Is it Erectile Dysfunction (ED) and Heart Disease? Why Morning Wood is a ‘Check Engine’ Light
Patients usually brush off fading morning erections as an inevitable, harmless part of getting older. The truth is, your body uses those erections as a biological "check engine" light. Losing them often signals blocked arteries three to five years before a heart attack strikes. Here is exactly why this vascular warning happens, and the cardiac screenings you need to prioritize before simply asking for a pill.

Here’s something most men don’t know — and most primary care doctors don’t mention: erectile dysfunction is not just a bedroom problem. It’s a cardiovascular warning sign. Research consistently shows that ED can precede a heart attack or stroke by 3 to 5 years [1]. That’s not a coincidence. It’s biology giving you advance notice. Erectile dysfunction and heart disease? both are interrelated.
If you’ve noticed that your morning erections have become less frequent, less firm, or have disappeared entirely — that’s not “just aging.” Morning wood (technically called nocturnal penile tumescence) is a barometer of your vascular health. When it fades, something is changing inside your blood vessels. Those are the exact same blood vessels that supply your heart and brain.
As a urologist, I see men every week who come in embarrassed about ED and leave with a referral for cardiac screening — screening that sometimes identifies arterial blockages before they become life-threatening emergencies. Here is the clinical breakdown of why this happens, what you should watch for, and the immediate next steps you need to take.
📋 Key Takeaways
- ED Erectile Dysfuction and heart disease share the same underlying cause: endothelial dysfunction — damage to the inner lining of blood vessels
- Penile arteries are 1–2 mm wide (about 1/16 inch) — they clog before your coronary arteries (3–4 mm), giving you an earlier cardiovascular warning
- Loss of regular morning erections is one of the earliest signs of vascular ED
- Men with ED have a 2× higher risk of heart attack and 1.5× higher risk of death from all cardiovascular causes [2]
- Every man presenting with ED should have blood pressure, fasting glucose, and a lipid profile checked — this is standard of care, not optional
- The good news: addressing cardiovascular risk factors often improves ED too — sometimes without medication
The Link Between Erectile Dysfunction and Heart Disease (The Biology)
To understand the link between erectile dysfunction and heart disease and why ED predicts heart disease, you need to understand one concept: endothelial dysfunction.
The endothelium is the thin inner lining of every blood vessel in your body. When it’s healthy, it produces nitric oxide — a molecule that relaxes blood vessel walls, allowing blood to flow freely. An erection is essentially a hydraulic event: nitric oxide causes the penile arteries to dilate, blood rushes in, and the penis becomes rigid. No nitric oxide, no erection.
Here’s the critical point: the same endothelial damage that prevents your penile arteries from dilating is also happening in your coronary arteries, your cerebral arteries, and your peripheral arteries. The difference is size.
Penile arteries are only 1–2 mm in diameter (about 1/16 inch). Coronary arteries are 3–4 mm (1/8 inch). The carotid arteries in your neck are 5–7 mm (about 1/4 inch). Atherosclerotic plaque and endothelial damage affect the smallest arteries first. This is why ED often appears years before a cardiac event — it’s the same disease process, but the narrower pipes clog first [3].
This concept is sometimes called the “artery size hypothesis” and it’s now well-established in cardiovascular and urological literature. A landmark meta-analysis published in Circulation: Cardiovascular Quality and Outcomes found that ED increased the risk of cardiovascular events by 44% and all-cause mortality by 25% [2].
Your erection is a canary in the coal mine for your cardiovascular system.
→ Try the Tool: ED Vascular Risk Screener — see your 5-year cardiac riskThe Loss of Morning Wood: Your Earliest Warning Sign
Morning erections — nocturnal penile tumescence (NPT) — occur during REM sleep, typically 3 to 5 times per night in healthy men. You notice them in the morning because you wake up during or just after a REM cycle. They are not caused by sexual arousal or a full bladder, despite what most men believe.
Morning erections are a vascular health check your body performs automatically every night. They test whether your endothelium is producing adequate nitric oxide and whether blood flow to the penis is sufficient. When morning erections become less frequent, less rigid, or disappear entirely, it suggests the underlying mechanism — vascular health — is deteriorating.
