Kidney Stones: Complete Guide from a Urologist | Causes, Symptoms & Treatment
When you are in the agonizing grip of a kidney stone, your only focus is just getting it out. The harsh reality is that passing the stone is only half the battle; without a specific prevention plan, you have a 50% chance of doing it all over again. As a urologist who surgically removes these every week, here is my unfiltered guide to clearing your current stone—and exactly how to stop the next one.

Kidney stones are one of the most common — and most painful — conditions I treat as a urologist. If you’ve landed on this page, you’re probably either dealing with a stone right now or trying to make sure you never deal with one again. Either way, I’ll give you the same information I give my patients in clinic: clear, honest, and based on what the evidence actually shows.
Roughly 1 in 10 people will develop a kidney stone during their lifetime, and recurrence rates are high — up to 50% within five years without preventive measures [1]. The good news is that most stones can be managed effectively, and many can be prevented entirely with the right approach.
As a urologist who performs ureteroscopy (URS), PCNL, and RIRS on a regular basis, I want to give you a kidney stones symptoms treatment guide that goes beyond generic symptom lists — one that explains what’s actually happening inside your urinary tract, what the treatment options involve, and how to stop this from happening again. For the full pillar overview, see our complete Kidney Stones Hub.
📋 Key Takeaways
- Most kidney stones are calcium oxalate (70–80%) and are strongly influenced by diet and hydration.
- Small stones (under 5–6 mm / about 1/4 inch) usually pass on their own with fluids and pain management; larger stones often need intervention.
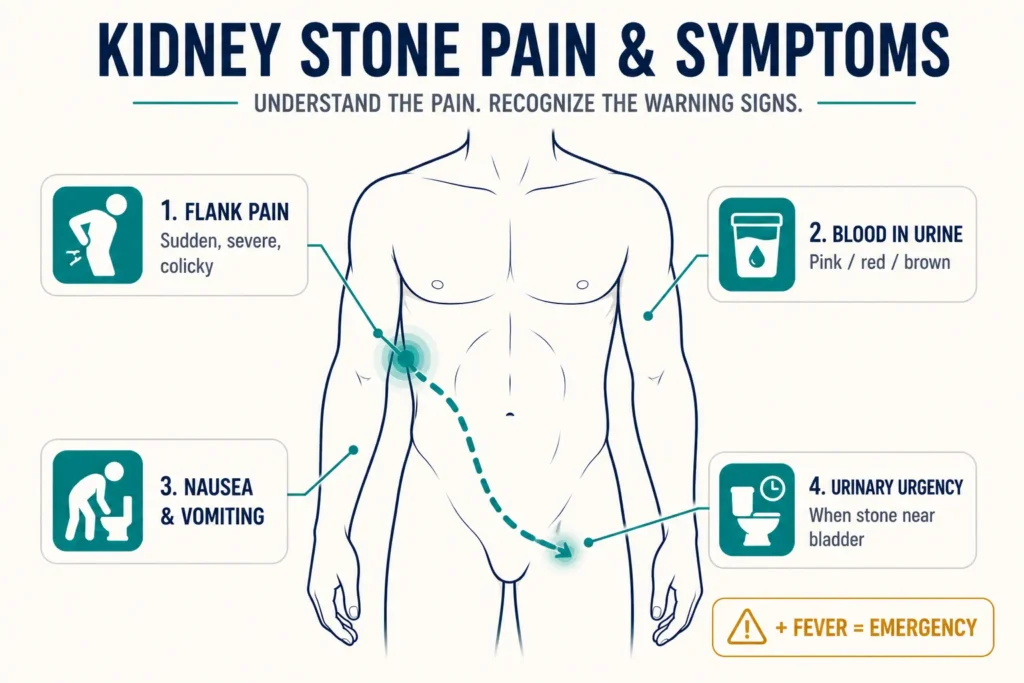
- Severe flank pain radiating to the groin, blood in urine, and nausea or vomiting are the classic triad of symptoms.
- Modern treatments — URS, PCNL, and RIRS — are minimally invasive, with success rates of 85–95%.
- Fever + flank pain = urological emergency. This combination means an infected obstructed kidney and requires immediate emergency room attendance.
- Prevention is largely about hydration, dietary adjustments, and understanding your stone type through chemical analysis.
What Are Kidney Stones?
Kidney stones — medically termed nephrolithiasis or urolithiasis (literally “stones in the urinary system”) — are hard mineral deposits that form inside your kidneys when urine becomes so concentrated that dissolved minerals begin to crystallize and clump together. They range from a grain of sand to a golf ball, though most that cause symptoms are somewhere between 2 mm and 15 mm (about 1/12 inch to 5/8 inch).
Stones form when there’s an imbalance between the substances that promote crystal formation (calcium, oxalate, uric acid, cystine) and those that inhibit it (citrate, magnesium). When this balance tips — through dehydration, diet, metabolic abnormalities, or genetics — crystals nucleate, grow, and eventually become large enough to cause obstruction or pain.
