Viagra vs Cialis Comparison: Urologist’s Guide
When patients ask me whether Viagra or Cialis is better, they are usually focused on which one is more powerful. In my experience, that is the wrong question. The secret to these medications isn't strength; it's matching the drug's exact timeline and food rules to your actual life. This guide strips away the marketing to explain how these molecules really work, so you can finally ask your doctor for the right prescription.

Most viagra vs cialis comparison guides start with the wrong question. The real one is not “which pill is stronger?” but “which molecule fits the way you actually have sex?” In clinic I see the same scenario every week — a man tried sildenafil once after a heavy dinner, found it disappointing, and concluded the drugs do not work for him. The drugs almost certainly do work for him. He was using the wrong one for his life.
Let me start with the basic point that causes the most confusion. “Viagra” and “sildenafil” are not two different drugs. They are the same molecule — sildenafil is the generic name, Viagra is Pfizer’s brand name. Cialis is tadalafil. Levitra is vardenafil. Stendra is avanafil. Four molecules, one class of medication: the phosphodiesterase type 5 (PDE5) inhibitors. Everything else — the glossy advertising, the color-coded packaging, the price difference of 50 to 1 between brand and generic — is marketing.
That said, the four molecules are not interchangeable. They differ meaningfully in how quickly they work, how long they last, how food affects them, and which side effects they tend to cause. In over a decade of prescribing these medications, I have learned that the choice is almost always about matching the drug’s pharmacology to the patient’s sexual pattern. A spontaneous weekend with your wife is a completely different prescribing problem from planned intimacy every Friday night. This guide will walk you through every practical difference. By the end, you will be able to have a proper conversation with your doctor rather than simply accepting whatever was prescribed first.
Key Takeaways
- “The tablet did not work” is usually a usage problem, not a drug failure — fatty meals, wrong timing, or insufficient dose explain the majority of complaints I see in clinic
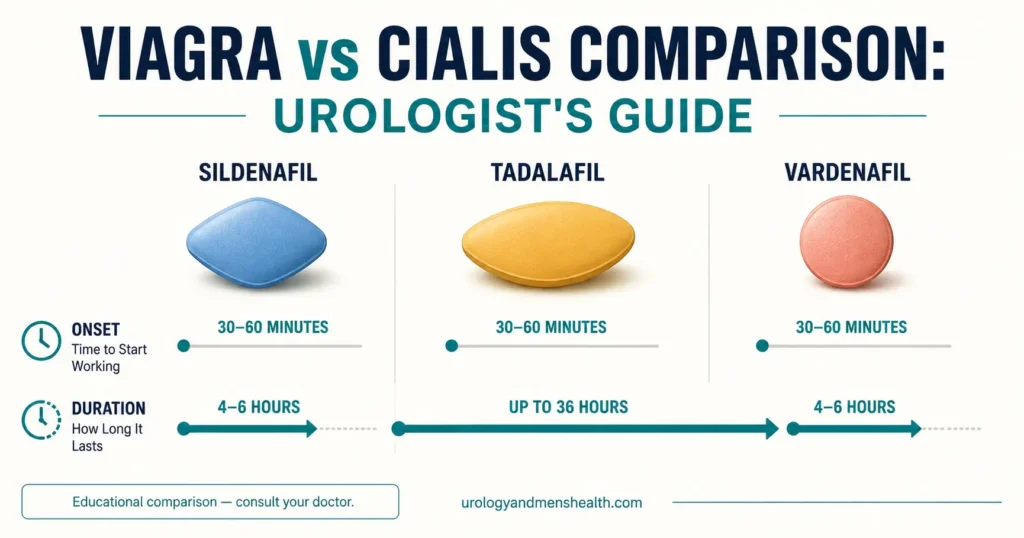
- Sildenafil (Viagra): onset 30-60 min, duration 4-6 hours, significantly impaired by fatty food
- Tadalafil (Cialis): onset 30-60 min, duration up to 36 hours, unaffected by food, and uniquely licensed for daily 2.5-5 mg dosing [1]
- Vardenafil (Levitra): similar to sildenafil but slightly faster onset and less food interaction
- Avanafil (Stendra): fastest onset at 15-30 minutes, cleanest side-effect profile, most recently licensed of the four (2012)
- PDE5 inhibitors are absolutely contraindicated with nitrates (including recreational “poppers”) — this combination can cause fatal hypotension [2]
- Daily low-dose tadalafil is the right starting choice for most men with ED and bothersome urinary symptoms from BPH
- Generic sildenafil costs roughly $1-2 per tablet in the US versus $70-90 for brand Viagra — identical active ingredient, identical FDA manufacturing standard
How PDE5 Inhibitors Actually Work (The Part Most Men Get Wrong)
This matters because it is the source of the single most common complaint I hear: “The tablet did not work.” More often than not, the tablet worked perfectly — the patient was using it wrong.
