Aquablation Therapy for BPH vs TURP & HoLEP
When facing prostate surgery, the biggest hesitation usually isn't the operation itself, but the almost guaranteed loss of normal ejaculation. While older techniques are highly effective, Aquablation uses a robotic, heat-free waterjet to deliver maximum symptom relief while drastically lowering the risk of a dry orgasm. However, it is not the perfect choice for every prostate. This guide directly compares this new technology against TURP and HoLEP so you can see which procedure actually fits your anatomy.

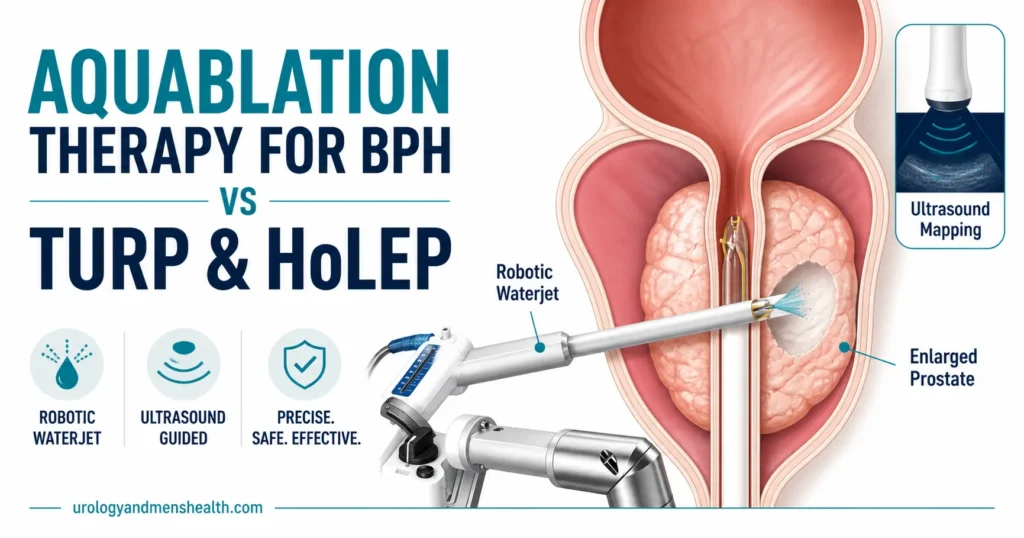
Aquablation therapy is the newest robotic option for an enlarged prostate, and it is genuinely different from anything we had before. It uses a high-pressure, heat-free waterjet — guided by ultrasound and steered by a robotic arm — to remove the obstructing prostate tissue. Patients keep asking me whether it is better than TURP or HoLEP. The honest answer is more interesting than a yes or no.
For the right man, aquablation can deliver TURP-level symptom relief with a dramatically lower risk of dry orgasm, almost regardless of how large the prostate is. For other men, the older techniques remain the smarter choice. This guide walks you through how aquablation actually works, how it stacks up against TURP and HoLEP on the metrics you care about, who is a good candidate, and what recovery looks like — written by a urologist who performs BPH surgery.
Key Takeaways
- Aquablation uses a heat-free, ultrasound-mapped robotic waterjet to remove BPH tissue — no electricity, no laser energy on the gland.
- Symptom relief at 1 year is comparable to TURP, but with a substantially lower rate of retrograde (dry) ejaculation: about 10% vs. 65–75%.
- It works for prostates 30–150 grams, with the strongest evidence in 30–80 g glands — covering the majority of BPH surgical candidates.
- Best for men who want to preserve ejaculatory function and are willing to undergo a short general anesthetic with a 1-night hospital stay.
- HoLEP remains the benchmark for very large prostates (>100 g) at experienced centers; aquablation is closing that gap but is newer.
What Is Aquablation Therapy? A Plain-English Explanation
Aquablation therapy — branded clinically as the AquaBeam Robotic System — is a treatment for benign prostatic hyperplasia (BPH) that uses a robotic, heat-free, high-velocity saline waterjet to remove the obstructing inner zone of the prostate gland. It received FDA clearance in the United States in 2017 and was approved by NICE in the United Kingdom in 2023 [1].