This distinction matters enormously clinically. A man who gets normal morning erections but struggles during sex likely has a psychological or situational cause. A man who has lost morning erections has an organic problem — vascular, hormonal, or neurological — that needs investigation. Morning erections are purely physiological; unlike sexual erections, they are unaffected by performance anxiety or relationship dynamics [4].
→ Self-Assessment: IIEF-5 Erectile Function Score (5 questions, 2 minutes)Vascular ED: Why It Is Rarely “Just Stress”
The frustrating reality for many men is that they’re told ED is “just stress” or “just age” without any investigation. While psychological factors absolutely play a role — especially in younger men — the majority of ED in men over 40 has an organic component.
Vascular (60–80% of cases in men over 50)
Atherosclerosis, hypertension, diabetes, dyslipidemia, and smoking all damage the endothelium. These are the same risk factors for heart attack and stroke. If you have ED plus any of these risk factors, your cardiovascular system needs attention — not just your erection.
Hormonal (5–15% of cases)
Low testosterone (hypogonadism) can cause ED, reduced libido, fatigue, and mood changes. However, testosterone alone is rarely the sole cause of ED in older men — it usually coexists with vascular disease. A total testosterone level below 8 nmol/L (230 ng/dL) warrants consideration of replacement therapy, but only after confirming with a repeat morning sample and checking LH, FSH, and prolactin [5].
→ Related Read: Low Testosterone Over 40 — Signs Your Doctor Might MissNeurological (10–15%)
Conditions affecting nerve pathways — diabetic peripheral neuropathy, multiple sclerosis, spinal cord injury, radical prostatectomy, and pelvic surgery — can impair the nerve signals needed for erection. Diabetic neuropathy is particularly common and often overlooked as a contributing factor alongside the vascular component in diabetic men.
Medication-Related (significant but often missed)
Several commonly prescribed medications can cause or worsen ED. The most frequent culprits include:
- Beta-blockers (atenolol, metoprolol) — among the worst offenders for ED
- Thiazide diuretics (hydrochlorothiazide) — can worsen ED, especially at higher doses
- SSRIs and SNRIs (sertraline, fluoxetine, venlafaxine) — cause both ED and delayed ejaculation
- 5-alpha reductase inhibitors (finasteride, dutasteride) — used for BPH and hair loss, can cause persistent sexual dysfunction
- Spironolactone — anti-androgen effects at higher doses
If ED began or worsened after starting a new medication, that connection must be discussed with your prescribing doctor. Often, switching to an alternative within the same drug class (for example, nebivolol instead of atenolol for blood pressure, or an ACE inhibitor instead of a thiazide) resolves the problem without sacrificing disease control.
Psychological (20–30% in younger men, often mixed in older men)
Performance anxiety, depression, relationship conflict, work stress, and pornography-related desensitization are real causes — especially in men under 40. However, even in these cases, I always check baseline cardiovascular risk factors. The two categories are not mutually exclusive. A man can have mild vascular compromise made significantly worse by performance anxiety. Treating only one misses half the picture.
The Cardiac Workup: What Every Man with ED Needs Checked
If you have ED — regardless of your age — these investigations should be considered. If your doctor prescribed Viagra without checking any of these, they’ve treated the symptom and missed the disease.