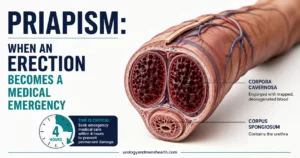
An erection is a vascular event. When you are sexually aroused, nerves in the penis release nitric oxide, which triggers smooth muscle relaxation in the corpora cavernosa (the spongy tissue of the penis). That relaxation lets blood flow in, the penis becomes engorged, and the veins get compressed against the tunica albuginea — trapping the blood and maintaining rigidity.
The molecule that ends this process is called cyclic GMP. An enzyme called phosphodiesterase type 5 (PDE5) breaks down cyclic GMP, the erection subsides, and blood drains out. This is normal and necessary physiology.
PDE5 inhibitors do exactly what the name says: they inhibit the enzyme that breaks down cyclic GMP. More cyclic GMP sticks around, smooth muscle stays relaxed for longer, the penis stays engorged for longer. But there must be arousal first. The drug does not create an erection — it protects the erection that your own nervous system starts. Take a tablet, sit on the sofa, watch the news, and nothing will happen. That is not drug failure. That is pharmacology working correctly [3].
What This Means Practically
- You need sexual stimulation for these drugs to work
- If you are nervous, over-focused on performance, or angry with your partner, the drug may not overcome the psychological block
- If there is no nitric oxide release — which happens in severe diabetes, pelvic nerve injury after prostate surgery, or advanced vascular disease — there may not be enough cyclic GMP produced in the first place, and the drug will seem ineffective
Getting this concept right explains around 30% of the “drug did not work” complaints I see. The other 70% involve incorrect timing, fatty meals, or wrong dose — which I will come to in a moment.
The Four Molecules — Detailed Comparison
Let me go through each drug systematically. I will give you the pharmacology plus what actually matters in practice.
Sildenafil (Viagra) — The Original
Licensed in 1998. The first of its class, and still the most commonly prescribed. Doses: 25, 50, 100 mg. Most men start at 50 mg; 100 mg is the maximum licensed dose [4].
- Onset: 30-60 minutes
- Peak effect: 60-120 minutes
- Duration: 4-6 hours
- Food effect: Significant. A fatty meal can delay absorption by up to an hour and reduce peak blood levels by around 30%. Take on an empty stomach or after a light meal for best effect
- Best for: Planned intercourse when you can predict timing; men who prefer a shorter-acting drug
Sildenafil is a proven, reliable molecule with 25+ years of real-world use. The food interaction is the single most common reason it “fails” — men take it after a heavy dinner and wonder why it did not kick in.
Tadalafil (Cialis) — The “Weekend Pill”
Licensed in 2003. Doses: 2.5, 5, 10, 20 mg. Tadalafil is pharmacologically unique because of its extraordinarily long half-life.
- Onset: 30-60 minutes
- Peak effect: 2 hours
- Duration: Up to 36 hours
- Food effect: None — eat whatever you want
- Best for: Men who value spontaneity; men with concurrent BPH/LUTS; men who prefer daily dosing
The 36-hour duration is the defining feature. Take one tablet on Friday evening, and it is still pharmacologically active on Sunday morning. This is why Cialis earned the nickname “the weekend pill” — it eliminates the 30-minute timing window pressure that some men find destroys intimacy.
Tadalafil is also available as a daily 2.5 or 5 mg tablet. This is a different prescribing proposition: instead of taking a larger dose before sex, you take a small dose every day, and the drug sits at a steady low level in your bloodstream. Within 5 days you have “background” readiness at all times. Many couples find this dramatically improves the quality of their sex life because it removes planning and performance anxiety entirely. It is also uniquely licensed for BPH symptoms — which is why daily tadalafil is often my first choice in men over 55 with both ED and bothersome urinary frequency or nocturia [1].
Vardenafil (Levitra) — The Understudy
Licensed in 2003 (same year as tadalafil). Doses: 5, 10, 20 mg.
