Visible blood in urine is your body’s fire alarm — and you should never ignore it, even if it goes off only once. As a urologist, hematuria is one of the most common reasons men are referred to me, and it is also the symptom that men delay acting on most dangerously. The story I hear over and over: “I saw blood once three months ago, it went away on its own, so I assumed it was nothing.” That assumption has cost men early-stage diagnoses that would have been curable.
Every episode of visible blood in urine — even a single episode, even if painless, even if it resolves spontaneously — needs urological investigation. This is not an overreaction. It is standard clinical practice worldwide, endorsed by the American Urological Association, the European Association of Urology, and every major urological guideline body. Bladder cancer, kidney cancer, and other serious conditions can present with intermittent, painless hematuria that appears once and does not recur for weeks or months [1].
This article walks you through the seven most common causes of blood in urine in men, the investigation pathway every man needs, and the specific clinical patterns that should send you to a specialist immediately rather than wait.
Key Takeaways
- A single episode of visible blood in urine warrants investigation — even one episode, even if it cleared on its own, even without pain. The bleeding stopping is not the same as the cause being resolved.
- Painless hematuria in a man over 50 is bladder cancer until proven otherwise. This is the single highest-yield clinical pattern in urology and the one most often dismissed by patients and primary care.
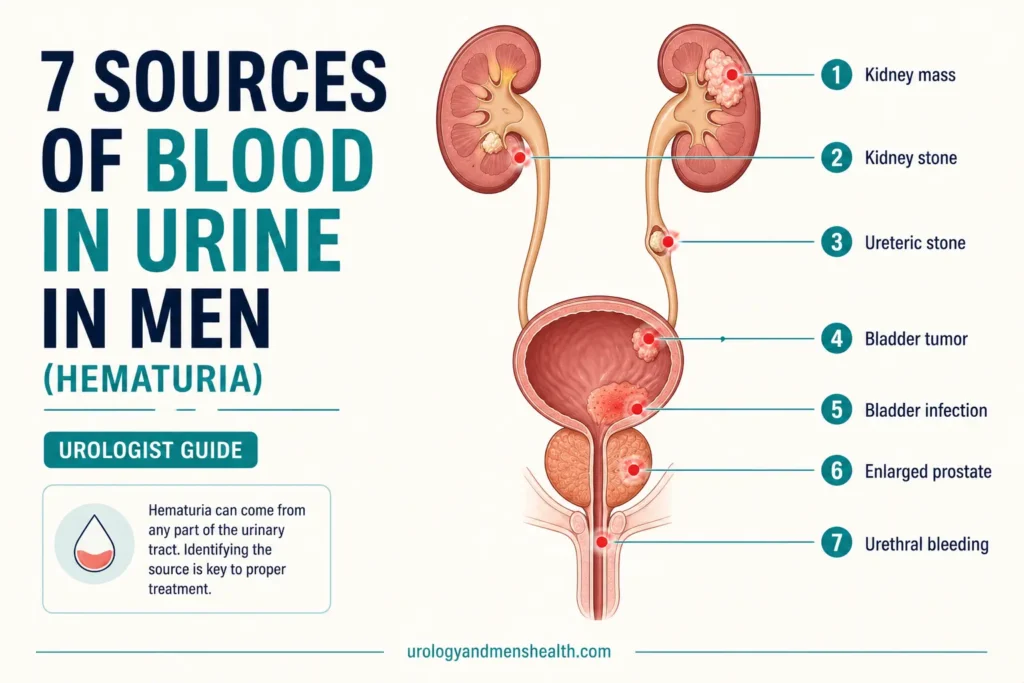
- The 7 causes covered here are: UTI, kidney stones, bladder cancer, BPH, kidney cancer, glomerulonephritis (kidney disease), and exercise-induced hematuria — in roughly that order of clinical likelihood for a man presenting with visible blood.
- The standard workup is three tests: urine analysis, CT urogram, and flexible cystoscopy. No single test covers the full urinary tract — all three are needed in most cases.
- Blood thinners do not cause hematuria — they unmask it. If you bleed into your urine on warfarin, aspirin, or apixaban, there is still an underlying source that needs identification. The investigation is identical.
- Microscopic hematuria (blood invisible to the naked eye, picked up only on a urine dipstick) also needs investigation in higher-risk men — those over 50, smokers, or with occupational chemical exposure.
In This Guide:
Gross vs. Microscopic Hematuria: What’s the Difference?
Gross (visible) hematuria means you can see the blood — your urine looks pink, red, brown, or tea-colored. Just 1 mL of blood in 1 liter of urine (about 1/4 teaspoon in 1 quart) is enough to produce visible discoloration. Even faintly pink urine should be taken seriously.
