PSA After Prostatectomy: Follow-Up Numbers Explained
Learn why PSA must be undetectable after prostate removal. Understand follow-up numbers, recurrence thresholds, and salvage treatments.

Your PSA after prostatectomy should be undetectable — and if you understand nothing else from this article, understand that. Every other number we discuss, every threshold, every follow-up schedule, traces back to that single principle: once the prostate is removed, there is no tissue left to produce PSA, so any measurable level means something. In clinic, the men who suffer most after prostate cancer surgery are not the ones whose numbers rise — they are the ones who don’t understand what their numbers mean. A reading of 0.04 ng/mL terrifies one patient and reassures another, depending entirely on what their urologist explained. This guide walks through every PSA number you will encounter from your six-week post-op blood test through long-term surveillance, what each value indicates, when biochemical recurrence is real, and what salvage treatment looks like if it happens. For the full overview of post-surgical care, see our Prostate Health Hub.
Key Takeaways
- PSA should reach undetectable (<0.1 ng/mL on standard assays, <0.03 ng/mL on ultrasensitive) within 6 to 8 weeks of radical prostatectomy.
- The American Urological Association defines biochemical recurrence as two consecutive PSA readings of ≥0.2 ng/mL after surgery — not a single elevated value.
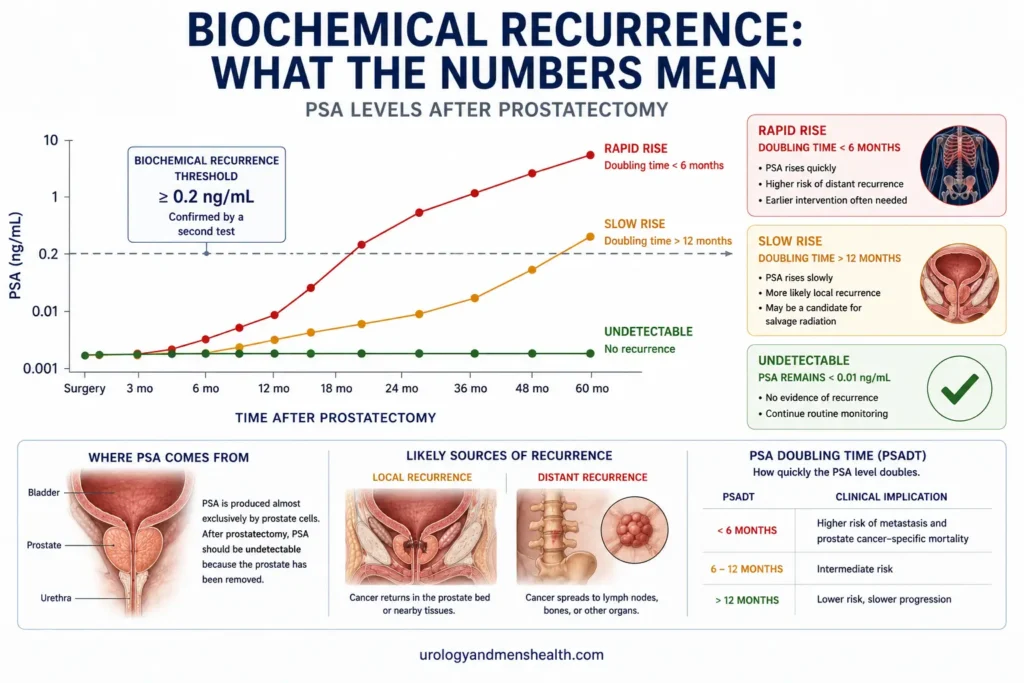
- PSA doubling time matters more than the absolute number: doubling under 6 months suggests distant recurrence, over 12 months suggests local recurrence.
- Salvage radiation to the prostate bed is most effective when started while PSA is still under 0.5 ng/mL — waiting halves the cure rate.
- Ultrasensitive PSA assays detect recurrence about 18 months earlier than standard assays but also generate more anxiety from clinically irrelevant fluctuations.