Here is what makes it different from every other BPH operation we have done for the last 80 years: no heat touches the prostate during the resection step. TURP burns away tissue with electrical current. HoLEP and GreenLight peel or vaporise tissue with laser energy. Aquablation simply uses water — pressurised to about 8,000 psi (similar to industrial waterjet cutting) but tuned so it shears soft adenomatous tissue while leaving blood vessels, nerves, and the prostate capsule intact [2].
The other unusual feature is the planning step. Before the waterjet fires, the surgeon uses a transrectal ultrasound (TRUS) probe to image the prostate live, then literally draws on a screen the exact zone of tissue to be removed — sparing the bladder neck, the verumontanum, and (crucially) the ejaculatory ducts. The robot then executes that plan with sub-millimetre precision. This is why aquablation preserves antegrade ejaculation in roughly 90% of men, while TURP destroys it in 65–75% [3].
💡 In My Practice
The first time I saw an aquablation case live, the part that surprised me was not the waterjet — it was the planning screen. The surgeon drew a treatment polygon on the ultrasound image, deliberately avoiding the area around the verumontanum. That single decision is what separates a “wet” surgery from a “dry” one for the patient.
For men who care about ejaculation — and most men under 65 do, even if they don’t say so on the first visit — that planning step is the entire reason aquablation is worth discussing. We could not draw a no-go zone with TURP if we wanted to.
How Aquablation Works: The Robotic Waterjet, Step by Step
The procedure takes about 30 to 60 minutes total, with the actual tissue resection lasting roughly 5 to 10 minutes [2]. Here is what happens, in order, on the day of surgery.
Step 1 — Anesthesia and Positioning
You are placed under general anesthesia (occasionally spinal). You lie on your back with your legs elevated in lithotomy position — the same posture used for cystoscopy or TURP. A urinary catheter and the rectal ultrasound probe are placed.
Step 2 — Imaging and Treatment Planning
The surgeon inserts a cystoscope to inspect the prostate visually, then uses live transrectal ultrasound to map the gland in three dimensions. Using a touchscreen interface, the surgeon outlines exactly which tissue to remove — including a deliberate exclusion zone around the verumontanum (the landmark that protects the ejaculatory ducts). This planning step is the part that most surgeons describe as “where the art is.”
Step 3 — Robotic Waterjet Resection
The robotic handpiece is locked into position. The surgeon presses a foot pedal, and the system fires a precisely controlled saline waterjet at high velocity, sweeping through the planned zone. The robot moves the jet automatically — the surgeon watches and can pause or adjust at any moment. Tissue is sheared away and washed out through the resectoscope. This step typically lasts 5 to 10 minutes regardless of prostate size, which is why aquablation has near-flat operative time even for very large glands.
Step 4 — Haemostasis (Stopping the Bleeding)
This is the one weakness of a heat-free technique: the waterjet does not seal blood vessels the way TURP electrical current or HoLEP laser energy does. So after the resection, the surgeon either uses brief, focal electrocautery to seal bleeding points, or relies on tamponade from a catheter balloon and continuous bladder irrigation. Newer protocols use minimal cautery and report shorter catheter times.
Step 5 — Catheter and Recovery
A urinary catheter is placed for 1 to 3 days. Most patients stay in hospital for 1 night. The catheter comes out once the urine runs clear of blood, and the great majority of men go home and urinate normally within 48 to 72 hours. Tissue removed during the procedure is sent to pathology — the same as with TURP and HoLEP — to rule out incidental prostate cancer.
→ Related Read: TURP Recovery Timeline — Week by WeekAquablation vs. TURP: The Old Standard Meets the Robot
TURP — transurethral resection of the prostate — has been the benchmark BPH surgery for over 50 years. It works. It has decades of follow-up. It is available in every hospital that has a urologist. So why even consider aquablation?
The answer comes from the WATER trial, a randomized controlled trial that pitted aquablation directly against TURP in 181 men with prostates 30–80 g. At 5 years of follow-up, the symptom score (IPSS) improvement was statistically equivalent between the two groups. But the difference in side-effects was striking [3][4].
