The kidney stone size chart that radiologists and urologists use isn’t fancy — it’s a single number that decides almost everything that happens next. A 3 mm stone and a 15 mm stone are different diagnoses with different timelines and different outcomes. One has a 90% chance of passing in your urine on its own, often within two weeks. The other has essentially zero chance and will need surgery. Most patients walk out of the emergency room with a CT report stating “4 mm distal ureteral calculus” and no real understanding of what that means for the next month of their life.
I see this every week in clinic — patients holding a piece of paper with a measurement in millimeters and asking the same question: how long do I wait, and when do I stop waiting? The answer follows a clear, evidence-based framework set out by the American Urological Association (AUA) and the European Association of Urology (EAU). This article is that framework, size by size, with the same recommendations I give my own patients.
Key Takeaways
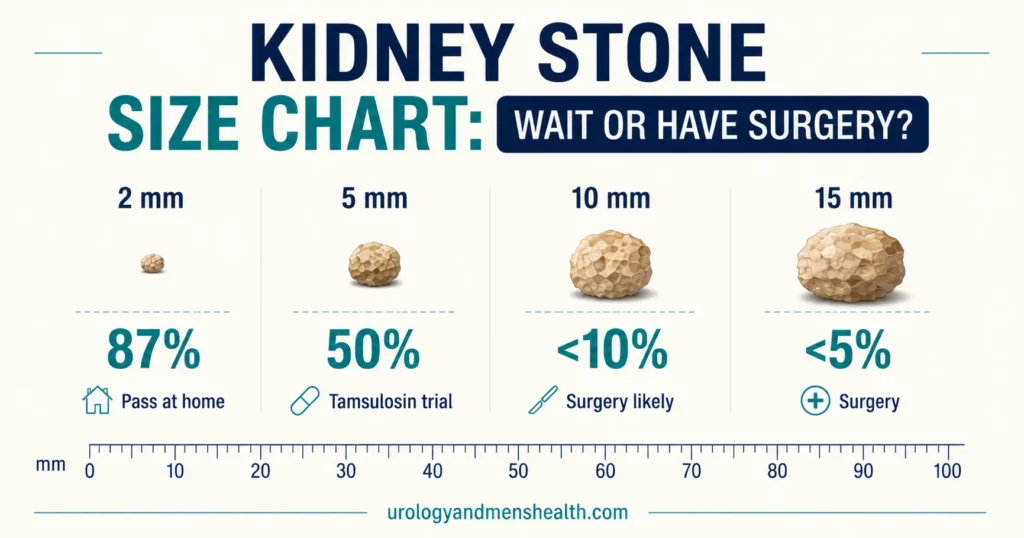
- Stones under 5 mm (about 1/5 inch) have a 68–98% spontaneous passage rate; most are managed at home with hydration and NSAIDs.
- Stones 5–10 mm are the decision-making zone — passage rates drop to 25–53%, and tamsulosin (medical expulsive therapy) is added to push the odds higher.
- Stones over 10 mm (about 2/5 inch) have a less than 5% chance of passing — surgery is the answer, not more waiting.
- Stone location matters as much as size — a 7 mm stone near the bladder passes more easily than a 7 mm stone near the kidney.
- The maximum window for conservative management is 4–6 weeks; waiting longer with an obstructing stone risks permanent kidney damage even after pain stops.
- For ureteral stones the procedure is usually ureteroscopy (URS) with laser; for stones over 20 mm or staghorn stones it’s PCNL; ESWL and RIRS are alternatives in specific situations.
In This Guide:
The Kidney Stone Size Chart: Passage Rates at a Glance
Here is the size-by-size framework I use in clinic — the same one recommended by the AUA 2024 Surgical Management of Stones guideline and the EAU 2024 Urolithiasis guideline [1]. The numbers come from large meta-analyses of patients followed from CT diagnosis to either spontaneous passage or surgery [2].
- Under 5 mm (1/5 inch): 68–98% pass on their own. Conservative management. Average wait 1–2 weeks.
- 5–10 mm: 25–53% pass. Tamsulosin trial. Maximum wait 4–6 weeks.
- Over 10 mm (2/5 inch): Less than 5% pass. Surgery is the answer.
If you want a fast estimate of your own odds based on size and location, I built a calculator that uses the same Jendeberg passage data — try the Kidney Stone Passage Calculator before you read on.
Under 5 mm: The “Watch and Wait” Zone
When I see a sub-5 mm stone on a CT report, my first conversation with the patient is almost always reassurance. Jendeberg and colleagues published the largest contemporary dataset on this question and found spontaneous passage rates of 87% for stones under 3 mm and 76% for stones 3–5 mm [2]. Average passage time is 1–2 weeks; some take up to 4 weeks. The job in this band is to keep the patient comfortable while the body does the work.