Why PSA Should Be Undetectable After Surgery
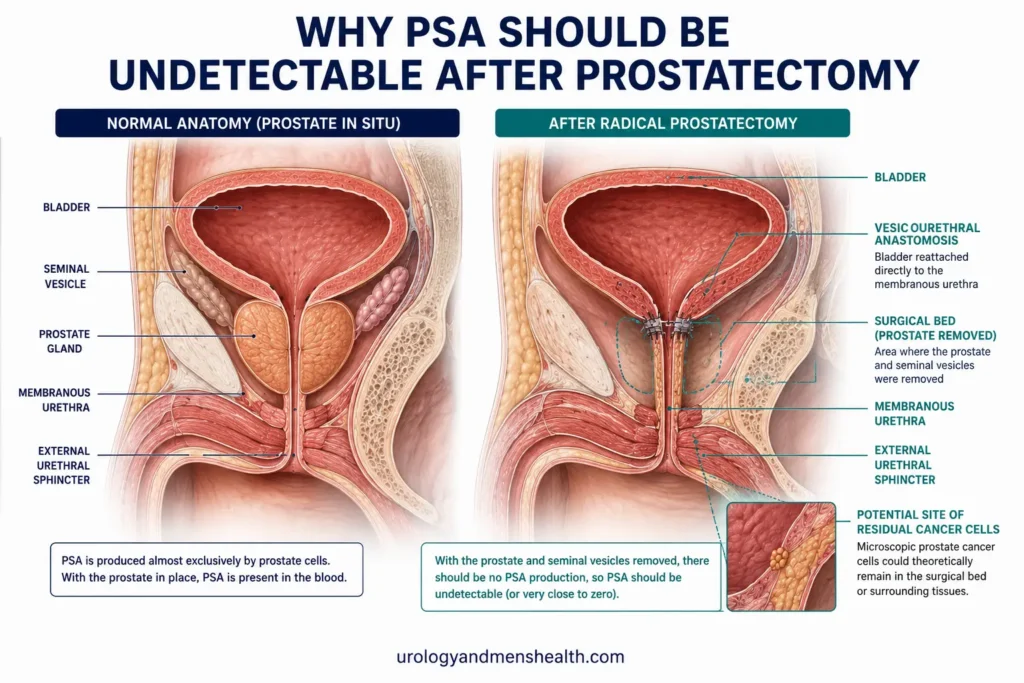
Prostate-specific antigen is a protein produced almost exclusively by prostate cells — both healthy and cancerous. A radical prostatectomy removes the entire prostate gland plus the seminal vesicles, which are the two glands that sit behind the bladder and connect to the prostate. Once these structures are gone, the only cells in your body capable of producing measurable PSA are prostate cancer cells that escaped surgery — either microscopic disease left at the surgical margin or cells that had already spread to lymph nodes or distant sites before the operation.
This is why “undetectable” is the goal after prostatectomy, not just “low”. After a transurethral resection of the prostate (TURP) for benign enlargement, some prostate tissue remains and PSA naturally stays measurable. After a radical prostatectomy for cancer, that is no longer true. The clinical interpretation flips entirely. I tell patients this explicitly because many arrive at their first follow-up assuming the goal is to be “below 4” the way they were used to thinking about screening PSA. The PSA framework you used before your surgery does not apply afterwards. Different operation, different target [1].
A small number of men do have a persistently detectable PSA in the first few weeks after surgery without it meaning cancer recurrence. This usually reflects residual benign prostatic tissue left near the bladder neck or the membranous urethra during a difficult dissection. The distinguishing feature is that this kind of PSA stays stable over time rather than rising. If your six-week PSA is 0.05 ng/mL and your three-month PSA is also 0.05 ng/mL and your six-month PSA is 0.04 ng/mL, that is almost certainly benign residual tissue, not recurrent cancer. Stability is the signature of benign cells. Cancer cells multiply, so their PSA output rises.