Microscopic hematuria means red blood cells are present in the urine but invisible to the naked eye — they are detected on a urine dipstick test or under a microscope during a routine check. The American Urological Association defines clinically significant microscopic hematuria as 3 or more red blood cells per high-power field on microscopy, and recommends investigation based on a single positive sample rather than the older “two of three samples” rule [1].
Both deserve investigation, but gross hematuria is treated as higher-risk because the probability of finding a serious underlying cause — particularly bladder or kidney cancer — is several times higher than with microscopic hematuria alone. If you cannot tell whether your urine color change is blood or something benign like beets, dehydration, or food coloring, the urine color decoder tool walks you through the differential.
In My Practice
The patients I worry about most are the ones who tell me, on the second or third visit, that they actually had blood in their urine “a while back” but did not mention it because it had stopped. By the time they bring it up, sometimes weeks or months have passed. With kidney stones or UTI, that delay is usually harmless. With bladder cancer, those weeks matter — every cystoscopy I do where the tumor has clearly grown since the patient first noticed blood is a missed window.
I have made it a rule in my own clinic: I ask every man over 45 about hematuria directly, even if it is not the reason he came in. Half the time the answer is no. The other half includes the cases that need urgent investigation.
The 7 Causes of Blood in Urine in Men
The seven most common causes I see in clinic, ranked roughly by frequency in adult men, are: urinary tract infection, kidney stones, bladder cancer, an enlarged prostate (BPH), kidney cancer, kidney disease (glomerulonephritis), and exercise-induced hematuria. Each has a different clinical fingerprint, and your job — and mine — is not to guess which one you have, but to make sure the investigation rules out the dangerous causes before settling on the benign explanation.
Cause 1: Urinary Tract Infection (UTI)
UTI is one of the most common causes of hematuria, particularly when it comes with burning on urination, frequency, urgency, and cloudy or foul-smelling urine. The infection inflames the bladder lining (cystitis), small surface vessels rupture, and blood appears in the urine.
Here is the clinical catch: in men, UTIs are uncommon enough that when one does occur, it often points to an underlying problem — incomplete bladder emptying from BPH, a kidney stone seeding bacteria, or a structural abnormality. A UTI in a man should not be treated with antibiotics and forgotten. A first UTI in a man over 50, or any recurrent UTI, warrants further workup [2]. You can estimate your personal UTI risk profile and what makes recurrence more likely with the UTI risk assessment for men.
Cause 2: Kidney Stones
Kidney stones are a common cause of both gross and microscopic hematuria. As a stone moves through the ureter — the narrow tube connecting kidney to bladder — it scrapes the lining and bleeds. The classic presentation is severe one-sided flank pain (renal colic) with blood in the urine. Some stones, however, sit silently in the kidney itself and produce painless hematuria; it is the moving stones that hurt.
If hematuria comes with colicky flank pain, nausea, and the inability to find a comfortable position, kidney stones are the most likely diagnosis. A non-contrast CT scan of the kidneys, ureters, and bladder (CT KUB) is the gold standard for confirming a stone — it identifies location, size, and density with around 97% sensitivity [3]. If a stone has been retrieved or partially passed, the kidney stone composition identifier helps work out which type of stone it is and what dietary changes to focus on.
➡ Related Read: Kidney Stones — Complete Guide from a UrologistCause 3: Bladder Cancer
This is the cause every urologist is trained to rule out first. Bladder cancer is the most common urinary tract malignancy presenting with hematuria, and its classic presentation is painless, intermittent, gross hematuria in a man over 50. The patient feels well, sees blood in the urine one day, it clears up on its own within a day or two, and he assumes the problem has gone. Weeks or months later, it recurs. The reason it bleeds intermittently is that the surface of a bladder tumor is fragile and bleeds when the bladder fills and stretches against it; once the bleed stops, the urine clears, but the tumor is still there.
The risk factors that meaningfully shift the probability of bladder cancer are: smoking (the single strongest risk factor — current and former smokers have around 3 times the risk of lifelong non-smokers), occupational exposure to aromatic amines (dye workers, painters, rubber and leather industry, hairdressers exposed to older permanent hair dyes), age over 50, and male sex (men are 3 to 4 times more likely than women to develop bladder cancer) [4].
The investigation for suspected bladder cancer is a flexible cystoscopy — a thin camera passed through the urethra into the bladder under local anesthetic gel, which lets the urologist look directly at the lining. If a tumor is seen, the next step is a TURBT (transurethral resection of bladder tumor) under anesthetic to remove it and biopsy the muscle to determine depth.