Where Aquablation Wins
- Retrograde ejaculation: roughly 10% with aquablation vs. 65–75% with TURP. This is the single biggest reason men under 65 choose aquablation.
- Sexual function preservation: overall sexual satisfaction scores at 1 year are higher in the aquablation group [3].
- Operative time independent of prostate size: a 90 g gland takes roughly the same waterjet time as a 50 g gland — TURP scales linearly with size.
- Lower surgeon learning curve: the robot does the cutting; the surgeon does the planning. Outcomes appear consistent across centers earlier in the experience curve.
Where TURP Still Wins (Or Ties)
- Availability: every urologist trained anywhere in the world can do TURP. Aquablation requires a specific robotic platform and a trained team.
- Cost: TURP uses a single-use loop electrode that costs a few dollars. Aquablation uses a single-use disposable handpiece that costs in the thousands. We will discuss who pays for this further down.
- Bleeding control: TURP cauterises as it cuts. Aquablation needs a separate haemostasis step, and bleeding is the most common reason for re-intervention in the early postoperative period [5].
- Long-term track record: we have 50+ years of data on TURP. Aquablation has high-quality 5-year data and growing — but it is not 50 years.
So if your priorities are cost, immediate availability, and a procedure with the longest possible follow-up, TURP remains a perfectly reasonable choice. If your priority is preserving ejaculation while still getting TURP-level symptom relief, aquablation has the better data.
→ Related Read: HoLEP vs. TURP — Which Prostate Surgery Is Better?Aquablation vs. HoLEP: Two Powerful Tools, Different Trade-Offs
HoLEP — holmium laser enucleation of the prostate — is the closest direct rival to aquablation. Both are size-independent. Both deliver excellent symptom relief. Both send tissue to pathology. So the comparison gets interesting fast.
HoLEP is widely considered the gold standard for very large prostates (greater than 100 g) at experienced centers. It physically peels the obstructing inner gland away from the surgical capsule, then morcellates and removes it. The symptom score improvements at 5 and even 10 years are excellent, and re-treatment rates are among the lowest of any BPH surgery [6].
Where Aquablation Has the Edge
- Ejaculatory function: aquablation preserves antegrade ejaculation in roughly 90% of men. Standard HoLEP causes retrograde ejaculation in 70–80% — although newer “ejaculation-sparing HoLEP” techniques are improving these numbers.
- Surgeon learning curve: HoLEP has a notoriously long learning curve — surgeons typically need 30–50 supervised cases before outcomes plateau. Aquablation outcomes appear consistent across centers much earlier [7].
- Operative time predictability: aquablation resection time is largely independent of prostate size and surgeon. HoLEP times vary widely with both.
Where HoLEP Has the Edge
- Very large prostates (>100–150 g): HoLEP has by far the longest track record at this size. Aquablation data above 150 g is still limited.
- Long-term durability: HoLEP 10-year retreatment rates are exceptionally low. Aquablation 5-year data is excellent, but 10-year data is still being collected.
- No size limit and no robotic platform required: any hospital with a holmium laser and a trained surgeon can offer it.
- Day-case potential: at high-volume HoLEP centers, same-day discharge is increasingly common; aquablation typically requires a 1-night stay.
The honest summary: if you want the best chance of preserving ejaculation, aquablation is the stronger choice for prostates 30–150 g. If your prostate is over 150 g, or you live near a high-volume HoLEP center and ejaculation is not your top priority, HoLEP remains the durable workhorse. Both substantially outperform TURP for very large glands.
💡 In My Practice
I sat with a 58-year-old patient last month who had failed two years of combination tamsulosin and dutasteride. His prostate was 95 g. He was sexually active, in a stable relationship, and the moment we mentioned that TURP would almost certainly cause dry orgasm, he visibly tensed.
We discussed all three options — TURP, HoLEP, aquablation — with the actual percentage risk of retrograde ejaculation for each. He chose aquablation. Six months later his IPSS score had dropped from 22 to 6, his flow rate had doubled, and his ejaculation was unchanged. That outcome is no longer rare. It is increasingly the expectation for the right candidate.