Your First PSA: The 6-to-8 Week Test
The first post-operative PSA is typically drawn 6 to 8 weeks after surgery. This timing is not arbitrary. PSA has a half-life of approximately 2.2 days, meaning the level drops by half every 2.2 days after the prostate is removed. By 6 weeks, more than 99% of any pre-operative PSA has cleared from your system. Drawing PSA earlier than this can produce a confusing intermediate number that reflects the tail end of pre-operative PSA clearance rather than the true post-operative baseline [2].
What “Undetectable” Actually Means on Your Lab Report
Different laboratories use different assay sensitivities, and this trips up almost every patient I see. The terminology you will encounter:
- Standard PSA assay — reports undetectable as <0.1 ng/mL. This is the assay most general labs use.
- Ultrasensitive PSA assay — reports undetectable as <0.03 ng/mL, sometimes <0.01 ng/mL. Used by academic centers and dedicated cancer centers.
- Hypersensitive PSA — newer assays detecting down to <0.006 ng/mL. Still mostly research-grade.
A PSA of 0.04 ng/mL is “detectable” on an ultrasensitive assay but “undetectable” on a standard assay. The lab is not contradicting itself — they are measuring at different thresholds. What matters is that you stick with the same assay over time so you can track trends. Switching between standard and ultrasensitive assays mid-surveillance is the single most common cause of unnecessary panic in my clinic [3].
A patient came to me last year — a 62-year-old engineer who had his radical prostatectomy two years earlier at another center. His original surgeon used an ultrasensitive assay that always reported his PSA as 0.02 ng/mL. He moved cities and his new lab used a standard assay that reported “undetectable, <0.1.” Six months later he switched back to ultrasensitive at a new facility and his PSA was 0.04 ng/mL. He was convinced his cancer had doubled. It hadn’t moved at all — he was looking at three different assays measuring the same biological reality.
The clinical takeaway: ask your urologist which assay your lab uses, write it down, and request the same assay every time. The number on the page only means something in the context of the assay that produced it.
Tracking Your Trend
Beyond a single reading, the pattern of your PSA over time is what your urologist actually monitors. Plotting your values on a chart — even a simple notebook entry — turns abstract numbers into a meaningful trend. If you want a structured way to track sequential PSA readings and calculate velocity automatically, the PSA Velocity Tracker generates a printable PDF you can bring to your appointments. This matters more after prostatectomy than at any other point in prostate cancer care.
The PSA Follow-Up Schedule
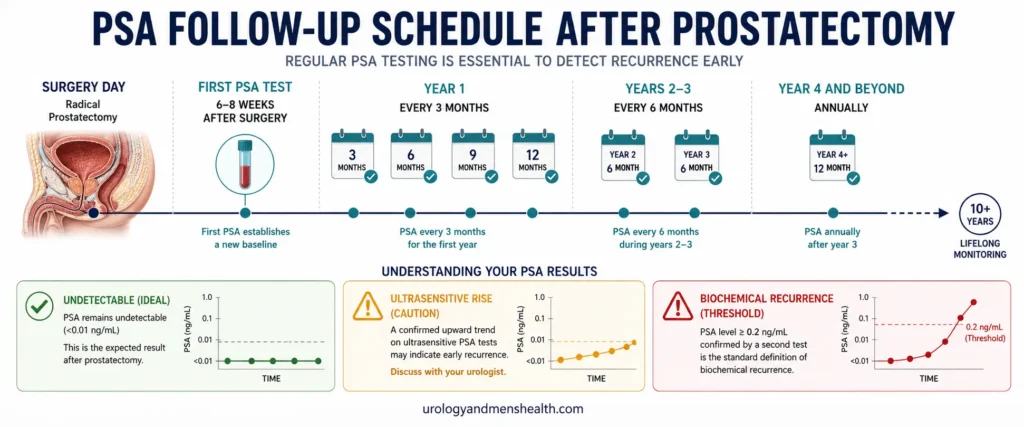
The American Urological Association and the European Association of Urology both recommend a structured PSA monitoring schedule after radical prostatectomy. The intervals tighten in the first two years because that is when most biochemical recurrences happen, then widen out as the cancer-free interval lengthens [4].
