Foods That Cause Kidney Stones: A Urologist’s Honest List
Most patients read an article online and immediately strip every single "kidney stone food" from their diet. The reality is, they usually cut out the wrong things while ignoring the daily deli sandwich that's actually driving the problem. Here is the honest, clinical list of what genuinely causes stones—and what you can finally stop stressing about.

Most articles about foods that cause kidney stones get the science half-right and the practical advice fully wrong. They tell you to avoid spinach and almonds, then say nothing about the slice of deli ham in your sandwich — which probably matters more. As a urologist, I see patients every week who have cut every “stone food” off their plate and still passed a third stone last month. The problem is rarely the food they’re avoiding. It’s the food they didn’t know to watch.
This guide is the honest list. It covers the dietary oxalate offenders that genuinely matter, the sodium sources that quietly drive stone formation, and the foods you’ve been told to avoid that you almost certainly don’t need to. It is built on AUA 2019 stone prevention guidelines and the NEJM dietary calcium evidence, not on internet folklore.
Key Takeaways
- About 80% of kidney stones are calcium oxalate, so dietary oxalate and sodium are the two food categories that matter most for the majority of stone formers.
- Sodium intake above 2,300 mg per day raises urinary calcium excretion and is a stronger driver of stone recurrence than dietary calcium ever was.
- Cutting dietary calcium increases stone risk, not decreases it — calcium with meals binds oxalate in the gut before it reaches the kidney.
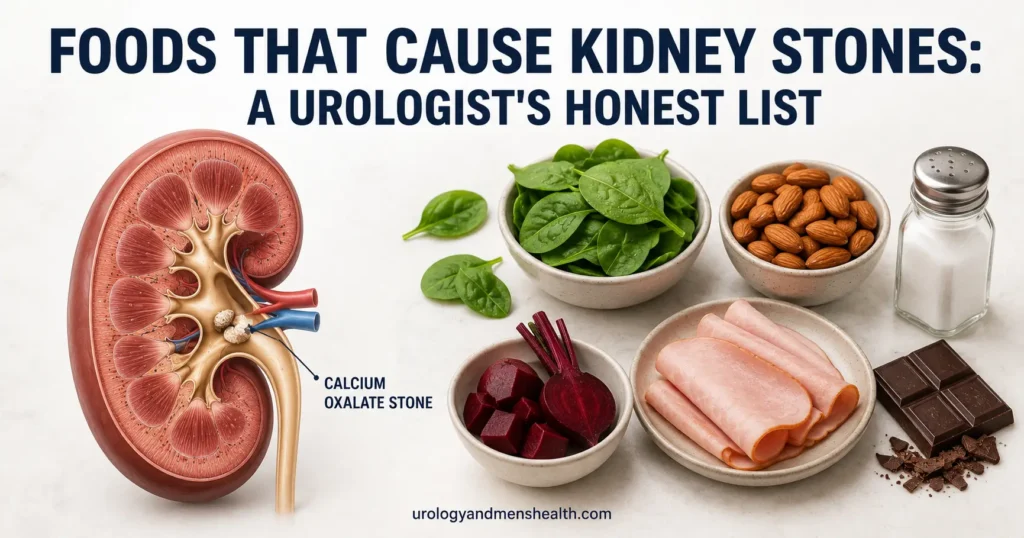
- Only six foods deliver enough oxalate to genuinely matter: spinach, rhubarb, almonds, cashews, beets, and dark chocolate. The rest of the “high-oxalate” list is largely a distraction.
- Animal protein, added sugar, and high-fructose drinks raise stone risk through separate mechanisms — not just oxalate and sodium.
Why Diet Matters for Some Stones More Than Others
Before we talk food, you need to know which stone you’re dealing with. The dietary advice that helps a calcium oxalate stone former can actively harm someone with cystine stones, and someone with uric acid stones needs an entirely different approach.
According to AUA 2019 stone prevention guidelines, the distribution of stone types in adults is roughly 75-80% calcium oxalate, 10-15% calcium phosphate, 5-10% uric acid, 1-2% struvite (infection stones), and under 1% cystine[1]. Because calcium oxalate dominates so heavily, most of this article assumes that’s what you have. If you’ve never had a stone analyzed, ask your urologist to order stone analysis on your next pass — it is the single most important data point for choosing the right diet.
For a complete breakdown by stone type, see my guide on the different types of kidney stones and how to identify yours. The rest of this article focuses on the dietary drivers of calcium oxalate stones, with notes for uric acid stones where relevant.
The Sodium Problem: The Real Driver Most People Ignore
If you remember one thing from this article, remember this: sodium is the single most powerful dietary lever for calcium oxalate stone prevention. More powerful than cutting oxalate. More powerful than cutting calcium. Yet almost nobody talks about it.