Weak stream and night-time trips wearing you down? Download Dr. Khalid’s BPH & Enlarged Prostate Guide.
Enter your email below to receive Dr. Khalid’s complete BPH & Enlarged Prostate Guide as a free, printable PDF.
Who Is a Good Candidate for Aquablation?
Aquablation is not for every man with BPH. The procedure has clear best-fit criteria, and being honest about them at the consultation stage prevents disappointment later.
You Are Likely a Good Candidate If:
- Your International Prostate Symptom Score (IPSS) is moderate to severe — typically 8 or higher, with bothersome symptoms despite medication.
- Your prostate volume is between 30 and 150 grams on ultrasound or MRI. The strongest evidence base sits in the 30–80 g range, but data is steadily accumulating up to 150 g.
- You have tried medication (alpha-blockers like tamsulosin, or 5-alpha reductase inhibitors like finasteride) and either it has not worked, or the side effects have been intolerable.
- You specifically want to preserve ejaculatory function — this is the headline reason most patients choose aquablation over TURP or standard HoLEP.
- You can tolerate a brief general anesthetic and are fit for a 1-night hospital stay.
- You have access to a center that offers it — see the cost and availability section below.
Aquablation Is Probably Not the Right Choice If:
- Your prostate is over 150 grams — HoLEP at an experienced center has more long-term data here.
- You have known prostate cancer requiring radical treatment — aquablation is for BPH only.
- You have a severely contracted bladder neck or urethral stricture that needs to be addressed first.
- You are on uninterruptible blood-thinning medication — bleeding is the main early postoperative risk, and not being able to pause anticoagulation is a problem with any BPH surgery, but particularly heat-free ones. Discuss this directly with your surgeon and cardiologist.
- You are looking for a clinic-based, no-anesthetic procedure — for that, look at UroLift or Rezum, which trade some symptom-relief power for almost no recovery.
If you want a quick first-pass assessment of how severe your symptoms are before sitting down with a urologist, the BPH Symptom Score (IPSS) Calculator uses the same questionnaire your surgeon will run through at the first appointment.
Recovery, Risks, and What to Expect Afterward
Recovery from aquablation is generally faster than from TURP and comparable to HoLEP at experienced centers. Here is the realistic timeline based on the published data and what I tell my own patients.
Day 0 — Day of Surgery
You go home with a urinary catheter or stay one night in hospital — the latter is more common. Your urine will look pink to red the first day. This is normal. Continuous bladder irrigation is sometimes used overnight to keep the catheter clear of clots.
Day 1 to Day 3 — Catheter Out
Once the urine clears (usually within 24–72 hours), the catheter is removed. The first few times you urinate may sting, and the stream may not yet feel powerfully better — this is because the prostate is swollen from the surgery itself. Most men go home the day after the catheter is removed.
Week 1 to Week 2 — Back to Normal Activity
Most men with desk jobs return to work within 5 to 7 days. Avoid heavy lifting (anything over 10 lb / 4.5 kg), strenuous exercise, and cycling for 2 to 4 weeks. Light walking is encouraged from day one. You may notice intermittent blood in your urine for up to 2 weeks — this is expected as the surgical bed heals. Drink plenty of water; aim for around 2 to 2.5 litres a day (roughly 70–85 fl oz, or 8–10 cups).
Week 4 to Week 6 — Sexual Activity
Most surgeons clear patients to resume sexual activity at the 4 to 6 week mark, depending on healing. Erections typically return without delay (the nerves involved in erection sit outside the prostate, so any BPH surgery should not affect them). The big question for most patients — whether ejaculation is preserved — is usually clear from the first sexual encounter after surgery.
Month 3 and Beyond — Full Symptom Relief
Symptom scores continue to improve for up to 3 months as the prostate fully heals. By 6 months, most men have a stable, durable result that closely matches the figures published in the WATER trials. PSA levels typically settle at a new lower baseline — your urologist will use this as the starting point for future cancer surveillance.