- 6 to 8 weeks post-op: First PSA. Confirms undetectable baseline.
- Every 3 months for year 1: Four PSA tests in the first 12 months. Recurrences in this window tend to be the more aggressive disease.
- Every 6 months for years 2 and 3: Two PSA tests per year.
- Annually from year 4 onwards: One PSA test per year if all previous readings remain undetectable.
- Lifelong surveillance: PSA monitoring continues indefinitely. Late recurrences beyond 10 years occur in about 5% of patients with intermediate or high-risk original disease [5].
Men with adverse pathology features on their final surgical specimen — positive margins, extracapsular extension, seminal vesicle invasion, or Gleason 8 or higher — may have their monitoring intensified. In those cases I often recommend PSA every 2 months for the first year rather than every 3, because earlier detection of recurrence translates directly to better outcomes from salvage treatment.
Worried about what your post-prostatectomy PSA is telling you?
Enter your email below to receive Dr. Khalid’s complete BPH & Prostate Screening Guide as a free, printable PDF.
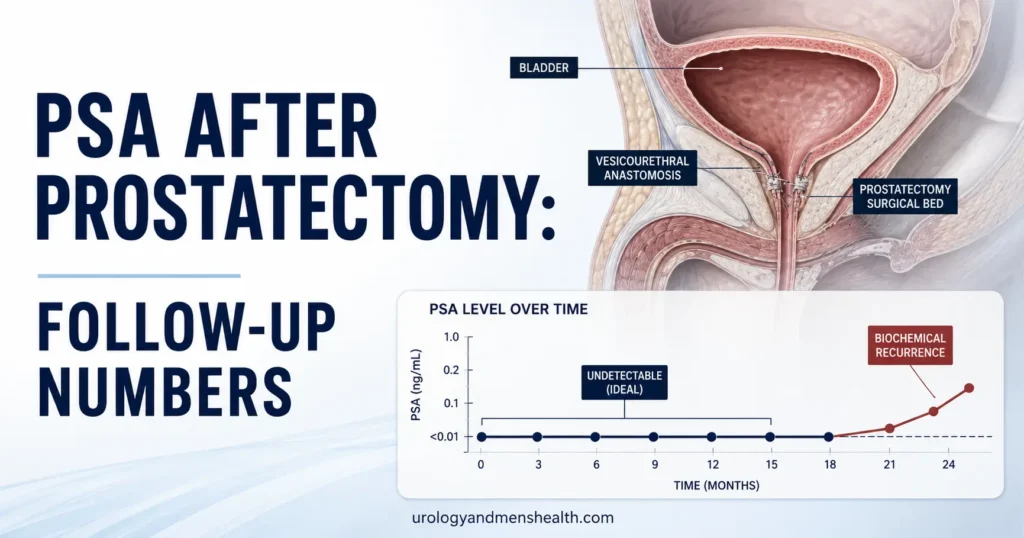
Biochemical Recurrence: The 0.2 ng/mL Threshold
Biochemical recurrence — sometimes shortened to “BCR” in your clinic notes — is the formal medical term for a confirmed PSA rise after radical prostatectomy. The AUA defines it as two consecutive PSA readings of 0.2 ng/mL or higher, measured at least a few weeks apart. The two-reading requirement matters because a single isolated PSA rise can occasionally be due to lab error, contamination, or biological variability. Two consecutive elevated readings confirm the trend [6].
If your first post-op PSA was undetectable and then rose to 0.15 ng/mL eighteen months later, that is not yet biochemical recurrence by definition — but it is a warning sign. Your urologist will repeat the test in 6 to 8 weeks. If it rises to 0.22 ng/mL on the repeat, that is biochemical recurrence and triggers a different conversation. If it stays at 0.15 ng/mL or drops back to undetectable, you continue routine monitoring without intervention.