- Onset: 25-60 minutes
- Peak effect: 45 minutes
- Duration: 4-8 hours
- Food effect: Mild — less affected by food than sildenafil but more than tadalafil
- Best for: Men who want something similar to sildenafil but with less food interaction; men with diabetes-related ED (where some evidence suggests slightly better efficacy)
Vardenafil is a good molecule that has never quite captured market share, largely because Cialis launched the same year with a much longer duration. It is a reasonable choice, particularly in orodispersible (dissolves on the tongue) formulations for men who struggle to swallow tablets.
Avanafil (Stendra) — The Fastest Option
Licensed in 2012, the most recently licensed of the four. Doses: 50, 100, 200 mg.
- Onset: 15-30 minutes (the fastest)
- Duration: 6 hours
- Food effect: Minimal
- Best for: Men who want the quickest onset; men who get bothersome facial flushing, headache, or nasal congestion on the older drugs (avanafil is more selective and has a cleaner side-effect profile)
Avanafil’s selling point is speed and tolerability. It binds more selectively to PDE5 and less to other PDE enzymes in the body, which translates to fewer “off-target” side effects like headache and visual disturbance. The downside is cost and availability — it is not yet widely stocked on generic prescription in many regions, and US insurance coverage is inconsistent.
Side Effects — What to Actually Expect
The clinical pattern I see is reassuringly consistent: most men get one or two minor symptoms, almost always tolerable, almost always settling within an hour or two. The headache that comes 20 minutes after the first tablet often does not happen on the second tablet. The top five side effects, in order of frequency, are [3,5]:
- Headache (10-15% of users) — caused by vasodilation of intracranial blood vessels. Usually responds to acetaminophen (paracetamol)
- Facial flushing (10%) — a warm, blushing sensation in the cheeks and neck. Harmless and self-limiting
- Nasal congestion (4-8%) — blocked or runny nose
- Dyspepsia / heartburn (4-7%) — most common with tadalafil due to its long half-life
- Muscle aches and back pain (3-5%) — almost unique to tadalafil, typically 12-24 hours after dosing
Rare but Important
- Visual disturbance — temporary blue-tinged vision (especially with higher-dose sildenafil) due to weak cross-inhibition of PDE6 in the retina. Harmless and reversible
- Priapism — painful erection lasting more than 4 hours. Very rare (under 0.1%) but a medical emergency. Men with sickle cell disease, leukemia, or on other medications that affect priapism risk need particular care
- Non-arteritic anterior ischemic optic neuropathy (NAION) — sudden painless loss of vision in one eye. Extremely rare but reported. Stop the drug and seek ophthalmological review immediately if this occurs
- Hearing changes — tinnitus or sudden hearing loss has been reported rarely
The Absolute Contraindication — Nitrates
Life-Threatening Interaction — Nitrates
Never combine a PDE5 inhibitor with nitrate medication. The combination can cause catastrophic, fatal hypotension [2]. This includes:
- Nitroglycerin (GTN) spray or tablets prescribed for angina
- Isosorbide mononitrate or isosorbide dinitrate
- Nicorandil
- Amyl nitrite or “poppers” — recreationally inhaled
If you take any of these medications, you cannot take a PDE5 inhibitor. If you have had a recent heart attack, unstable angina, or uncontrolled heart failure, you need cardiology clearance before starting an ED medication at all — request a stress test or ETT result review at your next cardiology appointment.
If you are on an alpha-blocker for prostate symptoms (tamsulosin, alfuzosin, doxazosin), the combination is not dangerous but can cause dizziness from additive blood pressure effects. The safe approach is to start at a low PDE5 inhibitor dose and take the two medications at least 4 hours apart.
How a Viagra vs Cialis Comparison Plays Out in Clinic
Here is how I genuinely decide in clinic. Every patient gets a 5-minute conversation about the differences before any prescription gets written.