The conservative management protocol I prescribe
Hydration: Drink 2.5–3 liters of fluid daily (about 85–100 fl oz, or 10–12 cups) spread across the day. The goal is high urine flow to push the stone along the ureter — not gulping a gallon in one sitting.
Pain control: NSAIDs are first-line because they reduce ureteral inflammation and spasm at the same time as treating pain. I use ibuprofen 400 mg three times daily with food or diclofenac 50 mg three times daily. Acetaminophen (paracetamol) can be added. Opioids — tramadol or codeine — are reserved for breakthrough pain when NSAIDs alone aren’t enough, and only short-term.
Medical expulsive therapy (MET): Both AUA 2024 and EAU 2024 guidelines state that MET is optional for stones under 5 mm because the absolute benefit is modest at this size [1]. I prescribe tamsulosin 0.4 mg daily for distal ureteral stones in the 4–5 mm range; for very small stones I usually don’t bother.
Strain your urine: Use a fine-mesh strainer (a coffee filter works at home) over the toilet to catch the stone when it passes. Send it for chemical analysis — knowing whether it’s calcium oxalate, uric acid, or struvite changes the prevention plan completely. If you’re not sure where to start, the Kidney Stone Composition Identifier gives you a starting point based on appearance and risk factors.
Related Read: How to Pass a Kidney Stone Fast — What I Tell My Patients5–10 mm: The Grey Zone Where Decisions Get Hard
This is where clinical judgment matters most. A stone in this size band can pass on its own — but the probability is much lower and the time to passage is longer. Hollingsworth and colleagues, in a meta-analysis still cited in the current AUA guideline, found passage rates of 53% for stones 5–7 mm and around 25–40% for stones 7–10 mm [3]. Within that range, where the stone sits in the ureter is almost as important as how big it is.
Distal ureter (lower third, near the bladder): Passage rates are highest here — up to 75% for 5–7 mm stones. The distal ureter is the narrowest part anatomically but also has the strongest peristaltic squeeze and the most alpha-receptors, which is why tamsulosin works best here.
Mid-ureter: Passage rates drop. The mid-ureter crosses the iliac vessels in the pelvis, creating a physiological narrowing that can trap stones for weeks.
Proximal ureter (upper third, near the kidney): Passage rates are lowest. A 7 mm stone at the pelvi-ureteric junction (PUJ — where the kidney meets the ureter) has a far worse chance of passing than a 7 mm stone at the vesicoureteric junction (VUJ — where the ureter meets the bladder).
Medical expulsive therapy (MET) — what tamsulosin actually does
Tamsulosin 0.4 mg daily is the standard MET. It’s an alpha-blocker that relaxes the smooth muscle of the distal ureter, widening it and dampening spasm. The 2018 Cochrane meta-analysis by Campschroer and colleagues found that tamsulosin increases passage rates by approximately 30% for stones 5–10 mm and shortens the time to passage [4]. I prescribe it routinely in this size range when conservative management is being attempted. It’s well tolerated — the main side effect men ask about is retrograde ejaculation, which is reversible when the drug stops.
When to convert to surgery
If a stone hasn’t progressed after 4–6 weeks of conservative management on follow-up imaging — or if the patient develops fever, intractable pain, or a rising creatinine at any point — ask your urologist to schedule URS or ESWL within the next 2 weeks. Prolonged obstruction beyond 6 weeks risks permanent nephron loss even when the pain has settled [5]. Pain stopping is not the same thing as the stone passing.
Your stone is in the 5–10 mm zone? Don’t lose the next month to guesswork.
Enter your email below to receive Dr. Khalid’s complete 7-Day Kidney Stone Prevention Meal Plan — the same evidence-based dietary framework I give patients to stop the next stone before it forms.
Over 10 mm: When Surgery Is the Answer
Stones larger than 10 mm have a less than 5% chance of passing on their own. Trying conservative management at this size wastes time and risks the kidney. The surgical decision then comes down to which procedure — and that depends on stone size, exact location, density on CT (Hounsfield Units), and your kidney anatomy. The four contemporary procedures, briefly:
URS (ureteroscopy with laser lithotripsy)
The most commonly performed stone surgery worldwide. A thin scope is passed through the urethra and bladder up to the stone in the ureter; a holmium or thulium laser fragments it on the spot. Suitable for ureteral stones of any size and kidney stones up to 15–20 mm. Stone-free rates exceed 90% for ureteral stones. A double-J (DJ) ureteral stent is usually placed for 1–2 weeks afterward to keep the ureter open while it heals.