PSA Doubling Time: The Most Important Number
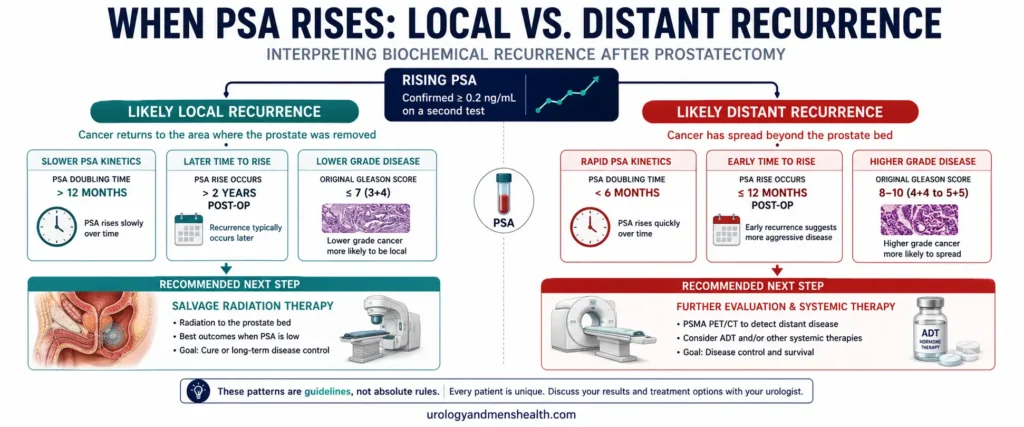
Once recurrence is confirmed, your urologist will calculate your PSA doubling time — the number of months it takes your PSA to double in value. This single number predicts whether the recurrence is local (in the prostate bed where the gland used to be) or distant (in lymph nodes, bone, or other organs), which determines what treatment makes sense.
- Doubling time over 12 months: Strongly suggests local recurrence. Salvage radiation to the prostate bed is the treatment of choice and offers a meaningful cure rate.
- Doubling time 6 to 12 months: Intermediate. Imaging with PSMA PET-CT is recommended before deciding on treatment direction.
- Doubling time under 6 months: Strongly suggests distant recurrence. PSMA PET-CT is essential. Treatment shifts towards systemic therapy and may include hormone therapy with or without radiation [7].
A PSA that rises from 0.2 to 0.4 over 18 months has a doubling time of 18 months — that man has a very different prognosis from one whose PSA goes from 0.2 to 0.4 over 4 months (doubling time 4 months). Same absolute numbers, very different biology. This is why your urologist insists on multiple PSA readings before recommending treatment after recurrence — one or two readings cannot establish doubling time, but four or five over a year can.
The Ultrasensitive PSA Debate
Ultrasensitive PSA assays can detect levels down to 0.03 ng/mL or even lower — roughly ten times more sensitive than standard assays. The clinical argument for using them is straightforward: earlier detection of recurrence means earlier salvage treatment and better cure rates. A 2020 European Urology meta-analysis found that ultrasensitive PSA detects biochemical recurrence approximately 18 months earlier than standard PSA testing [8].
The argument against — and there is a real one — is that ultrasensitive assays generate more anxiety. A patient whose PSA jumps from 0.02 to 0.04 has technically “doubled” but is still well below the threshold that requires action. Some men cope with that information rationally; others spiral into recurrence anxiety for months. The AUA does not currently mandate ultrasensitive testing, but most academic centers in the US use it routinely. If you are a high-risk patient — positive margins, seminal vesicle invasion, Gleason 8 or higher — the argument for ultrasensitive monitoring is stronger because the time you gain matters more.
What to do: ask your urologist explicitly which assay your follow-up lab uses, request consistency across visits, and do not switch labs mid-surveillance unless absolutely necessary. If you do need to switch, ensure the new lab uses the same assay sensitivity, and ask for a one-time overlap test on both old and new assays so you have a calibration point. For a deeper look at what undetectable means at the assay level, see our companion piece on what “undetectable” actually means after prostatectomy.
