The Kidney Stone Diet: My Clinical Protocol for Prevention
When patients want to stop forming kidney stones, their very first instinct is usually to completely cut calcium from their diet. That is the single biggest dietary mistake I see, and it actually guarantees you will form more stones. Here is the exact, guideline-backed clinical protocol I prescribe to stop recurrences, stripping away the internet folklore to tell you what actually works.

“What should I eat to stop getting stones?” — I hear this kidney stone diet question at least three times a week in clinic. And almost every time, the patient has already started doing the exact wrong thing: cutting out calcium. That single misconception causes more recurrent stones than any other dietary mistake I see.
The truth is that kidney stone prevention through diet is not complicated — but it is counterintuitive. Most of the advice circulating online is either outdated, oversimplified, or flat-out wrong. As a urologist who manages stone disease daily, I’m going to share the exact dietary protocol I give my patients — the same approach backed by the American Urological Association and European Association of Urology guidelines.
This isn’t generic “drink more water” advice. This is a structured, stone-type-specific prevention plan that has kept the majority of my compliant patients stone-free. If you’ve had one kidney stone, your risk of a second is roughly 50% within the next five years [1]. That number drops dramatically with the right dietary strategy.
📋 Key Takeaways
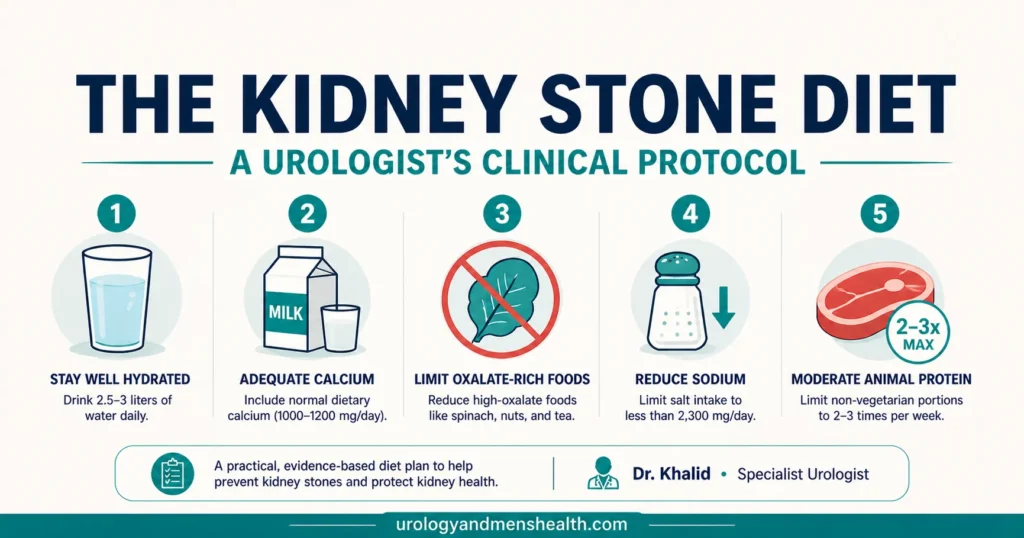
- Do NOT cut calcium — dietary calcium binds oxalate in your gut and actually prevents stones. Low-calcium diets increase stone risk by roughly 50%.
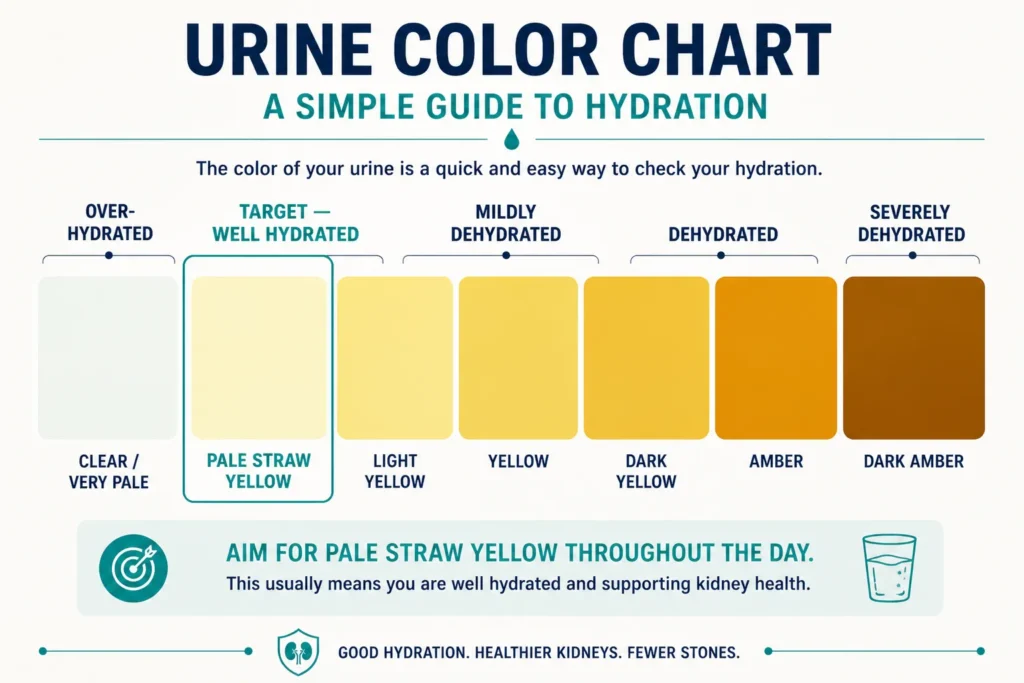
- Hydration is the single most impactful intervention — aim for 2.5+ liters of urine output daily (about 85 fl oz / 10 cups), with pale yellow urine as your visual check.