➡️ Related Read: Erectile Dysfunction Treatment — A Urologist’s Step-by-Step ProtocolMy Default Starting Point — Tadalafil 5 mg Daily
For most men over 50 with ED, I favor daily tadalafil 5 mg. Here is why:
- Removes the timing window — sex is spontaneous, not scheduled
- Treats concurrent BPH / LUTS (a large proportion of my patients have both)
- Often has a beneficial effect on early-morning erections and overall erectile quality
- Avoids the “took the tablet too early or too late or after a big meal” problem that wrecks so many first prescriptions
When I Choose Sildenafil
- Younger men with infrequent sex who do not want daily medication
- Cost-conscious patients — generic sildenafil is the cheapest option in the US, often under $2 per tablet with a discount card
- Men for whom on-demand dosing simply fits their lifestyle better
When I Choose Avanafil
- Men who had bad headaches or flushing on sildenafil or tadalafil
- Men who need faster onset (under 30 minutes reliably)
When I Switch Drugs
If a man has genuinely failed a maximum-dose PDE5 inhibitor taken correctly (empty stomach, adequate sexual stimulation, 30-60 minutes before intercourse, on at least four separate occasions before labeling it a failure), I switch molecules. A clear meaningful proportion of men who do not respond to sildenafil respond to tadalafil, and vice versa. Before abandoning the class entirely, always try at least two different PDE5 inhibitors at maximum dose [3].
In My Practice
The single most common “failed PDE5 inhibitor” scenario I see in clinic is a man who was prescribed sildenafil 50 mg, took it once after a heavy dinner with two glasses of wine, found it disappointing, and never tried again. I always ask four specific questions before accepting that a medication has failed: (1) Was it taken on an empty stomach or at least 2 hours after a light meal? (2) Was it taken 45-60 minutes before intended intercourse? (3) Was there adequate foreplay and arousal? (4) Was it tried at the maximum dose on at least four separate occasions?
If the answer to any of these is “no,” the medication has not actually failed. It has not yet been properly tested.
Choosing the Right ED Medication Starts With Knowing Your Pattern
Enter your email below to receive Dr. Khalid’s complete Evidence-Based ED Action Plan as a free, printable PDF — including the 4-question medication failure test and what to bring to your next appointment.
Generic vs Brand — A Practical Note on Cost
Sildenafil came off patent in 2013 and tadalafil in 2017. The generic formulations contain identical active ingredient to the brand, manufactured to the same FDA pharmaceutical quality standards in regulated markets. Generic sildenafil can cost as little as $1-2 per tablet at major US pharmacies with a discount card (GoodRx, Costco); brand Viagra retails at $70-90 per tablet without insurance [4]. The difference buys you a blue diamond-shaped tablet and a box. That is all.
A word of caution: do not buy PDE5 inhibitors from unregulated online sources. Counterfeit medications are extraordinarily common in this drug class — some contain no active ingredient, some contain the wrong dose, and the most dangerous contain contaminants or undeclared drugs. Always buy from a regulated pharmacy or via a prescription from a registered clinician.
Drug Interactions You Should Know
Beyond the absolute nitrate contraindication, there are several interactions worth understanding. The interaction with blood pressure medications in particular is a frequent source of side effects, and is covered in more detail in our companion article on blood pressure medication and erectile dysfunction.
- Alpha-blockers (tamsulosin, alfuzosin, doxazosin) — additive blood pressure drop; separate doses by 4 hours, start at the lowest PDE5i dose
- Ritonavir, ketoconazole, itraconazole, clarithromycin — strong CYP3A4 inhibitors that dramatically raise PDE5i blood levels; reduce doses significantly
- Grapefruit juice — mild CYP3A4 inhibitor; best avoided within 24 hours of dosing
- Alcohol — not dangerous in moderate amounts, but heavy alcohol is itself a major cause of erectile failure, and its effect is independent of the drug
- Recreational drugs — stimulants (cocaine, methamphetamine) combined with PDE5i dramatically raise cardiovascular risk
Will These Drugs Work for Everyone?
Overall response rates for PDE5 inhibitors in general ED populations sit around 70-80% [3]. But that headline number hides important variation by underlying cause — and the underlying cause is what determines whether a tablet alone will be enough or whether you need a fuller workup. If you are unsure where you sit on the severity spectrum, our IIEF-5 Erectile Function Self-Assessment takes 90 seconds and gives a validated severity score.
- Psychogenic ED — very high response rates (over 85%). The drug acts as a confidence reset more than anything else
- Mild-to-moderate vascular ED — good response (70-80%). The largest category in my clinic
- Diabetic ED — moderate response (50-60%), but response improves substantially if blood sugar is brought under control. Request an HbA1c at your next visit if not done in the past 6 months
- Post-radical prostatectomy ED — significantly poorer response, particularly if nerve-sparing surgery was not possible. Often requires combination therapy or moving up the treatment ladder
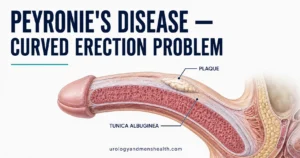
- Severe Peyronie’s disease, severe venous leak, advanced diabetes — poor response, other options (injections, vacuum devices, implants) may be needed sooner
Men with a clearly vascular problem should also be thinking beyond the tablet. ED is a vascular disease marker — if your penis cannot manage its blood flow, your heart may be next in line. A proper ED consultation should include a fasting lipid panel, HbA1c, and a blood pressure review, ideally within 6 weeks of starting ED treatment. The tablet is the easy part; the body-wide review is often what actually changes a man’s future. Read more on this in our piece on why morning wood is a check engine light for cardiovascular disease.