Here is the mechanism in one sentence: when your kidneys excrete excess sodium in urine, they drag calcium out with it, and that calcium then binds with whatever oxalate is in the urine to form crystals. A 24-hour urine study from the Brigham and Women’s group showed that for every 100 mmol increase in sodium intake (about 2,300 mg), urinary calcium excretion rose by approximately 25 mg[2]. That is the equivalent of taking a calcium supplement straight into your urine.
The AUA target for stone formers is sodium below 1,500 mg per day (about 3/4 teaspoon of salt). The average American eats around 3,400 mg. That gap is where stones come from.
Where the Sodium Actually Hides
The salt shaker on your table is almost never the problem. Roughly 70% of dietary sodium in the US comes from processed and restaurant food. Here are the worst offenders by category:
- Deli meats and cured meats: a 2 oz (about 56 g) serving of ham or salami can carry 500-800 mg sodium — over a third of your daily ceiling in one sandwich layer.
- Bread and bakery items: two slices of standard bread can deliver 300-450 mg sodium. The sandwich starts at 600-800 mg before any filling.
- Canned soup and broth: a single cup of regular canned soup ranges from 700 to 1,200 mg sodium.
- Restaurant meals: a typical sit-down restaurant entree carries 1,500-2,800 mg sodium in one plate. One restaurant dinner can blow the daily target.
- Condiments: soy sauce 900 mg per tablespoon, ketchup 150-200 mg per tablespoon, salad dressings 150-400 mg per 2 tablespoons.
- Frozen meals: 700-1,400 mg sodium per “single serving” tray. The “lite” versions average 600 mg.
In My Practice
I had a patient last year — 52, recurrent calcium oxalate stones, third episode in four years — who had read every diet article online and was eating no spinach, no almonds, no chocolate. He brought me a food diary on his second visit. He was eating a turkey sandwich every workday for lunch: two slices of whole-grain bread, four slices of deli turkey, a slice of cheese, mustard, pickle. By my count that was about 1,800 mg of sodium in a single sandwich. He was averaging close to 4,000 mg sodium a day and didn’t know it.
Six months after switching to a low-sodium lunch pattern — with no changes to his oxalate intake — his 24-hour urinary calcium dropped from 340 mg to 210 mg, well inside the stone-protective range. He has not formed another stone since.
The Oxalate List: The Six Foods That Actually Matter
Oxalate matters, but not nearly as much as the internet suggests. Most “high-oxalate” lists online include 30 to 60 foods, which is overwhelming and counterproductive. In clinical practice, six foods deliver enough oxalate per realistic serving to meaningfully shift your urinary oxalate. Cut these and you’ve done 90% of the work. Avoid the other 50 and you’ve made your life miserable for almost no clinical benefit.
The Six Foods Worth Genuinely Restricting
- Spinach: the single biggest oxalate offender by far — about 750 mg of oxalate per 100 g of raw spinach. One smoothie with two handfuls of spinach can deliver more oxalate than the rest of your week combined.
- Rhubarb: approximately 600-800 mg per 100 g. Less commonly eaten in the US, but if you bake with it, restrict it.
- Almonds and almond products: 120-140 mg per 1 oz (28 g). A standard handful of almonds is one of the densest single-serving oxalate sources in a Western diet.
- Cashews: 90-100 mg per 1 oz (28 g). Lower than almonds but still significant if eaten daily.
- Beets and beet greens: 500-600 mg per 100 g of beet greens, 70-150 mg per 100 g of the root.
- Dark chocolate (70%+ cacao): 110-130 mg per 1 oz (28 g). Milk chocolate is much lower, around 20-30 mg per ounce.
For a full quantified list with serving-size oxalate values, see my complete oxalate food list and calculator. The target for most stone formers per AUA guidance is keeping total dietary oxalate below 100 mg per day.
Foods Wrongly Blamed for Stones
The following frequently appear on “avoid” lists, but their oxalate content per realistic serving is moderate or low enough that restriction is rarely necessary:
- Sweet potatoes: moderate oxalate, but typical serving sizes keep total intake under 50 mg. Enjoy in moderation, just don’t eat a baked sweet potato every day.
- Tomatoes: low oxalate. Eating tomatoes daily is fine.
- Strawberries: low. Despite the internet’s confidence, strawberries are not a meaningful oxalate source.
- Bananas: very low. There is no good reason to avoid them.
- Coffee: a 12 oz cup contains around 6-10 mg oxalate. Two to three cups per day is fine and may even reduce stone risk through hydration.
- Tea (black): here the internet is closer to correct — black tea has 60-70 mg oxalate per 8 oz cup. Three or more strong cups a day starts to matter. Switch to green or herbal if you drink large amounts.