Risks You Should Know About
- Bleeding requiring transfusion or clot evacuation: roughly 1–4% of cases, slightly higher than modern TURP and HoLEP [5].
- Urinary tract infection: 5–10%, similar to other BPH surgeries.
- Temporary urinary incontinence: short-term leakage in roughly 1–3% of men, almost always resolved within weeks.
- Urethral stricture or bladder neck contracture: 1–2%, similar to TURP.
- Retrograde ejaculation: approximately 10%, compared to 65–75% with TURP.
- Need for re-treatment within 5 years: roughly 5–7% in the WATER trial cohort — comparable to TURP and HoLEP at the same time point [4].
⚠️ When to Call Your Surgeon — Urgently
After any BPH surgery, including aquablation, get medical attention without delay if you experience:
- Heavy bright-red bleeding or blood clots blocking your urine flow
- Inability to urinate at all once the catheter has been removed
- Fever above 38.5°C (101.3°F), shivering, or feeling systemically unwell — this can indicate urosepsis
- Severe pain in the lower abdomen or pelvic area not controlled by your prescribed pain relief
- A swollen, painful, hot scrotum or testicle (possible epididymitis)
Cost, Availability, and How to Ask for It
Aquablation is now widely available in the United States, growing in the United Kingdom, and gradually rolling out across Europe, Asia, and Australasia. Cost and access vary substantially by country and insurance status.
United States
Aquablation has been covered by Medicare since 2023 for eligible men with moderate-to-severe BPH symptoms. Most major commercial insurers (including Aetna, Cigna, and many Blue Cross Blue Shield plans) now cover it as well. Out-of-pocket costs for an uninsured patient typically run between roughly $9,000 and $20,000 USD depending on the hospital and region. Aquablation is offered at most academic urology centers and a growing list of community hospitals. The American Urological Association recognizes aquablation as a guideline-supported treatment option for BPH [8].
United Kingdom and Ireland
NICE issued positive guidance on aquablation in 2023, and it is being commissioned at selected NHS centers. Availability is currently uneven — some trusts offer it routinely, others do not yet have the platform. Private aquablation in the UK typically costs £8,000 to £15,000. In Ireland, availability is more limited and largely confined to private hospitals.
Rest of the World
The AquaBeam system has CE marking in Europe and is approved in over 30 countries including Australia, Canada, Japan, and several Middle Eastern and South Asian markets. Availability is growing year-on-year, but many regional centers still do not have access. Your urologist or hospital should be able to confirm whether the platform is operational at their facility — and if not, refer you to the nearest one.
How to Ask Your Urologist
If you think you might be a candidate, the most useful conversation to have at your consultation is the trade-off conversation. Ask directly: “Given my prostate size, my IPSS score, and my priorities — how would you compare TURP, HoLEP, and aquablation for me specifically?” A good urologist will not push you toward whichever procedure they personally do most. They will walk you through the actual trade-offs in your case, including whether aquablation is available locally and whether your insurance or system will cover it. If your local center does not offer aquablation but it is genuinely the best option for you, ask about referral pathways to a center that does.
→ Related Read: UroLift and Rezum — Minimally Invasive BPH Options ExplainedFrequently Asked Questions
Is aquablation therapy better than TURP?
Aquablation therapy delivers symptom relief comparable to TURP at 5 years in the WATER trial, but with a substantially lower rate of retrograde ejaculation (about 10% vs. 65–75%). For men who want to preserve ejaculation, aquablation is the stronger choice. For men who prioritize the longest possible track record, immediate availability, and lowest cost, TURP remains a reasonable option. There is no universal “better” — the right choice depends on prostate size, your priorities, and what your local center can offer. Read more about when surgery is appropriate for BPH.
How long does it take to recover from aquablation?
Most men spend one night in hospital, have the catheter removed within 1 to 3 days, and return to desk work within 5 to 7 days. Heavy lifting and strenuous exercise should be avoided for 2 to 4 weeks. Sexual activity is usually cleared at 4 to 6 weeks. Full symptom benefit is reached by around 3 months as the prostate fully heals. Light blood in the urine for up to 2 weeks afterward is normal and expected. The recovery curve is broadly similar to TURP recovery, slightly faster on average.