ESWL (extracorporeal shockwave lithotripsy)
Non-invasive — focused shockwaves delivered from outside the body break the stone into fragments that the patient then passes. Best for kidney stones 5–15 mm that aren’t too dense (under about 1,000 Hounsfield Units on the planning CT). Success rates are 70–80% in well-selected stones. ESWL underperforms for hard calcium oxalate monohydrate stones, cystine stones, and lower-pole kidney stones over 10 mm [6].
PCNL (percutaneous nephrolithotomy)
The standard procedure for large kidney stones (over 20 mm) and staghorn stones. A small tract is created through the back into the kidney; the stone is fragmented and removed through this channel. More invasive than URS or ESWL but far more effective for high stone burden — stone-free rates exceed 90% even for complex stones in a single procedure.
RIRS (retrograde intrarenal surgery)
A flexible ureteroscope passed up through the ureter into the kidney itself, used to laser-fragment stones in difficult locations — lower-pole calyces, calyceal diverticula. Increasingly used as an alternative to ESWL for kidney stones 10–20 mm, especially hard stones or lower-pole stones where ESWL performs poorly [7].
Choosing between URS, ESWL, PCNL, and RIRS is the most common decision conversation I have with patients. To see how the four compare on stone-free rates, recovery time, and risks for your stone size, the Urology Surgery Comparison Tool gives a side-by-side breakdown.
Related Read: URS, PCNL, RIRS — Which Kidney Stone Surgery Is Right for You?When Stone Size Isn’t the Whole Story
Size is the strongest single predictor of passage, but it isn’t the only one. Several other factors push the decision earlier toward surgery — sometimes regardless of how big the stone is.
Stone location: Distal ureteral stones pass more readily than proximal stones of the same size. A 6 mm stone at the VUJ behaves clinically like a 4 mm stone elsewhere.
Degree of obstruction: A partially obstructing stone may be watched. A completely obstructing stone causing hydronephrosis (visible kidney swelling on CT) gets a tighter timeline and lower threshold for intervention.
Infection — this is the emergency: An infected, obstructed kidney (a stone blocking the ureter plus a urinary tract infection or fever) is a urological emergency, full stop. The treatment is immediate drainage — either a ureteral stent placed cystoscopically or a percutaneous nephrostomy tube placed by interventional radiology — together with intravenous antibiotics. Definitive stone removal happens once infection is controlled. Delay in drainage in this scenario is one of the few urological situations where a patient can die within 48 hours [8].
Solitary kidney: If you have only one functioning kidney — congenitally, after donation, or after previous surgery — the threshold for intervention is far lower. Prolonged obstruction in a solitary kidney carries disproportionate risk because there is no contralateral compensation.
Renal function: A rising creatinine or falling eGFR during a stone episode is a hard trigger for earlier intervention. Obstruction-driven nephron loss is silent — patients often feel no worse even as kidney function drops. If you have pre-existing high blood pressure, the kidneys are already under load; combining hypertension with an obstructing stone accelerates damage. The relationship is covered in detail in High Blood Pressure and Your Kidneys: The Silent Damage.
Patient factors: Pain tolerance, occupation (a pilot, a long-haul truck driver, or a surgeon cannot afford weeks of unpredictable pain episodes), and prior stone history all factor into the shared decision. A patient on their fifth stone has different priorities to a patient on their first.
Related Read: Kidney Stones — Complete Guide from a UrologistIn My Practice
The 5–10 mm range is where I spend the most time in clinic. The conversation I have most often is with a patient sitting in front of me holding a CT report with a 6 mm distal ureteral stone, no fever, controllable pain, normal kidney function on the affected side. That patient is a textbook candidate for a 4-week trial of tamsulosin and a follow-up CT KUB. The conversation is short and the patient leaves with a plan. The harder conversation is the one I have a few weeks later with the patient whose stone hasn’t moved on the follow-up scan — because the natural human response is to ask for another month, and the natural urological response is to say no.
The rule I follow is uncomplicated: if there is no progress on imaging at 4 weeks, I offer surgery. Waiting beyond 6 weeks with a persistently obstructing stone is not conservative management — it is neglect of the kidney. Patients sometimes feel I am being too aggressive at that point; I would rather have that conversation than the one where I am explaining why their kidney function dropped and didn’t recover.
When to See a Doctor — Urgently
- Fever with a known or suspected kidney stone — infected obstruction is a life-threatening emergency. Go to the ER, do not wait.
- Inability to urinate at all — may indicate bilateral obstruction or obstruction in a solitary kidney; this is also an emergency.
- Pain not controlled by oral painkillers — you need ER assessment and IV analgesia, not stronger tablets at home.
- No progress after 4–6 weeks on follow-up imaging — prolonged obstruction risks permanent nephron loss even if pain has settled.