- Sodium is a hidden stone-former — every extra gram of salt you eat pushes about 40 mg of calcium into your urine.
- Oxalate restriction matters, but only for calcium oxalate stone formers — and only the top 8 highest-oxalate foods make a meaningful difference.
- Animal protein excess drives uric acid stones and worsens calcium stones — limit red meat to 2–3 servings per week.
- Citrate from lemons and oranges is a natural stone inhibitor — daily citrus intake is one of the easiest preventive measures.
- Prevention must be tailored to YOUR stone type — a kidney stone diet that prevents calcium oxalate stones is different from one that prevents uric acid stones.
Step 1: Know Your Stone Type (Everything Else Depends on This)
This is where most prevention strategies fail before they start. A patient passes a stone, gets treated, and is told to “drink more water.” No stone analysis. No metabolic workup. No targeted strategy. That’s like prescribing antibiotics without knowing which bacteria you’re treating.
If you’ve passed or had a stone removed, it should have been sent for chemical composition analysis. If it wasn’t — and this happens far too often — ask your urologist about a 24-hour urine metabolic evaluation, which can identify your risk profile even without the stone itself.
Here’s why stone type matters for diet:
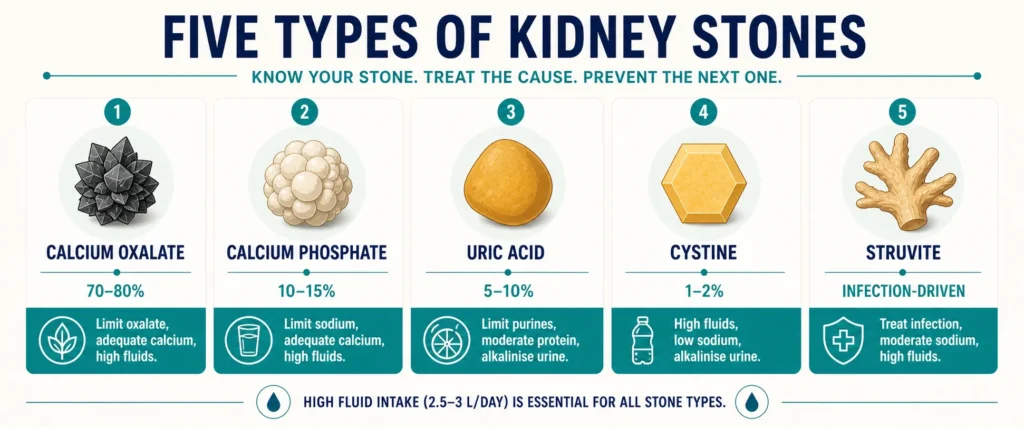
- Calcium oxalate (70–80% of stones): Reduce oxalate, increase dietary calcium, reduce sodium, increase citrate.
- Calcium phosphate (10–15%): Similar to oxalate approach, but also need to address urine pH (often too alkaline).
- Uric acid (5–10%): Reduce purines, alkalize urine with citrate, limit fructose — very different approach from calcium stones.
- Cystine (1–2%): Aggressive hydration and alkalization — genetic condition requiring specialist management.
- Struvite: Diet has minimal role — these are infection-driven and require complete surgical removal plus antibiotic treatment.
The protocol below focuses primarily on calcium oxalate stones (since they’re overwhelmingly the most common) with a dedicated section for uric acid stone prevention. If you don’t yet know your stone type, a simple risk calculator can help you understand your odds before getting a metabolic workup.
→ Related Read: Kidney Stones — Complete Guide from a Urologist🧮 Try the Tool: 5-Year Kidney Stone Risk ProfilerStep 2: Hydration — The Non-Negotiable Foundation
If you do nothing else from this entire article, do this: drink enough fluid to produce at least 2.5 liters of urine per day (about 85 fl oz / 10 cups). This single intervention reduces stone recurrence by 40–50% [4]. Nothing else you eat or avoid comes close to this impact.
For most adults, that means drinking approximately 3 to 3.5 liters of total fluid daily (about 100–120 fl oz). But there are nuances that matter.
What to drink
- Water — the gold standard. Still or sparkling, doesn’t matter. Tap water is fine in most developed countries.
- Lemon water — an excellent choice. The citrate in lemon juice inhibits stone formation. Squeeze half a lemon into a glass of water, 2–3 times daily. This provides meaningful dietary citrate without needing supplements.
- Orange juice — also a good citrate source, though higher in calories and sugar. One glass daily is reasonable.
- Herbal teas — fine, but be cautious with high-oxalate varieties (see below).