Will aquablation therapy affect my erections or ejaculation?
Erections are very rarely affected by aquablation, because the nerves responsible for erection sit outside the prostate and are not in the surgical field. Ejaculation is preserved in roughly 90% of men — a major advantage over standard TURP and HoLEP, which cause retrograde (dry) ejaculation in 65–80% of cases. This protection comes from the planning step, where the surgeon excludes the area around the verumontanum from the treatment zone. Discuss your specific anatomy with your urologist, since the planning approach can be individualized.
Is aquablation suitable for very large prostates?
Aquablation has solid evidence for prostates up to 150 grams, with the strongest data set in the 30 to 80 gram range. For prostates larger than 150 grams, HoLEP at an experienced center currently has the longer track record. The advantage of aquablation in large glands is that operative resection time stays roughly constant regardless of prostate size — a 100 gram gland takes about the same waterjet time as a 50 gram one, which is not true for TURP.
How much does aquablation therapy cost?
In the United States, aquablation has been covered by Medicare since 2023 and by most major commercial insurers. Out-of-pocket costs for uninsured patients typically run from $9,000 to $20,000 USD depending on the hospital and region. In the United Kingdom, NICE-approved aquablation is being commissioned at selected NHS centers at no patient cost; private aquablation in the UK runs roughly £8,000 to £15,000. In other countries, availability and cost vary widely — your urologist’s office is the best place to confirm both whether the platform is available locally and what coverage applies to you.
Is the prostate tissue sent to pathology after aquablation?
Yes. The tissue removed by the waterjet is washed out through the resectoscope, collected, and sent for histopathological examination — exactly the same as with TURP and HoLEP. This is important because around 5 to 10 percent of men undergoing BPH surgery turn out to have an incidental small focus of prostate cancer in the removed tissue. Sending tissue to pathology is one of the reasons we continue to prefer resection-based BPH surgery over tissue-ablation alternatives like Rezum or UroLift in men with rising or borderline PSA values. For more on PSA interpretation, see the grey-zone PSA guide.
📚 References
- National Institute for Health and Care Excellence. Robotically assisted transurethral waterjet ablation for lower urinary tract symptoms caused by benign prostatic hyperplasia. NICE Interventional Procedures Guidance IPG748. 2023. NICE Guidance
- Gilling P, Reuther R, Kahokehr A, Fraundorfer M. Aquablation — image-guided robot-assisted waterjet ablation of the prostate: initial clinical experience. BJU International. 2016;117(6):923-929. PubMed
- Gilling P, Barber N, Bidair M, et al. WATER: A double-blind, randomized, controlled trial of aquablation vs transurethral resection of the prostate in benign prostatic hyperplasia. Journal of Urology. 2018;199(5):1252-1261. PubMed
- Gilling P, Barber N, Bidair M, et al. Five-year outcomes for aquablation therapy compared to TURP: results from a double-blind, randomized trial in men with LUTS due to BPH. Canadian Journal of Urology. 2022;29(1):10960-10968. PubMed
- Bach T, Giannakis I, Bachmann A, et al. Aquablation of the prostate: single-center results of a non-selected, consecutive patient cohort. World Journal of Urology. 2019;37(7):1369-1375. PubMed
- Gilling P, Mackey M, Cresswell M, Kennett K, Kabalin J, Fraundorfer M. Holmium laser versus transurethral resection of the prostate: a randomized prospective trial with 1-year followup. Journal of Urology. 1999;162(5):1640-1644. PubMed
- Bhojani N, Bidair M, Zorn KC, et al. Aquablation for benign prostatic hyperplasia in large prostates (80–150 cc): 1-year results. Urology. 2019;129:1-7. PubMed
- Sandhu JS, Bixler BR, Dahm P, et al. Management of Lower Urinary Tract Symptoms Attributed to Benign Prostatic Hyperplasia (BPH): AUA Guideline Amendment 2023. Journal of Urology. 2024;211(1):11-19. AUA Guidelines
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.