The Calcium Paradox: Why Cutting Calcium Backfires
This is the most common dietary mistake I see in stone formers, and it took the urology field decades to correct. Cutting dietary calcium increases your kidney stone risk. It does not decrease it.
The reason is mechanical. When you eat calcium with a meal that contains oxalate, the calcium binds the oxalate inside your gut and the complex is excreted in stool. The oxalate never reaches your bloodstream and never reaches your kidney. If you cut dietary calcium, that same oxalate now has nothing to bind in the gut, gets absorbed, ends up in your urine, and forms a stone.
The landmark NEJM trial by Borghi and colleagues confirmed this directly. Men with recurrent calcium oxalate stones were randomized to either a low-calcium diet or a normal-calcium, low-sodium, low-animal-protein diet. After five years, the normal-calcium group had a 51% lower recurrence rate than the low-calcium group[3]. The low-calcium diet — the intuitive answer — was actively making stones worse.
The practical rule: aim for 1,000-1,200 mg dietary calcium per day, eaten with meals, primarily from food sources (dairy, fortified plant milks, leafy greens that are not spinach). Avoid taking calcium supplements between meals — supplements taken on an empty stomach do not bind oxalate in the gut and may modestly raise stone risk.
Tired of guessing what to eat? Get Dr. Khalid’s 7-Day Kidney Stone Prevention Meal Plan
Enter your email below to receive Dr. Khalid’s complete 7-Day Kidney Stone Prevention Meal Plan as a free, printable PDF — built around the low-sodium, calcium-with-meals protocol that cuts recurrence by half.
Animal Protein, Sugar, and Fructose: The Other Three Drivers
Oxalate and sodium do most of the damage, but three other dietary patterns matter enough to address:
Animal Protein (Especially Red and Cured Meats)
High animal protein intake raises urinary calcium and uric acid while lowering urinary citrate — a triple hit for stone formation. Citrate is the body’s main natural stone inhibitor, and when it drops, calcium oxalate crystals form more easily. The AUA recommends limiting animal protein to 0.8-1.0 g per kg body weight per day for stone formers. For an 80 kg (about 176 lb) man, that’s roughly 65-80 g of meat or fish protein daily — about 8-10 oz of cooked meat total across the day. Red and cured meats raise risk more than poultry or fish.
Added Sugar and High-Fructose Drinks
Fructose, in particular, raises urinary uric acid and calcium and is independently associated with stone formation. A Harvard-led Nurses’ Health Study analysis found that women drinking one or more sugar-sweetened sodas per day had a 23% higher risk of developing a kidney stone compared to those drinking less than one per week[4]. The pattern held in men in the parallel cohort. Cut sugar-sweetened sodas, sweetened iced teas, and fruit juices with added sugar.
Inadequate Fluid Intake (The Permission Slip for Every Other Risk Factor)
No discussion of foods that cause kidney stones is complete without acknowledging that dehydration multiplies every other dietary risk. If you produce less than 2 liters of urine daily, every other intervention is working against a stacked deck. The AUA target is at least 2.5 liters of fluid intake per day (around 85 fl oz / 10 cups), with enough to produce 2+ liters of urine. See my detailed guide on hydration and kidney stone prevention for the full protocol.
A Different Diet for Uric Acid Stones
If your stone analysis came back as uric acid rather than calcium oxalate, the dietary priorities flip. Oxalate becomes largely irrelevant. The drivers are:
- Purine-rich foods: organ meats (liver, kidney), anchovies, sardines, mackerel, herring, beer, and high-yeast products raise uric acid most.
- Acidic urine pH: uric acid only crystallizes in acidic urine. Diets heavy in animal protein push urine pH down. Diets heavy in fruits and vegetables push it up.
- Alcohol, especially beer: beer is a double hit — high purines plus dehydrating effects.
For uric acid stone formers, an alkalinizing diet (Mediterranean-style, heavy in vegetables and citrus) often dissolves existing stones and prevents new ones — sometimes with medical urinary alkalinization added. Your urologist may also check fasting blood glucose, since type 2 diabetes and insulin resistance are strongly linked to uric acid stones.
When Diet Alone Isn’t Enough
Dietary changes can cut stone recurrence risk by 40-60% in adherent patients. They cannot reduce it to zero, and they cannot help everyone equally. Diet is the first step, not the only step.
See a Urologist If Any of These Apply
- You have formed two or more stones in the past five years despite dietary changes — you likely need a 24-hour urine metabolic workup and possibly medication (thiazide diuretic, potassium citrate, or allopurinol depending on findings).
- You have a single stone but a strong family history of recurrent stone disease — early metabolic workup is warranted.
- You have known cystinuria, primary hyperoxaluria, or distal renal tubular acidosis — these require specialist management beyond diet.