If your symptoms have a strong fatigue, low libido, or “feeling old before my time” component alongside the erectile difficulty, that pattern often points to coexisting low testosterone — see our guide on low testosterone in men over 40 for the symptom picture and what testing to request.
Frequently Asked Questions
Can I take two different PDE5 inhibitors on the same day?
No. Combining sildenafil and tadalafil (or any two PDE5 inhibitors) does not produce a bigger effect — it produces bigger side effects, particularly a greater drop in blood pressure. If one is not working, stop and try a different molecule on a separate day, after the first has cleared (24 hours for sildenafil, 36 hours for tadalafil). Read the full step-up treatment protocol here.
Why does my partner notice the tablet works differently on different nights?
This is one of the most common observations I hear in clinic, and it almost always traces back to four variables: meal content (fatty meals delay sildenafil absorption by up to an hour), timing (45-60 minutes before sex is the sweet spot for sildenafil and vardenafil), arousal level (the drug protects an erection your body initiates — without arousal, nothing happens), and dose (50 mg sildenafil works for many men, but 100 mg works for more). If your evenings are inconsistent, switching to daily tadalafil eliminates almost all of these variables.
Will daily tadalafil improve my erections even when the drug eventually leaves my system?
Daily tadalafil over 3-6 months of use appears to have a modest “rehabilitative” effect on the erectile tissue in some men, particularly after pelvic surgery or in mild vascular ED. The improvement is real but usually modest. On-demand dosing (sildenafil, vardenafil, avanafil, or on-demand tadalafil) does not produce long-term change in underlying erectile function — once the drug is out of your system, your baseline erection returns. If you are looking for a “rehabilitative” approach, daily tadalafil is the only PDE5 inhibitor with reasonable evidence for this.
How long before sex should I take it?
Sildenafil and vardenafil: 45-60 minutes on an empty stomach. Tadalafil: 30-60 minutes, with or without food. Avanafil: 15-30 minutes. Daily tadalafil: no specific timing — the full effect is reached by day 5 of continuous use, after which you have background readiness around the clock.
Are PDE5 inhibitors safe after a heart attack?
In most cases, yes — but only after cardiology clearance and only if you are not on nitrate therapy. Sexual activity itself is about as cardiovascularly taxing as climbing two flights of stairs. Men who can manage that level of exertion without chest pain can usually manage sex safely. The real danger is the combination of PDE5 inhibitors and nitrates, which is why a structured cardiology review matters. Request a copy of your most recent ETT or stress test result before your urology appointment.
Is generic sildenafil really as effective as brand Viagra?
Yes. Generic sildenafil contains the identical active ingredient to brand Viagra, manufactured to the same FDA regulatory standard. The pharmacology is identical. The price difference — roughly $1-2 versus $70-90 per tablet in the US — pays for packaging, advertising, and brand. Not for any clinical effect. The same applies to generic tadalafil versus brand Cialis.
References
References
- Salonia A, Bettocchi C, Carvalho J, et al. EAU Guidelines on Sexual and Reproductive Health. European Association of Urology. 2024. EAU
- Kloner RA. Cardiovascular effects of the 3 phosphodiesterase-5 inhibitors approved for the treatment of erectile dysfunction. Circulation. 2004;110(19):3149-3155. PubMed
- Burnett AL, Nehra A, Breau RH, et al. Erectile Dysfunction: AUA Guideline. American Urological Association. 2018 (amended 2022). AUA
- National Institute for Health and Care Excellence (NICE). Erectile dysfunction — Clinical Knowledge Summary. NICE. 2024. NICE
- Yuan J, Zhang R, Yang Z, et al. Comparative effectiveness and safety of oral phosphodiesterase type 5 inhibitors for erectile dysfunction: a systematic review and network meta-analysis. European Urology. 2013;63(5):902-912. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.