrane review concluded that behavioral techniques offer some IELT improvement over no treatment, but the effect is smaller than with pharmacotherapy and harder to sustain long-term [3].
I still recommend them, especially as adjuncts. They cost nothing, have no side effects, and give a man back a sense of agency over his body — which matters psychologically as much as physiologically.
2. Pelvic Floor Muscle Training
A randomized trial by Pastore and colleagues showed that pelvic floor rehabilitation increased IELT from about 32 seconds to around 146 seconds over 12 weeks in men with lifelong PE who had not responded to other therapies [4]. That is a clinically meaningful 4-fold improvement from a free, side-effect-free intervention. I increasingly recommend pelvic floor training as a foundation, particularly for men who want to avoid medication or use the lowest possible dose.
3. Topical Anesthetics (Underused in the US)
Lidocaine-prilocaine cream or spray, applied to the glans 10-15 minutes before sex, is one of the most effective and underused options in the US market. It reduces sensory input from the dorsal penile nerve enough to delay the reflex, without crossing into systemic side effects when used correctly. The AUA/SMSNA guideline endorses topical anesthetics as a first-line option [1].
What to do: ask your urologist or primary care doctor about a lidocaine-prilocaine spray formulation specifically designed for PE (some are FDA-cleared for this use). Apply 10-15 minutes before intercourse, then wipe off any excess before contact to avoid numbing your partner. Use a condom for the first few uses while you learn your dose response.
4. Daily SSRIs (Off-Label, Highly Effective)
This is the pharmacologic backbone for moderate-to-severe lifelong PE. Paroxetine 20 mg daily, sertraline 50-100 mg daily, and fluoxetine 20 mg daily all have randomized evidence supporting IELT increases of 3-8 times baseline over 4-6 weeks [5]. In the US, all of these are prescribed off-label for PE — meaning the drug is FDA-approved (for depression), but the PE indication is supported by guideline evidence rather than FDA labeling. The AUA/SMSNA guideline explicitly endorses this practice [1].
Side effects to know: nausea (usually settles in 1-2 weeks), reduced libido in some men, occasional erectile difficulty, delayed ejaculation that overshoots (rare but real), and discontinuation syndrome if you stop abruptly. Never stop an SSRI cold — taper under medical supervision.
What to ask your urologist: “Given my IELT and PEDT score, would a 4-6 week trial of daily paroxetine 20 mg or sertraline 50 mg be appropriate, and what is your re-assessment plan at 6 weeks?” That single sentence will tell your clinician you understand what’s being offered.
5. On-Demand Dapoxetine (Where Available)
Dapoxetine is a short-acting SSRI specifically developed for PE. Taken 1-3 hours before sex, it raises IELT by roughly 2-3 fold compared with placebo, with rapid clearance from the system. It is approved in over 60 countries — but, importantly, not FDA-approved in the US. Patients in the US sometimes obtain it through other routes, which I do not endorse without proper medical oversight. If you are in the US and interested in on-demand pharmacotherapy, discuss it with a urologist. (Read more in our forthcoming piece on dapoxetine and SSRIs for PE.)
6. Treating Comorbid ED
If PE is acquired and there’s any suggestion of erectile difficulty, a PDE5 inhibitor (sildenafil, tadalafil) often improves PE as a secondary effect — because the man no longer fears losing his erection mid-act. The AUA guideline is explicit that comorbid ED should be treated according to the ED guideline as part of any PE management plan [1]. Our step-by-step ED treatment protocol walks through that pathway.
What to Track at Home Before Your Urology Visit
If you’re planning to see a urologist about PE, two weeks of basic tracking will make the visit dramatically more productive. Record:
- IELT estimates in seconds for each attempt — rough is fine, no stopwatch needed.
- Whether you achieved a satisfying erection beforehand, and whether you lost any rigidity during.
- Your morning erections — present or absent, and how rigid (a quick proxy for vascular health).
- Any new medications started in the past 6-12 months, including over-the-counter supplements.
- Sleep quality, stress level, and any major life changes in the last year.
Bring the printable result from our PEDT premature ejaculation diagnostic tool and your IIEF-5 score if available. This shaves 20 minutes off the consultation and lets your urologist focus on examining the cause rather than reconstructing the history.
When Premature Ejaculation Signals Something Else
See a urologist within 2 weeks if you have:
- Sudden onset of PE in your 30s or older with no obvious trigger — possible hyperthyroidism, prostatitis, or early ED.
- PE accompanied by pain on ejaculation, perineal pain, or pelvic discomfort — possible chronic prostatitis or CPPS.