Essential Investigations (every man with ED)
- Blood pressure measurement — undiagnosed hypertension is common and directly causes endothelial damage and ED
- Fasting glucose and HbA1c — diabetes is the single strongest independent risk factor for ED. Up to 50% of diabetic men develop ED [6]
- Lipid profile (total cholesterol, LDL, HDL, triglycerides) — dyslipidemia accelerates atherosclerosis in penile and coronary arteries equally
- Morning total testosterone — drawn between 7–11 AM (testosterone is highest in the morning; afternoon samples are misleadingly low)
- BMI and waist circumference — central obesity is a modifiable risk factor for both ED and cardiovascular disease. A waist over 102 cm (40 inches) in men is a major risk marker
Additional Investigations (in specific cases)
- Thyroid function — both hypo- and hyperthyroidism can affect erectile function
- Prolactin — if testosterone is low and libido is severely reduced (may indicate a pituitary adenoma)
- Penile Doppler ultrasound — if vascular ED is suspected and surgical or injection therapy is being considered; measures arterial inflow and venous leak
- Cardiac risk score (Framingham, ASCVD, or QRISK3) — should be calculated for every man over 40 with ED, particularly with two or more cardiovascular risk factors
Treatment: A Urologist’s Approach (Not Just “Take a Pill”)
The treatment of ED should be layered, starting with the most impactful and least invasive approach. Too many men jump straight to PDE5 inhibitors without addressing the underlying cause. Here’s the systematic approach I use in clinic — and the one that’s also outlined in my step-by-step ED treatment protocol.
Step 1: Address the Cardiovascular Risk Factors — Always First
This is not optional. It’s the foundation. If a man has uncontrolled hypertension, diabetes, obesity, or dyslipidemia, treating the ED without addressing these is like mopping the floor while the tap is running. A randomized trial published in JAMA found that one-third of obese men with ED restored normal function through lifestyle changes alone, with no medication [7]. Exercise improving endothelial function has been shown to be as effective as PDE5 inhibitors in mild ED [8]. Smoking cessation improves erectile function within 6–12 months of stopping.
Step 2: PDE5 Inhibitors — First-Line Medical Therapy
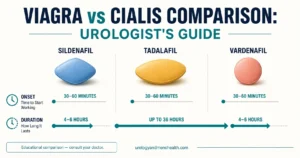
If lifestyle modification alone isn’t sufficient — or while waiting for it to take effect — PDE5 inhibitors remain the first-line pharmacological treatment. They work by enhancing the nitric oxide pathway, allowing blood vessels in the penis to dilate more effectively. For a detailed comparison of the four available options, see my Viagra vs Cialis vs Sildenafil comparison guide.
- Sildenafil (Viagra) — the original, well-studied option. Take 30–60 minutes before activity. Lasts 4–6 hours. Absorption is reduced with fatty meals. Now widely available as an affordable generic
- Tadalafil (Cialis) — longer-acting (up to 36 hours), can be taken daily at low dose (2.5–5 mg) for spontaneous function. Often my first choice because it removes the need to “plan ahead” and has additional benefits for men with concurrent BPH symptoms
- Vardenafil (Levitra) and Avanafil (Stendra) — alternatives with slightly different onset times and side effect profiles
Critical safety point: PDE5 inhibitors are absolutely contraindicated with nitrate medications (nitroglycerin spray or tablets, isosorbide mononitrate). The combination can cause life-threatening hypotension. This is why cardiovascular assessment before prescribing is essential — not a formality. The Princeton III Consensus provides the framework most urologists and cardiologists use to risk-stratify men with cardiovascular disease before prescribing [12]. Response rate to PDE5 inhibitors is approximately 60–70% overall, but drops significantly in men with diabetes (around 50%) or after radical prostatectomy without nerve-sparing (15–30%) [9].
Step 3: Second-Line Therapies
- Intracavernosal injections (alprostadil, trimix) — self-injection directly into the penis. Sounds alarming but is highly effective (85–90% success rate) and relatively painless with proper technique. Used extensively in post-prostatectomy rehabilitation
- Vacuum erection devices (VED) — non-invasive. A cylinder creates negative pressure, drawing blood into the penis. A constriction ring maintains the erection. Requires practice and partner cooperation but is medication-free
- Intraurethral alprostadil (MUSE) — a small pellet inserted into the urethra. Less invasive than injection but also less effective; useful in men unwilling to self-inject
Step 4: Penile Prosthesis — The Definitive Surgical Option
For men who have failed or cannot tolerate all other treatments, a penile implant (inflatable penile prosthesis, IPP) is the definitive solution. Modern three-piece inflatable devices provide excellent rigidity for intercourse and complete flaccidity when not in use. Patient and partner satisfaction rates exceed 90% in published series [10]. This is a specialized urological procedure requiring a surgeon with specific implant experience.