➡ Related Read: Bladder Cancer — Symptoms, Stages, and What Happens After DiagnosisCause 4: Benign Prostatic Hyperplasia (BPH)
An enlarged prostate can cause hematuria because the enlarged glandular tissue carries a dense network of blood vessels on its surface. These dilated vessels can bleed spontaneously or with straining, producing visible blood in the urine. BPH-related hematuria is usually accompanied by other lower urinary tract symptoms: weak stream, hesitancy, frequency, urgency, nighttime urination (nocturia), and a feeling of incomplete emptying.
Here is the clinical principle that matters most: you cannot assume hematuria is “just from the prostate” without completing the full investigation. Men with BPH can have bladder cancer at the same time — they are in the same age group, often the same risk profile (older male, smoker, prior occupational exposure). BPH should be a diagnosis of exclusion for hematuria, not a first assumption. I will accept BPH as the cause only after a normal CT urogram and a normal cystoscopy [5].
Cause 5: Kidney Cancer (Renal Cell Carcinoma)
Kidney cancer classically presents with the triad of hematuria, flank pain, and a palpable abdominal mass — but in modern practice, this complete triad is seen in fewer than 10% of cases. Most kidney cancers today are picked up incidentally on a CT or ultrasound scan ordered for some unrelated reason. When kidney cancer does cause visible blood, it tends to be intermittent and painless, much like bladder cancer.
Risk factors include smoking, obesity, uncontrolled hypertension, and a family history of kidney cancer. It is more common in men than women (around 2:1) and typically presents after age 50. CT urogram with intravenous contrast is the primary imaging test for both detection and staging [6].
➡ Related Read: Kidney Masses and Cysts — When to Worry About RCCCause 6: Kidney Disease (Glomerulonephritis)
When the kidneys’ glomeruli — the microscopic filtering units that separate blood from urine — become inflamed or damaged, red blood cells leak through the filter into the urine. This is called glomerulonephritis, and the most common cause worldwide is IgA nephropathy. Other causes include post-streptococcal glomerulonephritis (after a recent throat or skin infection), lupus nephritis, and other autoimmune conditions.
The distinguishing fingerprint of glomerular hematuria is that the urine looks brown or cola-colored rather than bright red, and the bleeding usually comes with protein in the urine (proteinuria), swelling around the eyes and ankles (edema), and high blood pressure. Under a microscope, the red blood cells look misshapen (dysmorphic) — they have been mechanically distorted by squeezing through the damaged glomerular filter, which is the urine microscopist’s clue that the bleeding source is in the kidney itself, not the bladder. These patients need referral to a nephrologist (kidney specialist) rather than a urologist [7]. Because the same patients often have undetected hypertension driving the kidney damage, this is also a moment to read about how high blood pressure silently damages the kidneys.
Cause 7: Exercise-Induced Hematuria
Hard exercise — particularly long-distance running — can cause transient hematuria. Two mechanisms drive it: repeated impact of the bladder wall against itself during running (sometimes called “runner’s bladder”) and a temporary drop in blood flow to the kidneys during sustained intense exertion. Dehydration concentrates the urine and makes any small amount of blood more visible.
Exercise-induced hematuria is a diagnosis of exclusion. It typically resolves within 48 to 72 hours of rest. If the blood persists past 72 hours, recurs, or appears at exercise intensities that previously did not provoke it, the full investigation is still needed. Never accept hematuria as exercise-related until the full urinary tract has been confirmed normal [8].
➡ Related Read: What Color Is Your Urine? A Urologist Decodes the SpectrumPainless Hematuria in Men Over 50: The Single Most Important Pattern
If you take one thing away from this article, take this: painless, intermittent, visible blood in the urine of a man over 50 is bladder cancer until proven otherwise. This is not a scare line. It is the single most reliable clinical pattern in urology, and it is the pattern that gets dismissed most often — by patients who feel well, by partners who hope it was nothing, and sometimes by clinicians who attribute the bleed to a presumed UTI without sending a culture or arranging imaging.
The reason painless hematuria is more concerning than painful hematuria is mechanical. A kidney stone hurts because it stretches the ureter as it moves. A UTI hurts because the inflamed bladder wall is firing pain signals every time it fills. A bladder tumor sitting on the dome of the bladder has no pain fibers in its surface — it can grow to several centimeters and bleed repeatedly without hurting at all. The absence of pain is not reassurance; it is information.