- Rising creatinine or falling eGFR on bloodwork — the obstruction is causing measurable kidney damage and intervention is now urgent.
Frequently Asked Questions
Can a 7 mm kidney stone pass on its own?
It’s possible but unlikely without help. The spontaneous passage rate for a 7 mm stone is about 25–40%, depending on location — better in the distal ureter near the bladder, worse in the proximal ureter near the kidney. Tamsulosin (medical expulsive therapy) improves the odds modestly. If a 7 mm stone hasn’t moved on follow-up imaging at 4 weeks, surgery is usually recommended to prevent kidney damage from continued obstruction. To estimate your specific odds based on size and location, use the Kidney Stone Passage Calculator.
How long is too long to wait for a stone to pass?
The AUA 2024 and EAU 2024 guidelines both set a maximum of 4–6 weeks of conservative management for an obstructing ureteral stone before intervention is recommended [1]. Beyond that window, even if pain has stopped, persistent obstruction can cause irreversible kidney damage. A pain-free patient is not necessarily a stone-free patient — the stone can simply have become impacted in a less symptomatic position. Follow-up imaging is non-negotiable to confirm passage versus the need for surgery.
Should I take tamsulosin for a 4 mm stone?
For a 4 mm stone in the distal ureter, I usually do prescribe tamsulosin 0.4 mg daily, even though current AUA and EAU guidelines call MET optional at this size. The downside is small — mild dizziness in some patients, occasional retrograde ejaculation (reversible) — and the upside is a meaningful reduction in time-to-passage. For very small stones (under 3 mm), the absolute benefit is too small to bother. For stones 4–5 mm, especially distal, I treat. For stones 5–10 mm, the answer is definitely yes — the tamsulosin for kidney stones article covers the dosing, duration, and side-effect profile in more detail.
Does stone composition affect passage?
Composition has a smaller effect on passage than size and location, but it changes the surgical decision. Hard stones (calcium oxalate monohydrate, cystine) fragment poorly with ESWL and usually need laser via URS instead. Uric acid stones can sometimes be dissolved by alkalinizing the urine with potassium citrate — sometimes avoiding surgery entirely. Struvite (infection) stones nearly always need complete surgical removal because they harbor bacteria that won’t clear with antibiotics alone. The Kidney Stone Composition Identifier can give you a starting estimate based on appearance and risk factors.
My CT says my stone is 4 mm but my pain is severe — why?
Pain severity has almost no relationship with stone size. A tiny 2 mm stone causing acute obstruction and ureteral spasm can produce identical pain to a 10 mm stone. The pain comes from ureteral distension and stretching of the renal capsule caused by obstruction, not from the stone itself. A small stone moving through one of the ureteral narrowings can be excruciating; a larger stone sitting quietly in the kidney often causes no symptoms at all. This is why we rely on the CT measurement and the location, not the pain score, to decide on treatment.
References
- Assimos D, Krambeck A, Miller NL, et al. Surgical Management of Stones: AUA/Endourological Society Guideline (2024 amendment). J Urol. 2024;211(5):717–731. AUA Guidelines
- Jendeberg J, Geijer H, Alshamari M, Cierzniak B, Lidén M. Size matters: the width and location of a ureteral stone accurately predict the chance of spontaneous passage. Eur Radiol. 2017;27(11):4775–4785. PubMed
- Hollingsworth JM, Rogers MA, Kaufman SR, et al. Medical therapy to facilitate urinary stone passage: a meta-analysis. Lancet. 2006;368(9542):1171–1179. PubMed
- Campschroer T, Zhu X, Vernooij RW, Lock MT. Alpha-blockers as medical expulsive therapy for ureteral stones. Cochrane Database Syst Rev. 2018;4(4):CD008509. PubMed
- Frokiær J. Pathophysiology of urinary tract obstruction. In: Partin AW, Dmochowski RR, Kavoussi LR, Peters CA, eds. Campbell-Walsh-Wein Urology. 12th ed. Philadelphia: Elsevier; 2021:1257–1290.
- Türk C, Petřík A, Sarica K, et al. EAU Guidelines on Urolithiasis (2024 update). Eur Urol. 2024 (in press); summary in Eur Urol. 2016;69(3):475–482. EAU Guidelines
- Breda A, Territo A, López-Martínez JM. Benefits and risks of ureteral access sheaths during retrograde intrarenal surgery. Curr Opin Urol. 2018;28(3):245–250. PubMed
- Borofsky MS, Walter D, Shah O, Goldfarb DS, Mues AC, Makarov DV. Surgical decompression is associated with decreased mortality in patients with sepsis and ureteral calculi. J Urol. 2013;189(3):946–951. PubMed

Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.