Download Your Free Clinical Action Plan
Enter your email below to download Dr. Khalid’s complete Evidence-Based ED Action Plan as a free, printable PDF.
The Age Factor: What’s Normal and What Isn’t
ED becomes more common with age, but it is never a normal or inevitable part of aging. The Massachusetts Male Aging Study found that approximately 40% of men in their 40s, 50% in their 50s, 60% in their 60s, and 70% in their 70s reported some degree of erectile difficulty [11]. These numbers are often cited to normalize ED, but they mask a critical detail: in each age group, the men with ED have significantly higher rates of undiagnosed cardiovascular disease.
Age correlates with ED primarily because age correlates with accumulated vascular damage. A healthy, active 65-year-old non-smoker with normal blood pressure and no diabetes will have dramatically better erectile function than a sedentary 50-year-old with metabolic syndrome. If you have ED at any age, investigate it. Do not accept “you’re just getting older” as an explanation without investigation.
💡 In My Practice
The most common pattern I see is a man in his late 40s or 50s who has been ignoring gradually worsening erections for 1–2 years before coming in. Almost invariably, when I check his blood pressure it’s elevated. His fasting glucose is borderline or frankly diabetic. His cholesterol hasn’t been checked in years. He came in about ED, but what we actually found was undiagnosed cardiovascular disease hiding in plain sight.
The other pattern that concerns me is younger men — late 20s, early 30s — presenting with situational ED who’ve already self-prescribed sildenafil bought online without any medical assessment. These men usually have performance anxiety, sometimes compounded by excessive pornography use, but without checking baseline testosterone and fasting glucose, we can’t be certain we’re not missing something organic. Online sildenafil also bypasses the single most important conversation: do you take nitrates? That conversation, in person, has prevented more than one near-miss in my career.
The takeaway I give every patient: ED is a symptom, not a verdict. It tells me something about your blood vessels, your hormones, and your nervous system. It is not a referendum on your masculinity. The men who do best are the ones who treat it as the early-warning sign it is — and act before the next, larger event.
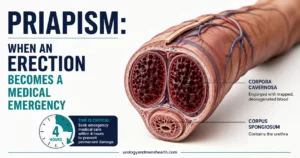
⚠️ When to See a Doctor — Urgently
- Chest pain, shortness of breath, or palpitations alongside ED — may indicate active cardiac disease requiring immediate evaluation before any ED treatment is started
- ED that developed suddenly (over days rather than months) — could indicate a neurological event, acute medication side effect, or acute hormonal change requiring urgent assessment
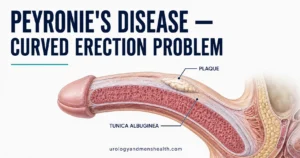
- Painful erection or penile curvature developing over time — may indicate Peyronie’s disease, which requires separate specialist evaluation
- Known diabetes with new-onset ED — warrants formal vascular and neuropathy assessment alongside cardiovascular risk screening
- ED after starting a new medication — do NOT stop medication without consulting your prescribing doctor first, but always report the symptom promptly
- ED accompanied by loss of libido, fatigue, and mood changes — this triad suggests hypogonadism (low testosterone) requiring blood testing
Frequently Asked Questions
Does having ED always mean I have heart disease?
No. ED has multiple causes — psychological, hormonal, neurological, and medication-related. But in men over 40, vascular disease is by far the most common contributing factor. The key point is that ED should prompt a cardiovascular risk assessment, not that every man with ED has heart disease. Think of it as a reason to check, not a diagnosis in itself. That check may come back completely normal — but it could also catch something important early. The ED Vascular Risk Screener can give you a starting point before your appointment.
I’m 35 with ED — should I worry about my heart?
At 35, psychological causes and lifestyle factors — poor sleep, stress, excess alcohol, smoking, obesity — are more likely than established vascular disease. However, early-onset atherosclerosis does occur, especially with a family history of heart disease or diabetes. A baseline check of blood pressure, fasting glucose, and lipids is sensible at any age. It takes 10 minutes and costs very little. It could also genuinely save your life if something is found early. Quantify your ED first with the IIEF-5 so you have a baseline number to track.