What to limit or avoid
- Black tea — one of the highest dietary sources of oxalate. A common hidden culprit in countries where heavy tea drinking is the norm (South Asia, UK, Middle East). If you drink 4–6 cups of black tea daily, this alone can significantly raise urinary oxalate. Switch to green tea or herbal alternatives.
- Sugar-sweetened beverages — the fructose in soft drinks and commercial juices increases urinary calcium and uric acid excretion. Cola also contains phosphoric acid. One large prospective study (Nurses’ Health Study) found that sugary drinks raised stone risk by 23–33% [5].
- Excessive coffee — moderate coffee (2–3 cups/day) is actually slightly protective. Excessive intake may contribute to dehydration if you’re not compensating with water.
- Beer and spirits — alcohol is a net dehydrator. The popular myth that “beer flushes out stones” is dangerous nonsense. Beer also contains purines that raise uric acid.
The timing trick most people miss
Hydration isn’t just about total volume — it’s about consistency throughout the day. Most stones form overnight when urine is most concentrated (you don’t drink while sleeping). The practical fix: drink a full glass of water before bed and again if you wake during the night. This single habit addresses the highest-risk window for crystal formation.
How do you know if you’re drinking enough? Your urine should be pale straw yellow. If it’s dark yellow or amber, you’re under-hydrated. If it’s completely clear and colorless, you may actually be over-hydrating — which is unnecessary and can wash out protective electrolytes. To make this concrete, my Hydration Calculator will give you a personalized daily fluid target based on your weight, climate, and activity level.
→ Related Read: Hydration & Kidney Health — The Water Myth vs. What Science Shows🧮 Try the Tool: Hydration Calculator for Stone PreventionStep 3: The Calcium Paradox — Why You Must NOT Cut Dairy
This is the most counterintuitive part of kidney stone prevention, and it’s where the majority of patients and even some non-specialist doctors get it wrong.
Dietary calcium prevents kidney stones. It does not cause them.
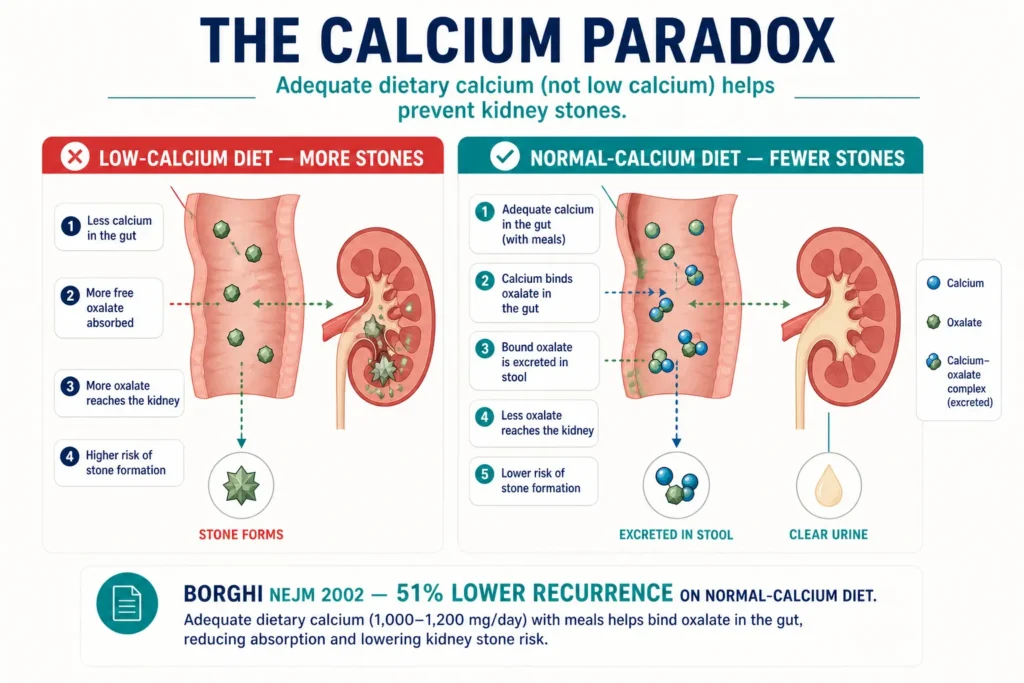
The landmark study that changed this understanding was a randomized controlled trial published in the New England Journal of Medicine by Borghi et al. in 2002. Men with recurrent calcium oxalate stones were randomized to either a low-calcium diet or a normal-calcium, low-sodium, low-animal-protein diet. The normal-calcium group had a 51% lower recurrence rate [2]. This was a paradigm-shifting finding.
The mechanism is straightforward: when you eat calcium-rich foods alongside oxalate-containing foods, the calcium binds to oxalate in your gut, forming an insoluble complex that is excreted in stool — not absorbed into your blood and filtered through your kidneys. Less oxalate reaches your kidneys, fewer stones form.
When you cut calcium from your diet, you absorb MORE oxalate from food, which reaches your kidneys in higher concentrations and crystallizes with whatever calcium is already in your urine. The result: more stones, not fewer.