What you should actually do, as a man over 50 with even one episode of painless visible blood: contact your primary care doctor and specifically request a urology referral plus a CT urogram and flexible cystoscopy. In US practice, the AUA recommends evaluation within a defined timeframe; in UK and Irish practice, this is the urgent two-week-wait pathway. If you are told the blood is “probably just a UTI” without a urine culture, urine cytology, and a referral plan, ask the question directly: “If this is not a UTI, what is the next test you would arrange, and when?”
The Investigation: What Happens When You See a Urologist
When you present with hematuria, the investigation is designed to look at the entire urinary tract — kidneys, ureters, bladder, prostate, and urethra. No single test covers all of it, which is why the standard workup combines three.
Step 1: Urine Analysis
Urine dipstick confirms blood is actually present (not beet juice or food dye). Urine microscopy counts the red blood cells and looks at their shape — dysmorphic cells point toward a kidney (glomerular) source, normal cells point toward a lower tract (bladder, prostate, urethra) source. Urine culture rules out infection. Urine cytology looks for abnormal cells suggestive of bladder cancer; it is not as sensitive as cystoscopy but adds value when positive.
Step 2: Imaging — CT Urogram
A CT urogram is a CT scan done in two phases — first without contrast (to look for stones, which show up as bright white objects), then with intravenous contrast that flows through the kidneys and is excreted into the urinary tract (which lights up the kidneys, ureters, and bladder for cancer and structural assessment). It is the gold standard imaging test for hematuria [9]. In men with significant kidney function impairment, an MRI urogram is the alternative.
Step 3: Cystoscopy
Flexible cystoscopy is a camera examination of the bladder done in the outpatient clinic. A thin flexible scope is passed through the urethra under local anesthetic gel, and the urologist looks directly at the bladder lining on a monitor. This is the only reliable way to detect bladder cancer — imaging alone can miss flat (carcinoma in situ) lesions that lie in the surface of the bladder wall without forming a visible mass. The procedure takes 5 to 10 minutes. It is uncomfortable but tolerable, and modern flexible scopes are far less invasive than the older rigid ones.
“But I’m on Blood Thinners” — Why You Still Need Investigation
I hear this every week: “My doctor said the blood is probably from the warfarin/aspirin/apixaban.” This is a dangerous misconception, and it is one of the most common reasons hematuria investigation gets delayed. Anticoagulants (blood thinners) do not cause hematuria — they unmask it. A normal urinary tract does not bleed just because you are on a blood thinner. If blood is appearing in your urine on anticoagulants, there is an underlying source, and that source needs identification.
The published evidence is consistent: men on anticoagulants who present with hematuria have the same rate of significant urological findings, including cancer, as men not on anticoagulants [10]. The investigation should proceed in exactly the same way regardless of whether you are on warfarin, aspirin, clopidogrel, apixaban, rivaroxaban, or any other agent. If your primary care doctor tells you the blood is “from the warfarin,” ask directly: “Can you arrange a urology referral and a CT urogram so we can confirm there is no underlying cause?”
In My Practice
The most preventable cancer cases I see are men in their 60s and 70s who first noticed blood in their urine months earlier, were started on antibiotics for a presumed UTI, never had a urine culture sent, and never had imaging arranged. By the time they reach me, the bladder tumor is sometimes large enough that the standard TURBT alone is not curative and we need to discuss radical cystectomy. None of that is the patient’s fault. It happens because the system does not always treat a single episode of hematuria with the urgency it deserves.
If you are in the situation right now — you saw blood once, it stopped, you were told it was probably a UTI, and no further investigation has been arranged — please do not wait for the next episode. Phone your primary care office and ask for the referral specifically by name: urology, with a CT urogram and flexible cystoscopy.
Bringing your hematuria question to a doctor next week? Download the prep guide.
Enter your email below to receive Dr. Khalid’s complete 7-Day Kidney Stone Prevention Meal Plan as a free, printable PDF — it covers the kidney protection rules that prevent the most common benign cause of blood in urine in men.
When to See a Doctor — Urgently
- Any visible blood in urine — even once — needs urological investigation, including CT urogram and flexible cystoscopy. Do not wait for it to recur before acting.
- Painless hematuria in a man over 50 — highest probability of bladder cancer. Phone your primary care doctor the same day and ask for a urology referral.
- Blood in urine with clots — the bleeding volume is significant. Go to the emergency room if clots are passing or if you are passing large amounts of blood.
- Hematuria with inability to urinate (clot retention) — this is a urological emergency. Go to the ER. The bladder needs urgent catheterization and washout.
- Blood in urine with weight loss, persistent flank pain, or a palpable abdominal mass — concerning features for kidney or urothelial cancer. Request urgent imaging the same week, not “in a few weeks.”