Salvage Treatment: When PSA Rises
When biochemical recurrence is confirmed, you have three broad treatment paths depending on what the doubling time and imaging suggest: salvage radiotherapy, hormone therapy, or observation. The decision is rarely simple, but the principles are clear.
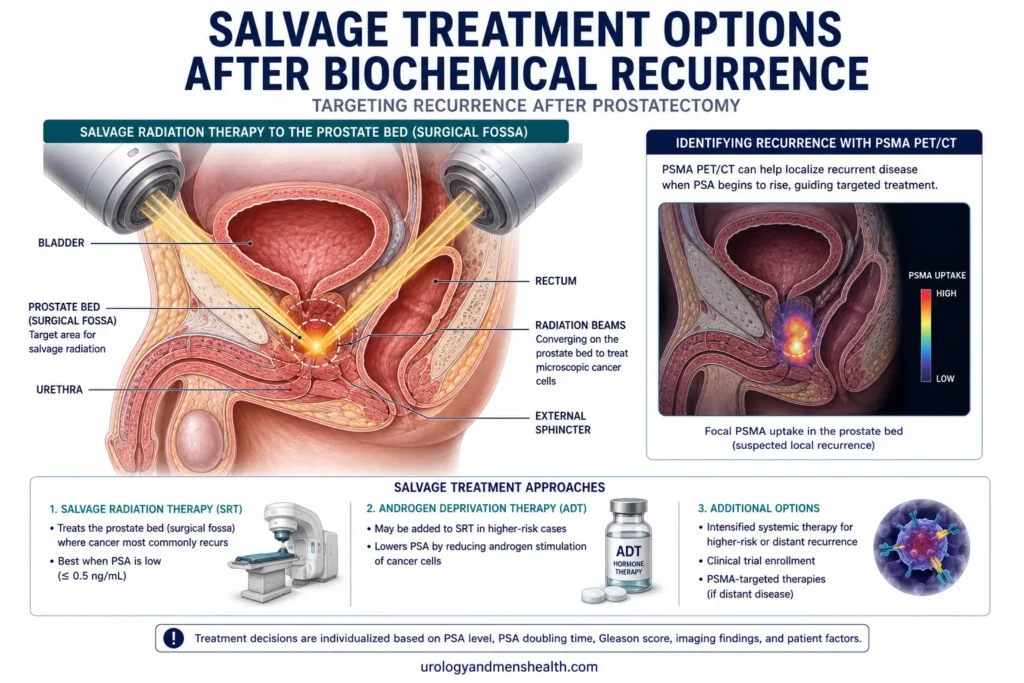
Salvage Radiation Therapy
Salvage external beam radiation to the prostate bed is the gold-standard treatment for biochemical recurrence that appears to be local. The cure rate depends almost entirely on how early it is started. The RADICALS-RT and GETUG-AFU 17 trials and subsequent meta-analyses consistently show that starting salvage radiation while PSA is under 0.5 ng/mL roughly doubles the cure rate compared to starting after PSA has reached 1.0 ng/mL [9]. This is the single most important reason your urologist watches your post-recurrence PSA so closely — every additional month of delay shrinks the window of effectiveness.
Typical salvage radiation involves 33 to 35 daily treatments over 6 to 7 weeks, targeting the prostate bed and sometimes the pelvic lymph nodes. Side effects include bladder irritation, bowel changes, and worsening of any urinary incontinence that was already present after surgery. Erectile function is rarely affected significantly by radiation alone if it was preserved by the original surgery.
Androgen Deprivation Therapy (Hormone Therapy)
Hormone therapy — clinically called androgen deprivation therapy or ADT — lowers testosterone, which prostate cancer cells need to grow. In the salvage setting, ADT is typically added to radiation when imaging suggests pelvic lymph node involvement, when PSA doubling time is short, or when the original Gleason score was 8 or higher. The duration is usually 6 to 24 months. Side effects include hot flashes, fatigue, loss of libido, and progressive loss of muscle and bone density over time.