The clinical recommendation
- Target: 1,000–1,200 mg of dietary calcium per day (equivalent to 3 servings of dairy).
- Source: Food, not supplements. Calcium supplements — especially when taken between meals — have been associated with increased stone risk because they don’t encounter dietary oxalate in the gut [6].
- Timing: Spread calcium intake across meals, especially meals containing high-oxalate foods. Having yogurt with a spinach salad is protective. Having the spinach alone is not.
Good calcium sources (per serving)
- Milk — 250 ml (8 fl oz): 300 mg calcium
- Yogurt — 200 g (about 7 oz): 280 mg
- Cheddar cheese — 40 g (about 1.4 oz): 290 mg
- Sardines with bones — 100 g (about 3.5 oz): 380 mg
- Fortified plant milks (almond, soy, oat) — 240–300 mg per cup (check the label)
- Calcium-set tofu — 100 g (about 3.5 oz): 350 mg
If you are lactose intolerant, yogurt is often better tolerated than milk (fermentation reduces lactose content), and lactose-free milk products provide the same calcium benefit.
Step 4: The Kidney Stone Diet — Oxalate Restriction Done Right

Oxalate restriction is probably the most over-emphasized aspect of stone prevention online. You’ll find exhaustive lists of 50–100 foods ranked by oxalate content, which are impractical and often lead patients to develop an unhealthy fear of vegetables.
Here’s the clinical reality: only a handful of extremely high-oxalate foods contribute meaningfully to urinary oxalate levels. Moderate-oxalate foods, eaten in normal portions with adequate calcium, are generally fine.
The “Definitely Restrict” list (very high oxalate — avoid or minimize)
- Spinach — the single highest dietary oxalate source. 100 g (about 3.5 oz) of cooked spinach contains 750–800 mg of oxalate. This is the one food I tell every calcium oxalate stone former to eliminate or drastically reduce. Use kale, lettuce, or bok choy instead.
- Rhubarb — extremely high oxalate, rarely eaten in large quantities but problematic when it is.
- Almonds and cashews — the highest-oxalate nuts. Switch to walnuts, pecans, or macadamias which are much lower.
- Beets (beetroot) — high oxalate in both raw and cooked forms.
- Dark chocolate and cocoa powder — significant oxalate content. Milk chocolate is lower but still moderate.
- Sweet potatoes — surprisingly high. Regular white potatoes are a much better choice.
- Star fruit — extremely high oxalate, also nephrotoxic in patients with kidney disease.
- Soy products (soy flour, soy protein isolate) — concentrated soy is very high; whole edamame is moderate.
The “Don’t Worry About It” list (moderate oxalate — fine in normal portions)
- Broccoli, cauliflower, cabbage — low oxalate, eat freely.
- Carrots, peppers, cucumbers — low to moderate, perfectly safe.
- Tomatoes — commonly blamed but actually low-moderate oxalate. Safe in normal amounts.
- Berries (strawberries, blueberries) — moderate but portion sizes are small enough to be insignificant.
- Rice, pasta, bread — low oxalate staples.
- Most fruits (apples, bananas, grapes, melon, peaches) — low oxalate.
- Chicken, fish, eggs — essentially zero oxalate.
The practical rule: avoid the top 8 high-oxalate foods, eat everything else normally, and always include calcium with meals. This approach is sustainable, evidence-based, and doesn’t turn eating into a source of anxiety. If you want a complete searchable A–Z reference, I keep an updated oxalate food list on the site.
🧮 Try the Tool: Searchable Oxalate Food List (A–Z)Step 5: Slash Your Sodium (This One Surprises Everyone)
Most patients are surprised when I tell them that salt intake directly affects kidney stone risk. The mechanism is well-established: for every 100 mmol of sodium excreted by the kidneys, approximately 40 mg of calcium is pulled along with it [3]. High-sodium diets literally push calcium into your urine, providing more substrate for stone formation.
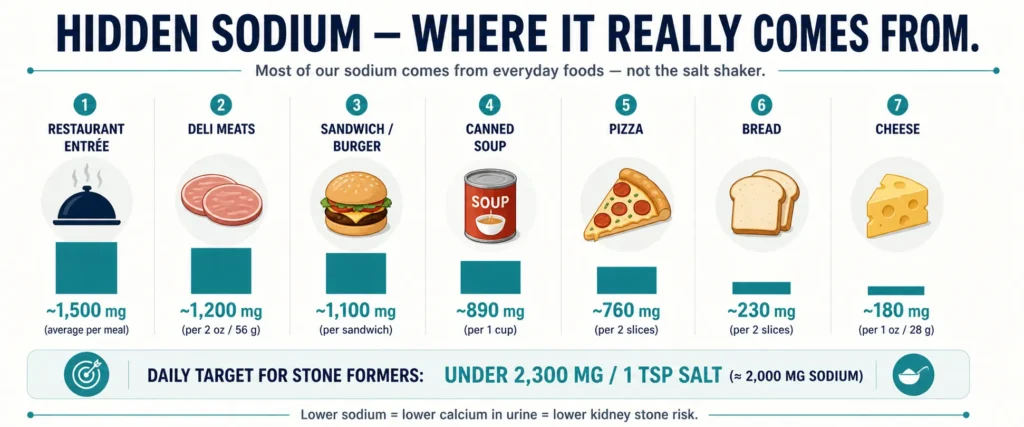
The guideline recommendation for stone formers is under 2,300 mg of sodium per day (about 1 teaspoon of table salt), with an ideal target below 1,500 mg (about ¾ teaspoon) [7]. For context, the average American diet contains 3,400–4,000 mg daily, and South Asian and Middle Eastern diets often exceed this.