- Your stones are increasing in size or number on imaging despite a clean diet — ask whether you need medical therapy alongside dietary management.
- You have new flank pain, blood in your urine, or fever — see my guide on acute stone management and consider urgent assessment.
If you’ve had a stone and want to know your real recurrence risk before changing your whole diet, run the numbers first. My free Kidney Stone 5-Year Risk Profiler uses AUA-validated inputs to give you a personalized risk tier, and the Calcium-Oxalate Meal Balancer will tell you exactly how much calcium to pair with the oxalate in a given meal.
Frequently Asked Questions
What is the single worst food for kidney stones?
For calcium oxalate stone formers — which is roughly 80% of all stone patients — the single most problematic single food is raw spinach, at approximately 750 mg of oxalate per 100 g serving. One spinach smoothie can deliver more oxalate than the rest of your week’s diet combined. For uric acid stone formers, the worst single food category is organ meats, which are extremely high in purines and drive uric acid excretion. For a quantified breakdown by serving, see the full oxalate food list.
Are foods that cause kidney stones the same for everyone?
No. The foods that cause kidney stones depend entirely on your stone type. Calcium oxalate stone formers need to watch oxalate, sodium, and animal protein. Uric acid stone formers need to watch purines and urine pH. Cystine stone formers need to watch sodium and total protein. Struvite stones are infection-driven, not diet-driven. If you have never had a stone analyzed in the lab, ask your urologist to order stone analysis on your next pass — it is the single most useful data point for choosing the right diet. Learn more in my complete guide to kidney stone types.
Should I stop eating dairy if I have kidney stones?
Almost certainly not. This is the most common mistake stone formers make. Dietary calcium from dairy, eaten with meals, binds oxalate in the gut and prevents it from being absorbed and reaching the kidney. The NEJM Borghi trial showed that men with recurrent calcium stones who ate a normal-calcium, low-sodium diet had 51% fewer recurrences than men on a low-calcium diet. Aim for 1,000-1,200 mg calcium daily from food, eaten with meals. The exception is calcium supplements taken on an empty stomach, which do not bind oxalate and may modestly raise risk.
How much sodium is safe if I’m a kidney stone former?
The AUA target for active stone formers is below 1,500 mg sodium per day — roughly 3/4 of a teaspoon of salt. The average American eats around 3,400 mg daily, more than double the target. About 70% of dietary sodium comes from processed and restaurant food, not the salt shaker. The highest-yield change is reducing deli meats, bread, canned soup, restaurant meals, and condiments. Cutting sodium is the single most powerful dietary lever for calcium oxalate stone prevention — more powerful than cutting oxalate.
Does drinking lemon water actually help prevent kidney stones?
Yes, for calcium oxalate and uric acid stones, with caveats. Lemon juice contains citrate, which is the body’s main natural stone inhibitor — it binds calcium in urine before it can complex with oxalate. The mechanism is real, but the volume matters: 4 oz (about 120 ml) of fresh lemon juice per day, diluted in water, is the rough therapeutic dose used in clinical studies. A slice of lemon in your water glass will not move the needle. For full dosing protocols and which patients benefit most, see my dedicated guide on lemon water for kidney stones.
If I cut high-oxalate foods, how long before my urine oxalate drops?
Urinary oxalate responds within 24-72 hours of a dietary change. If you cut spinach, almonds, and dark chocolate on Monday, your Wednesday 24-hour urine collection will already reflect a lower oxalate output. This makes 24-hour urine studies a useful feedback tool — many of my patients do a baseline study, change their diet for two weeks, then repeat to see whether the changes are actually working. If you’ve made dietary changes and your urinary oxalate has not dropped, you are either still eating hidden oxalate sources or your gut is hyperabsorbing oxalate, which needs different management.
References
- Pearle MS, Goldfarb DS, Assimos DG, et al. Medical management of kidney stones: AUA guideline. Journal of Urology. 2014;192(2):316-324. Reaffirmed 2019. AUA Guidelines
- Taylor EN, Curhan GC. Demographic, dietary, and urinary factors and 24-h urinary calcium excretion. Clinical Journal of the American Society of Nephrology. 2009;4(12):1980-1987. PubMed
- Borghi L, Schianchi T, Meschi T, et al. Comparison of two diets for the prevention of recurrent stones in idiopathic hypercalciuria. New England Journal of Medicine. 2002;346(2):77-84. PubMed
- Ferraro PM, Taylor EN, Gambaro G, Curhan GC. Soda and other beverages and the risk of kidney stones. Clinical Journal of the American Society of Nephrology. 2013;8(8):1389-1395. PubMed
- Skolarikos A, Neisius A, Petřík A, et al. EAU Guidelines on Urolithiasis. European Association of Urology, 2024. EAU Guidelines
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.