Can exercise really improve erections?
Yes, and the evidence is strong. A meta-analysis of 11 trials found that aerobic exercise significantly improved erectile function, with effects comparable to PDE5 inhibitors in mild-to-moderate ED. The mechanism is direct: exercise improves endothelial function, reduces systemic inflammation, improves insulin sensitivity, and modestly boosts testosterone. Walking briskly for 30 minutes five times a week is sufficient to see meaningful improvement within 2–3 months. This is the same lifestyle pillar I describe in my full ED treatment protocol.
Is Viagra (sildenafil) safe if I have heart disease?
PDE5 inhibitors (sildenafil, tadalafil) are safe for most men with stable cardiovascular disease — and in fact they have mild beneficial effects on blood pressure and cardiac workload. The one absolute contraindication is concurrent use of nitrate medications (nitroglycerin spray, isosorbide mononitrate). The combination can cause a life-threatening drop in blood pressure. If you take nitrates for angina, PDE5 inhibitors must be avoided. For all other cardiac patients, they are generally safe when prescribed after a proper clinical assessment. See my side-by-side comparison for help choosing between them.
My morning erections are fine but I can’t perform during sex — is it vascular?
Almost certainly not. If morning erections are normal — full, regular, and firm — the vascular and neurological machinery is working. The problem is almost certainly psychological (performance anxiety, relationship stress, situational). This is actually reassuring — it means the plumbing is intact. A conversation with your urologist about the psychological component, and potentially a referral to a psychosexual therapist, is often the most effective next step rather than medication.
📚 References
- Montorsi P, Ravagnani PM, Galli S, et al. Association between erectile dysfunction and coronary artery disease: matching the right target with the right test in the right patient. Eur Urol. 2006;50(4):721–731. PubMed
- Vlachopoulos CV, Terentes-Printzios DG, Ioakeimidis NK, Aznaouridis KA, Stefanadis CI. Prediction of cardiovascular events and all-cause mortality with erectile dysfunction: a systematic review and meta-analysis of cohort studies. Circ Cardiovasc Qual Outcomes. 2013;6(1):99–109. PubMed
- Montorsi F, Briganti A, Salonia A, et al. Erectile dysfunction prevalence, time of onset and association with risk factors in 300 consecutive patients with acute chest pain and angiographically documented coronary artery disease. Eur Urol. 2003;44(3):360–365. PubMed
- Yafi FA, Jenkins L, Albersen M, et al. Erectile dysfunction. Nat Rev Dis Primers. 2016;2:16003. PubMed
- Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018;103(5):1715–1744. PubMed
- Kouidrat Y, Pizzol D, Cosco T, et al. High prevalence of erectile dysfunction in diabetes: a systematic review and meta-analysis of 145 studies. Diabet Med. 2017;34(9):1185–1192. PubMed
- Esposito K, Giugliano F, Di Palo C, et al. Effect of lifestyle changes on erectile dysfunction in obese men: a randomized controlled trial. JAMA. 2004;291(24):2978–2984. PubMed
- Gerbild H, Larsen CM, Graugaard C, Areskoug Josefsson K. Physical activity to improve erectile function: a systematic review of intervention studies. Sex Med. 2018;6(2):75–89. PubMed
- Salonia A, Bettocchi C, Boeri L, et al. EAU Guidelines on Sexual and Reproductive Health: Erectile Dysfunction. European Association of Urology. 2024. EAU Guidelines
- Bettocchi C, Palumbo F, Spilotros M, et al. Patient and partner satisfaction after AMS inflatable penile prosthesis implant. J Sex Med. 2010;7(1 Pt 1):304–309. PubMed
- Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol. 1994;151(1):54–61. PubMed
- Nehra A, Jackson G, Miner M, et al. The Princeton III Consensus recommendations for the management of erectile dysfunction and cardiovascular disease. Mayo Clin Proc. 2012;87(8):766–778. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.