- PE with new-onset erectile difficulty — possible early vascular disease; ask about a cardiac risk assessment.
- PE with blood in semen on more than one occasion — needs urgent evaluation regardless of other factors.
- PE with significantly reduced libido and energy — possible low testosterone or thyroid disease.
Frequently Asked Questions
What is the medical definition of premature ejaculation?
The AUA/SMSNA 2020 guideline defines lifelong premature ejaculation as poor ejaculatory control, associated bother, and ejaculation within about 2 minutes of penetration that has been present since sexual debut. Acquired PE has the same control and bother criteria but is defined by an ejaculatory latency markedly reduced from your prior baseline. Both require all three components — duration alone does not make a diagnosis. If you want a structured assessment, our PEDT diagnostic tool uses the same 5-item questionnaire urologists rely on.
Why does premature ejaculation happen at all?
Lifelong PE is largely neurobiological — a difference in how the serotonin system regulates the spinal ejaculation reflex, often with a genetic component. Acquired PE has identifiable causes: erectile dysfunction (rushing to finish before losing rigidity), chronic prostatitis, hyperthyroidism, performance anxiety, and occasionally low testosterone. The treatable cause matters enormously, which is why a urology workup catches what an internet quiz cannot.
What is the most effective treatment for premature ejaculation?
For lifelong PE, daily SSRIs (paroxetine 20 mg, sertraline 50-100 mg) are the most evidence-backed, with IELT improvements of 3-8 times baseline over 4-6 weeks. For acquired PE, treating the underlying cause is the most effective approach — fix the ED, treat the thyroid, address the prostatitis, and the PE often resolves with it. Topical lidocaine-prilocaine sprays are underused first-line options that work within days. See our full treatment ladder for sexual dysfunction for context.
Can premature ejaculation be cured permanently?
Acquired PE often resolves when the underlying cause is treated — that is a permanent fix. Lifelong PE is more like managing a chronic condition: behavioral techniques, pelvic floor training, and SSRIs or topical anesthetics can give you reliable control, but stopping treatment usually means symptoms return. The good news is that effective long-term management is genuinely available, and most men I treat reach a satisfaction level they had stopped believing was possible.
Is dapoxetine available in the United States for premature ejaculation?
No. Dapoxetine is approved in over 60 countries specifically for PE but has not received FDA approval in the United States. US-based men interested in on-demand pharmacotherapy generally use off-label daily SSRIs (paroxetine or sertraline) under urologist supervision instead. Do not source dapoxetine from unregulated online pharmacies — the dose, purity, and interactions cannot be verified.
Does watching too much pornography cause premature ejaculation?
The evidence here is weaker than the popular discourse suggests. There’s no high-quality randomized data linking pornography use directly to PE. What we do know clinically is that conditioning to rapid solo arousal patterns, combined with performance anxiety in partnered sex, can shorten IELT in some men. Reducing intensity of self-stimulation and reintroducing slower partnered patterns can help — but it’s not a cure, and most men with PE benefit from formal treatment regardless.
References
- Shindel AW, Althof SE, Carrier S, et al. Disorders of Ejaculation: An AUA/SMSNA Guideline. J Urol. 2022;207(3):504-512. AUA
- Waldinger MD, Hengeveld MW, Zwinderman AH, Olivier B. Effect of SSRI antidepressants on ejaculation: a double-blind, randomized, placebo-controlled study with fluoxetine, fluvoxamine, paroxetine, and sertraline. J Clin Psychopharmacol. 1998;18(4):274-281. PubMed
- Melnik T, Althof S, Atallah AN, Puga ME, Glina S, Riera R. Psychosocial interventions for premature ejaculation. Cochrane Database Syst Rev. 2011;(8):CD008195. Cochrane
- Pastore AL, Palleschi G, Fuschi A, et al. Pelvic muscle floor rehabilitation as a therapeutic option in lifelong premature ejaculation: long-term outcomes. Asian J Androl. 2018;20(5):442-446. PubMed
- Castiglione F, Albersen M, Hedlund P, Gratzke C, Salonia A, Giuliano F. Current pharmacological management of premature ejaculation: a systematic review and meta-analysis. Eur Urol. 2016;69(5):904-916. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.

Numbing Creams vs Pills for PE: Which Works Better?
Premature Ejaculation: Why It Happens & What Actually Works
Premature ejaculation is the most common male sexual disorder worldwide, affecting roughly 20–30% of men at some point...

GLP-1 Drugs and Male Fertility: Help or Harm?
GLP-1 Drugs and Erectile Dysfunction: What Men Should Know