The biggest hidden sodium sources
- Processed and packaged foods — chips, ready meals, canned soups, instant noodles. A single bowl of canned chicken noodle soup can hit 890 mg.
- Restaurant and takeout food — typically 2–3× the sodium of home-cooked equivalents. A Subway footlong, Chipotle bowl, or Panera sandwich often clears 1,500 mg in one meal.
- Bread — a surprisingly major contributor because of the quantity consumed daily. Two slices of standard sandwich bread is around 230 mg.
- Cheese — particularly processed cheese, feta, halloumi, and many South Asian paneers cured with salt.
- Sauces and condiments — soy sauce, ketchup, pickles, chutneys, achaar.
- Cured meats — ham, salami, bacon, sausages, deli turkey. Oscar Mayer-style packaged deli meats are among the highest-density sodium sources in the American grocery aisle.
Reducing sodium isn’t about never adding salt to food. It’s about being aware of how much hidden sodium you’re consuming from processed and restaurant food. Cooking at home with fresh ingredients and seasoning with herbs, spices, lemon, and garlic instead of salt makes a substantial difference.
Step 6: Animal Protein — The Moderation Message
High intake of animal protein — red meat, poultry, fish, and eggs — affects stone risk through three mechanisms simultaneously:
- Increases urinary uric acid — promoting both uric acid stones and acting as a nidus for calcium oxalate crystallization.
- Decreases urinary citrate — citrate is your kidneys’ natural stone inhibitor; high protein diets suppress it.
- Generates an acid load — lowers urine pH, favoring uric acid stone formation.
The Borghi trial that demonstrated the benefit of normal calcium also used protein restriction as part of the intervention — limiting animal protein to 52 g/day (about 1.8 oz) [2]. You don’t need to become vegetarian, but limiting red meat and organ meats to 2–3 servings per week and keeping total animal protein to roughly 0.8–1.0 g/kg body weight per day is a reasonable clinical target.
Plant protein (lentils, chickpeas, beans) does not carry the same risk and can replace animal protein freely. Fish is generally preferable to red meat, though shellfish and oily fish are higher in purines and should be moderated in uric acid stone formers.
Step 7: Citrate — Your Natural Stone Inhibitor
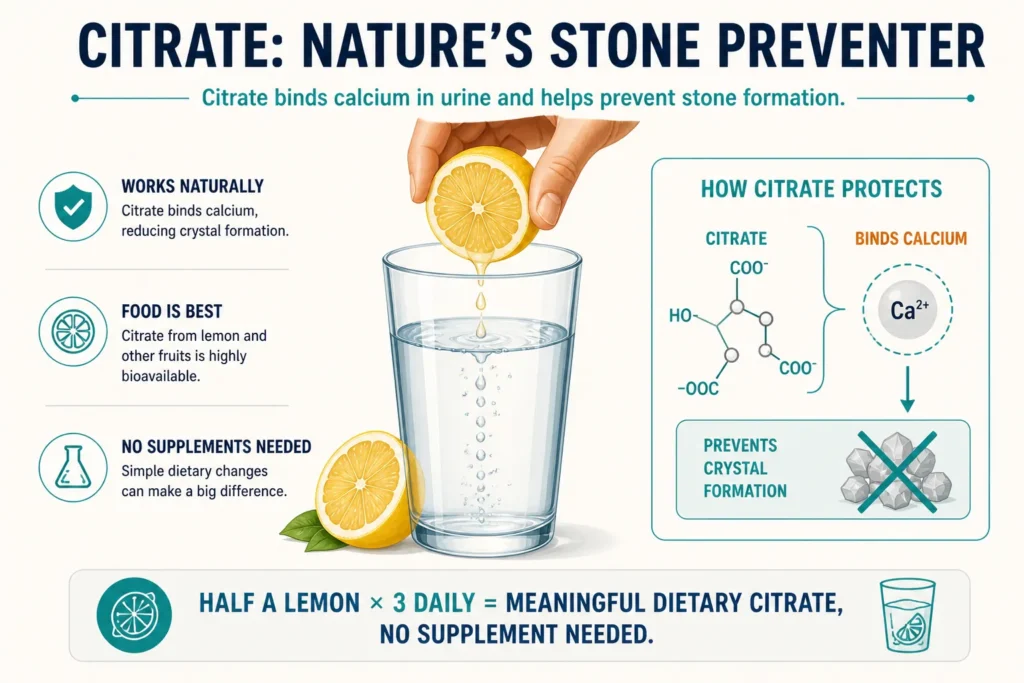
Citrate is one of the most important substances in your urine for preventing stones. It works by binding to calcium in the urine (preventing calcium oxalate crystal formation) and by directly inhibiting crystal growth and aggregation. Low urinary citrate (hypocitraturia) is found in 20–60% of stone formers [8].