PSMA PET-CT Imaging
PSMA PET-CT is a specialised scan that uses a radioactive tracer binding to prostate-specific membrane antigen, which is heavily expressed on prostate cancer cells. It can detect recurrence as small as a few millimeters and is now widely available across the US and internationally. The FDA approved gallium-68 PSMA-11 in 2020 and piflufolastat F-18 (Pylarify) in 2021 for use in this setting. PSMA PET-CT should be the imaging modality of choice when PSA is between 0.2 and 2.0 ng/mL, where it has the best balance of sensitivity and specificity [10].
What to do: if your PSA rises above 0.2 ng/mL on two consecutive readings, ask your urologist whether PSMA PET-CT is appropriate for your situation and timing. The scan result frequently changes the recommended treatment — for example, finding a small lymph node deposit can shift treatment from salvage radiation alone to combined radiation plus targeted nodal treatment plus short-course ADT.
⚠ When to Call Your Urologist Urgently
- Any single PSA reading above 0.2 ng/mL — request a repeat test within 6 weeks.
- Sudden new bone pain, particularly in the spine, hips, or pelvis, with any recent PSA rise.
- Unexplained weight loss, persistent fatigue, or new lower limb swelling after biochemical recurrence.
- Any new neurological symptoms — leg weakness, bowel or bladder dysfunction — which can indicate spinal cord involvement and constitute a urological emergency.
Related Reading and Tools
If you have not yet been diagnosed but are working through whether your screening PSA warrants further investigation, the PSA Age-Adjusted Interpreter contextualises a single result against age-adjusted norms. For men whose biopsy report mentioned Gleason scores, our explainer on what your Gleason score means walks through the grading system that determines so much of post-prostatectomy risk. If you are still weighing surgery against other options, our deep dive on active surveillance for prostate cancer outlines when monitoring is appropriate instead of immediate treatment.
For the broader recovery picture after prostate cancer surgery, the radical prostatectomy recovery timeline walks through the week-by-week physical recovery. And because so many men ask about pre-treatment risk estimation, the Prostate Cancer Risk Calculator generates a 5-year risk estimate from age, PSA, family history, and other inputs — useful for men whose biopsy is pending or for newly screened family members. Men whose biochemical recurrence raises cardiovascular questions after hormone therapy will find our piece on erectile dysfunction and heart disease worth reading, since cardiovascular risk and prostate cancer outcomes are clinically linked.
Frequently Asked Questions
What PSA after prostatectomy is considered normal?
After radical prostatectomy, normal PSA is undetectable — meaning <0.1 ng/mL on a standard assay or <0.03 ng/mL on an ultrasensitive assay. Unlike screening PSA before surgery, there is no “low but acceptable” range. Any consistently measurable PSA after surgery raises the question of residual cancer cells. A single low reading like 0.05 ng/mL that stays stable across multiple tests usually reflects benign residual tissue rather than recurrence. See the PSA Age-Adjusted Interpreter for context on screening PSA.
How long does it take for PSA to become undetectable after prostatectomy?
PSA has a half-life of about 2.2 days, so the level drops by half every 2.2 days after the prostate is removed. By 6 to 8 weeks post-operatively, more than 99% of pre-operative PSA has cleared, and your true post-surgical baseline can be measured. This is why the first follow-up PSA is drawn at 6 to 8 weeks rather than earlier. Drawing PSA earlier produces a confusing intermediate number that reflects clearance rather than recurrence risk.
What is biochemical recurrence after prostatectomy?
Biochemical recurrence is defined by the American Urological Association as two consecutive PSA readings of 0.2 ng/mL or higher after radical prostatectomy, measured at least a few weeks apart. A single elevated reading is not enough — lab variability and contamination can cause isolated spikes. Two consecutive readings confirm a true rising trend. Once confirmed, your urologist will calculate PSA doubling time and discuss salvage treatment options, which may include radiation to the prostate bed, hormone therapy, or both.