Frequently Asked Questions
If the blood went away on its own, do I still need to be investigated?
Yes. The single most dangerous misunderstanding about blood in urine is that the bleeding stopping equals the cause being resolved. Bladder and kidney cancer typically cause intermittent hematuria — the tumor surface bleeds for a day or two, then a small clot covers the bleed, the urine clears, and the cancer continues to grow silently in the meantime. Every episode warrants the full workup: urine cytology, CT urogram, and cystoscopy. Read more about bladder cancer presentation patterns.
Is microscopic hematuria (blood only on dipstick) serious?
It can be. While microscopic hematuria carries a substantially lower cancer risk than gross hematuria, it still warrants investigation in higher-risk men — those over 50, current or former smokers, men with occupational chemical exposure, and men with any irritative urinary symptoms. The AUA’s 2020 guideline lowered the previous threshold and now recommends evaluation based on a single positive sample with risk-stratified imaging and cystoscopy [1]. Transient microscopic hematuria after exercise, intercourse, or minor trauma can usually be monitored with repeat testing in low-risk men. More on the men’s hematuria workup here.
Does blood in urine always mean cancer?
No. Cancer is found in approximately 15 to 20% of men investigated for visible hematuria, meaning the majority have benign causes — UTI, kidney stones, BPH, glomerular kidney disease, or exercise. The reason every episode is investigated is the consequences of missing the 15 to 20%. Think of the workup as a screening process: most men come back reassured, but the men whose cancer is caught at the first episode are the ones who get a curative TURBT instead of a radical cystectomy. More on the benign causes here.
Can my primary care doctor handle hematuria, or do I need a specialist?
Your primary care doctor can do the first round of tests — urine dipstick, urine culture, and basic blood work — and that is a valuable starting point. The complete hematuria in men workup, however, requires CT urogram imaging and flexible cystoscopy, both of which are specialist investigations arranged or performed by a urologist. Your primary care office should refer you promptly. In US practice, the AUA pathway defines the timeline. In UK and Irish practice, visible hematuria in men over 45 triggers a two-week-wait urgent referral. When to ask for a urologist directly.
My blood in urine came with severe pain — is that better or worse than painless blood?
Counterintuitively, painful hematuria is usually more reassuring than painless. Pain with blood typically means kidney stone or UTI — both treatable, both benign. Painless hematuria — particularly in a man over 50 — is the presentation that raises the highest suspicion for bladder or kidney cancer, because the surfaces of those tumors do not have pain fibers and can bleed repeatedly without hurting. The absence of pain should never be taken as reassurance. If you are over 50 and you saw blood once without pain, treat that single episode as the highest priority for investigation.
References
- Barocas DA, Boorjian SA, Alvarez RD, et al. Microhematuria: AUA/SUFU Guideline. J Urol. 2020;204(4):778-786. PubMed
- Schaeffer AJ, Nicolle LE. Urinary tract infections in older men. N Engl J Med. 2016;374(6):562-571. PubMed
- Smith-Bindman R, Aubin C, Bailitz J, et al. Ultrasonography versus computed tomography for suspected nephrolithiasis. N Engl J Med. 2014;371(12):1100-1110. PubMed
- Burger M, Catto JW, Dalbagni G, et al. Epidemiology and risk factors of urothelial bladder cancer. Eur Urol. 2013;63(2):234-241. PubMed
- Foster HE, Dahm P, Kohler TS, et al. Surgical management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA Guideline Amendment 2019. J Urol. 2019;202(3):592-598. PubMed
- Ljungberg B, Albiges L, Abu-Ghanem Y, et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update. Eur Urol. 2022;82(4):399-410. PubMed
- Vivante A, Afek A, Frenkel-Nir Y, et al. Persistent asymptomatic isolated microscopic hematuria in adolescents and young adults and risk for end-stage renal disease. JAMA. 2011;306(7):729-736. PubMed
- Jones GR, Newhouse I. Sport-related hematuria: a review. Clin J Sport Med. 1997;7(2):119-125. PubMed
- Silverman SG, Leyendecker JR, Amis ES Jr. What is the current role of CT urography and MR urography in the evaluation of the urinary tract? Radiology. 2009;250(2):309-323. PubMed
- Avidor Y, Nadu A, Matzkin H. Clinical significance of gross hematuria and its evaluation in patients receiving anticoagulant and antiplatelet therapy. Urology. 2000;55(1):22-24. PubMed
- Witjes JA, Bruins HM, Cathomas R, et al. European Association of Urology Guidelines on Muscle-Invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur Urol. 2021;79(1):82-104. PubMed

Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.