Dietary citrate sources
- Lemons and limes — the highest citrate-to-calorie ratio. Half a lemon squeezed into water, 2–3 times daily, is the simplest dietary intervention I prescribe.
- Oranges and orange juice — high citrate but also high sugar and calories. One glass daily is reasonable, but lemon water is preferable for most patients.
- Grapefruit — a good citrate source but interacts with multiple medications (statins, calcium channel blockers). Check with your doctor first.
When diet isn’t enough: potassium citrate supplements
For patients with documented hypocitraturia on 24-hour urine analysis (urinary citrate below 320 mg/day), I prescribe potassium citrate supplements — typically 30–60 mEq/day in divided doses. This is the most evidence-based pharmacological intervention for calcium stone prevention and also alkalizes urine, which helps prevent uric acid stones [9].
Sodium citrate should be avoided — it provides citrate but the sodium load counteracts the benefit by increasing calcium excretion.
Download Your Free Clinical Action Plan
Enter your email below to download Dr. Khalid’s complete 7-Day Kidney Stone Prevention Meal Plan as a free, printable PDF.
Special Protocol: Uric Acid Stone Prevention
Uric acid stones require a fundamentally different dietary approach. The primary driver is acidic urine (pH below 5.5), not oxalate. The strategy centers on alkalizing urine and reducing purine intake.
- Alkalize urine: Target urine pH 6.0–7.0. Potassium citrate is the mainstay. Dietary alkalization with increased fruits and vegetables helps.
- Reduce purine-rich foods: Organ meats (liver, kidney), game meats, shellfish, anchovies, sardines, and beer are the worst offenders.
- Limit fructose: High-fructose corn syrup (in soft drinks and processed foods) increases uric acid production. This is an under-recognized contributor.
- Moderate alcohol: Beer is particularly problematic (high in purines AND dehydrating). Wine and spirits have less purine content but still dehydrate.
- Hydration: Even more important than for calcium stones — uric acid solubility is highly volume-dependent.
The unique advantage of uric acid stones is that they can sometimes be dissolved with aggressive urine alkalization — something no other common stone type allows. If you have a uric acid stone in your kidney, a trial of potassium citrate with urine pH monitoring (target 6.5–7.0) for 2–3 months may dissolve it completely without surgery.
→ Related Read: Types of Kidney Stones — Which One Do You Have?My 5-Point Daily Kidney Stone Diet Protocol
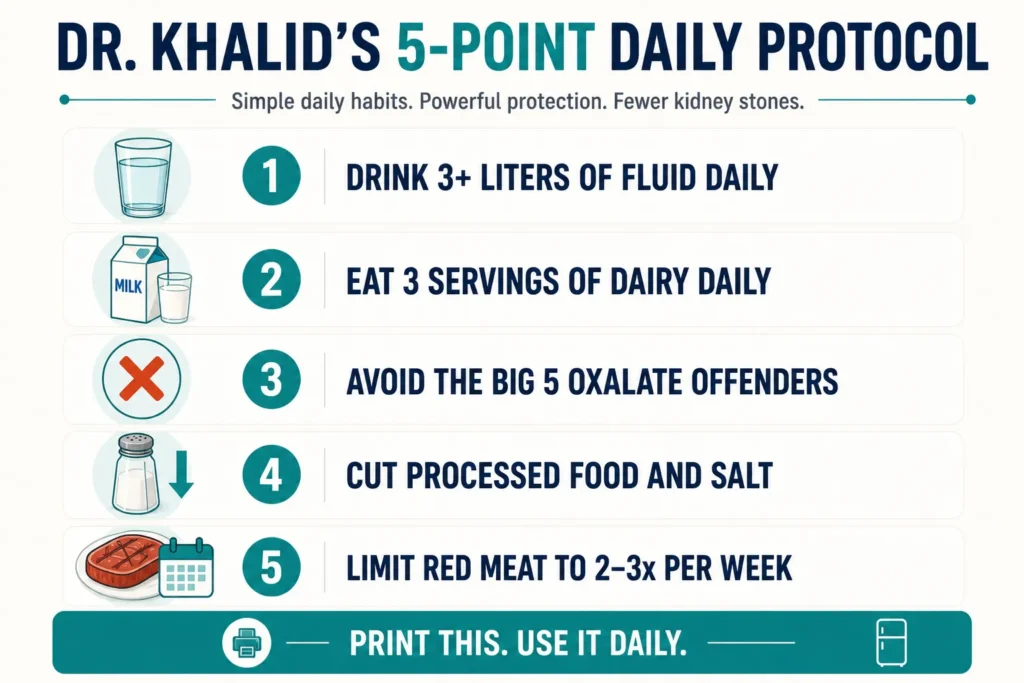
When patients ask me to simplify everything into an actionable daily kidney stone diet, this is what I give them. It’s printed and handed out in my clinic:
- Drink 3+ liters of fluid daily (about 100+ fl oz). Water primarily. Add half a lemon to 2–3 glasses. Drink a full glass before bed and if you wake at night. Target: pale yellow urine all day.