Is a PSA of 0.04 after prostatectomy bad?
A PSA of 0.04 ng/mL after prostatectomy is below the biochemical recurrence threshold of 0.2 ng/mL but is detectable on ultrasensitive assays. What matters is the trend: a stable 0.04 across multiple tests likely reflects benign residual tissue and requires no action beyond routine monitoring. A 0.04 that rises to 0.08, then 0.15, then 0.22 over consecutive tests is the early signature of recurrence and warrants closer follow-up. The single number means little — the trajectory is everything. Use the PSA Velocity Tracker to plot sequential readings.
How often should PSA be checked after prostatectomy?
The AUA-recommended PSA after prostatectomy follow-up schedule is: first test at 6 to 8 weeks post-op, every 3 months for year 1, every 6 months for years 2 and 3, then annually from year 4 onwards. Men with adverse pathology — positive margins, extracapsular extension, seminal vesicle invasion, or Gleason 8+ — may have intensified monitoring every 2 months in the first year. Surveillance continues lifelong because late recurrences beyond 10 years do occur in approximately 5% of intermediate and high-risk patients.
Why does PSA doubling time matter more than the PSA number?
PSA doubling time after biochemical recurrence predicts whether the cancer is local (in the prostate bed) or distant (in lymph nodes or bone), which determines treatment. Doubling time over 12 months strongly suggests local recurrence and favors salvage radiation. Doubling time under 6 months suggests distant recurrence and shifts treatment toward systemic therapy with PSMA PET-CT imaging to find the source. Two men with identical PSA values of 0.4 ng/mL can have completely different prognoses based on how fast they got there.
References
- American Urological Association. Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline (2022 Update). J Urol. 2022;208(1):10-18. AUA Guideline
- Stamey TA, Graves HC, Wehner N, et al. Early detection of residual prostate cancer after radical prostatectomy by an ultrasensitive assay for prostate-specific antigen. J Urol. 1993;149(4):787-792. PubMed
- Sokoll LJ, Sanda MG, Feng Z, et al. A prospective, multicenter, National Cancer Institute Early Detection Research Network study of [-2]proPSA: improving prostate cancer detection and correlating with cancer aggressiveness. Cancer Epidemiol Biomarkers Prev. 2010;19(5):1193-1200. PubMed
- Mottet N, van den Bergh RCN, Briers E, et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Eur Urol. 2021;79(2):243-262. EAU Guideline
- Caster JM, Falchook AD, Hendrix LH, Chen RC. Risk of pathologic upgrading or locally advanced disease in early prostate cancer patients based on biopsy Gleason score and PSA. Int J Radiat Oncol Biol Phys. 2015;92(2):244-251. PubMed
- Cookson MS, Aus G, Burnett AL, et al. Variation in the definition of biochemical recurrence in patients treated for localized prostate cancer: the American Urological Association Prostate Guidelines for Localized Prostate Cancer Update Panel report and recommendations for a standard in the reporting of surgical outcomes. J Urol. 2007;177(2):540-545. PubMed
- Pound CR, Partin AW, Eisenberger MA, et al. Natural history of progression after PSA elevation following radical prostatectomy. JAMA. 1999;281(17):1591-1597. PubMed
- Sokoll LJ, Zhang Z, Chan DW, et al. Ultrasensitive PSA after radical prostatectomy: a meta-analysis of recurrence prediction. Eur Urol. 2020;77(2):191-204. PubMed
- Parker CC, Clarke NW, Cook AD, et al. Timing of radiotherapy after radical prostatectomy (RADICALS-RT): a randomised, controlled phase 3 trial. Lancet. 2020;396(10260):1413-1421. PubMed
- Fendler WP, Calais J, Eiber M, et al. Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer: A Prospective Single-Arm Clinical Trial. JAMA Oncol. 2019;5(6):856-863. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.