- Eat 3 servings of dairy daily. Milk, yogurt, or cheese — with meals, not between meals. This is your oxalate defense system.
- Avoid the Big 5 oxalate offenders: spinach, rhubarb, almonds, beets, dark chocolate. Everything else in normal portions is fine.
- Cut processed food and excess salt. Cook at home, season with lemon and spices instead of salt. Target under 2,300 mg sodium/day (about 1 teaspoon).
- Limit red meat to 2–3 times per week. Replace with fish, chicken, eggs, or plant protein. No organ meats.
That’s it. Five rules. If a patient follows these consistently, the likelihood of recurrence drops dramatically. The patients who struggle are usually the ones who try to follow overly complex oxalate spreadsheets and give up within a month.
→ Related Read: How to Pass a Kidney Stone Fast — What I Tell My Patients💡 In My Practice
The single biggest barrier to dietary compliance in my practice is the calcium misconception. I’d estimate that 60–70% of patients who come to me with recurrent calcium stones have already started restricting dairy — either on their own or on advice from a non-specialist doctor. The first thing I do is sit them down, explain the Borghi trial in plain language, and tell them to start eating yogurt again. The relief on their faces is visible. One patient — a 52-year-old man with three episodes of obstructing ureteric stones over four years — had been drinking only black coffee and avoiding milk for two years on the advice of a relative. Within six months of restoring normal dairy intake and the rest of the 5-point protocol, his 24-hour urinary oxalate dropped from 65 mg/day to 38 mg/day, and he has been stone-free for over two years.
The second most common issue in my patient population is black tea consumption. In our region, patients routinely drink 6–8 cups of strong black tea daily — often with the leaves boiled hard, which extracts maximum oxalate. This is an enormous oxalate load that many don’t even consider a dietary factor because tea is so culturally embedded. I have patients switch to green tea or reduce to 1–2 cups, and I’ve watched recurrent stone formers stop forming new stones over 12–18 months on imaging.
The third pattern: patients want a complicated answer. They want a 50-food spreadsheet. They want supplements. They want a special bottled water. The 5-point protocol above is far more effective than any of that — because simplicity drives compliance. The patients who memorize those five rules and actually follow them almost never come back with another stone. The patients who chase complexity usually quit within four to six weeks and end up back in my clinic with recurrent disease.
Common Myths That Need to Die
Myth: “Drink cranberry juice to prevent stones”
Wrong target. Cranberry juice has some evidence for UTI prevention (debatable), but it actually increases urinary oxalate excretion and may raise stone risk [10]. It also provides unnecessary sugar and calories. Lemon water is superior in every way for stone prevention.
Myth: “Avoid all vegetables because of oxalate”
Dangerously wrong. Vegetables provide potassium, magnesium, and alkali — all protective against stones. Only spinach, rhubarb, and beets need serious restriction. The rest of the vegetable kingdom is your ally, not your enemy. A plant-rich diet actually reduces stone risk [11].
Myth: “Beer flushes out kidney stones”
A persistent myth with zero evidence. Beer increases urine volume temporarily but causes net dehydration through alcohol’s diuretic effect. It also raises uric acid (purines in beer), increases urinary calcium, and lowers citrate. Beer consumption is associated with increased stone risk, not decreased.
Myth: “Vitamin C supplements are fine for stone formers”
Caution needed. Vitamin C (ascorbic acid) is metabolized to oxalate. Doses above 1,000 mg/day have been associated with increased kidney stone risk in men [12]. Getting vitamin C from food (oranges, peppers, kiwi) is safe and preferred. Mega-dose supplements should be avoided in stone formers.
Myth: “Tomatoes cause kidney stones”
Almost universally untrue. Tomato oxalate content is moderate (about 50 mg per medium tomato) and a lifetime of normal tomato consumption — including in cooking, sauces, and salads — has not been linked to stone formation in any major dietary study. This myth is especially entrenched in South Asian medical culture, where patients are often told to stop eating tomatoes after their first stone. There is no evidence to support that advice.
→ Related Read: Foods That Cause Kidney Stones — Oxalate, Sodium & the Truth⚠️ When to See a Urologist — Urgently
- Recurrent stones (2+ episodes) — you need a 24-hour urine metabolic evaluation, not just generic diet advice. This identifies your specific metabolic abnormality (hypercalciuria, hyperoxaluria, hypocitraturia, hyperuricosuria) and allows targeted treatment.
- Family history of kidney stones — you’re at 2.5× higher risk and should adopt preventive measures proactively.
- First stone under age 25 — may indicate an underlying metabolic condition (cystinuria, primary hyperoxaluria, hyperparathyroidism) requiring specialist workup.
- Stones despite good hydration and diet — pharmacological prevention (thiazide diuretics, potassium citrate, allopurinol) may be needed alongside dietary measures.
- Stones with chronic kidney disease — dietary modifications need to be balanced with CKD dietary restrictions, which sometimes conflict (e.g., potassium restriction in CKD vs. potassium citrate for stones).
Frequently Asked Questions
Can I eat tomatoes if I have kidney stones?
Yes. Tomatoes are one of the most commonly — and incorrectly — blamed foods for kidney stones. Their oxalate content is moderate (about 50 mg per medium tomato) and nowhere near the levels found in spinach or almonds. Normal consumption of tomatoes, including in cooking, is perfectly safe for most stone formers. This myth persists strongly in South Asian medical culture, but it is not supported by evidence. For a fuller list of which foods actually matter, see my guide to foods that cause kidney stones.
Should I stop drinking milk if I have calcium kidney stones?
The opposite. You should make sure you’re getting adequate dairy — about 3 servings per day. The calcium in milk binds oxalate in your gut and prevents it from reaching your kidneys. Cutting milk increases your stone risk. This is one of the most evidence-based recommendations in all of stone prevention, established by the Borghi NEJM trial in 2002. To estimate your own 5-year stone risk, try my Kidney Stone Risk Profiler.
How much water is too much for kidney stone prevention?
There is no benefit to drinking beyond 3.5–4 liters daily for stone prevention. Excessive water intake (over 5 liters/day) can dilute electrolytes dangerously, particularly sodium, causing hyponatremia. The target is 2.5 liters of urine output — not maximum possible water consumption. Pale yellow urine is the goal; completely clear urine means you can ease off slightly. For a personalized fluid target, use my Hydration Calculator.
Is a vegetarian diet better for preventing kidney stones?
Generally yes, with caveats. Vegetarian and plant-rich diets are associated with lower stone risk because they reduce animal protein load, increase dietary alkali, and tend to be lower in sodium. However, vegetarians who rely heavily on spinach, nuts, and soy (all high-oxalate) can still form stones. The principle is not eliminating meat entirely but rather balancing protein sources and managing oxalate intake regardless of dietary pattern. The oxalate food list applies equally to vegetarians and omnivores.
Do I need to follow this kidney stone diet forever?
If you’ve had one stone, yes — these are lifelong habits, not a short-term diet. The recurrence rate without prevention is roughly 50% in 5 years and 80% in 10 years. With consistent dietary prevention, those numbers drop to 10–15%. The good news is that once the 5-point protocol becomes habit (which takes about 3–4 weeks), it doesn’t feel like a “diet” — it’s just how you eat. If you want a complete picture of what you’re up against, read my complete kidney stones guide.
📚 References
- Moe OW. Kidney stones: pathophysiology and medical management. Lancet. 2006;367(9507):333–344. PubMed
- Borghi L, Schianchi T, Meschi T, et al. Comparison of two diets for the prevention of recurrent stones in idiopathic hypercalciuria. N Engl J Med. 2002;346(2):77–84. PubMed
- Nouvenne A, Meschi T, Prati B, et al. Effects of a low-salt diet on idiopathic hypercalciuria in calcium-oxalate stone formers: a 3-month randomized controlled trial. Am J Clin Nutr. 2010;91(3):565–570. PubMed
- Borghi L, Meschi T, Amato F, et al. Urinary volume, water and recurrences in idiopathic calcium nephrolithiasis: a 5-year randomized prospective study. J Urol. 1996;155(3):839–843. PubMed
- Ferraro PM, Taylor EN, Gambaro G, Curhan GC. Soda and other beverages and the risk of kidney stones. Clin J Am Soc Nephrol. 2013;8(8):1389–1395. PubMed
- Curhan GC, Willett WC, Speizer FE, Spiegelman D, Stampfer MJ. Comparison of dietary calcium with supplemental calcium and other nutrients as factors affecting the risk for kidney stones in women. Ann Intern Med. 1997;126(7):497–504. PubMed
- Pearle MS, Goldfarb DS, Assimos DG, et al. Medical management of kidney stones: AUA guideline. J Urol. 2014;192(2):316–324. AUA Guidelines
- Zuckerman JM, Assimos DG. Hypocitraturia: pathophysiology and medical management. Rev Urol. 2009;11(3):134–144. PubMed
- Pak CY, Sakhaee K, Fuller C. Successful management of uric acid nephrolithiasis with potassium citrate. Kidney Int. 1986;30(3):422–428. PubMed
- Gettman MT, Ogan K, Brinkley LJ, Adams-Huet B, Pak CY, Pearle MS. Effect of cranberry juice consumption on urinary stone risk factors. J Urol. 2005;174(2):590–594. PubMed
- Turney BW, Appleby PN, Reynard JM, Noble JG, Key TJ, Allen NE. Diet and risk of kidney stones in the Oxford cohort of the European Prospective Investigation into Cancer and Nutrition (EPIC). Eur J Epidemiol. 2014;29(5):363–369. PubMed
- Thomas LD, Elinder CG, Tiselius HG, Wolk A, Akesson A. Ascorbic acid supplements and kidney stone incidence among men: a prospective study. JAMA Intern Med. 2013;173(5):386–388. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.

Supplements for Kidney Stone Prevention: What Works
Foods That Cause Kidney Stones: A Urologist’s Honest List
Hydration and Kidney Health: The Truth About Water Intake
Hydration and kidney health are linked far more tightly than most patients realize — and far more strangely...
Kidney Stones: Complete Guide from a Urologist | Causes, Symptoms & Treatment