The pain from kidney stones — renal colic — is frequently described by patients as the worst pain they’ve ever experienced, sometimes compared to or exceeding childbirth in severity. This pain occurs when a stone migrates from the kidney into the ureter (the narrow tube connecting kidney to bladder) and causes obstruction and muscle spasm.
→ Related Read: How to Pass a Kidney Stone Fast — What I Tell My PatientsTypes of Kidney Stones: Why Your Stone Type Matters
Not all kidney stones are the same, and knowing your stone type matters for prevention — our breakdown of the five main stone types and how to tell which one you form goes deeper than this overview. The type determines your dietary strategy, medical management, and risk of recurrence. If your stone was not sent for chemical composition analysis after treatment, ask your urologist about a 24-hour urine metabolic evaluation — this can identify your risk profile even without the stone itself [2].
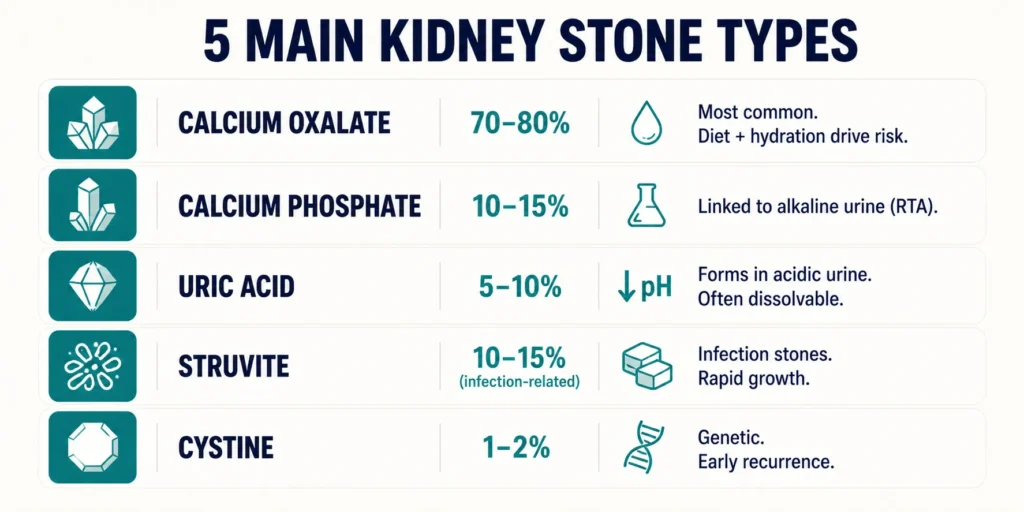
Calcium Oxalate Stones (70–80% of cases)
By far the most common type. They form when calcium combines with oxalate in the urine. Despite the name, calcium restriction is not the answer — adequate dietary calcium actually reduces stone risk by binding oxalate in the gut before it reaches the kidneys. High-oxalate foods that contribute to these stones include spinach, rhubarb, beets, almonds, dark chocolate, and sweet potatoes.
Calcium Phosphate Stones (10–15%)
These are often associated with renal tubular acidosis or conditions that raise urine pH to abnormally alkaline levels. They tend to be harder to prevent and may recur more aggressively than calcium oxalate stones.
Uric Acid Stones (5–10%)
Unique because they form in acidic urine (pH below 5.5) and are the only common stone type that can potentially be dissolved with medical therapy. They’re more common in patients with gout, diabetes, obesity, and chronic diarrhea [3]. Potassium citrate to alkalinize urine is the cornerstone of both treatment and prevention.
Struvite Stones (Infection Stones)
Caused by urinary tract infections with urease-producing bacteria (most commonly Proteus species). They can grow rapidly into large “staghorn” calculi that fill the entire renal collecting system. More common in women. They require both complete stone removal and treatment of the underlying infection — leaving fragments behind means guaranteed recurrence.
Cystine Stones (1–2%)
These occur in patients with cystinuria, a genetic condition causing excessive cystine excretion in urine. They tend to present at a young age and recur frequently. Management requires aggressive hydration, urine alkalinization, and sometimes medications like tiopronin or D-penicillamine.
→ Related Read: The Kidney Stone Diet — My Clinical Protocol for PreventionSymptoms: How Do You Know You Have a Kidney Stone?
The classic presentation of a kidney stone is unmistakable — but not all stones announce themselves dramatically. Here’s what to watch for.
Renal Colic — The Hallmark
Renal colic is severe, colicky (comes in waves) pain that typically starts in the flank — the side of the back below the ribs — and radiates downward toward the groin, lower abdomen, or genitalia. It follows the path of the ureter as the stone travels. The pain is often so severe it causes vomiting and prevents the patient from finding a comfortable position — unlike back muscle pain, where lying still provides some relief.
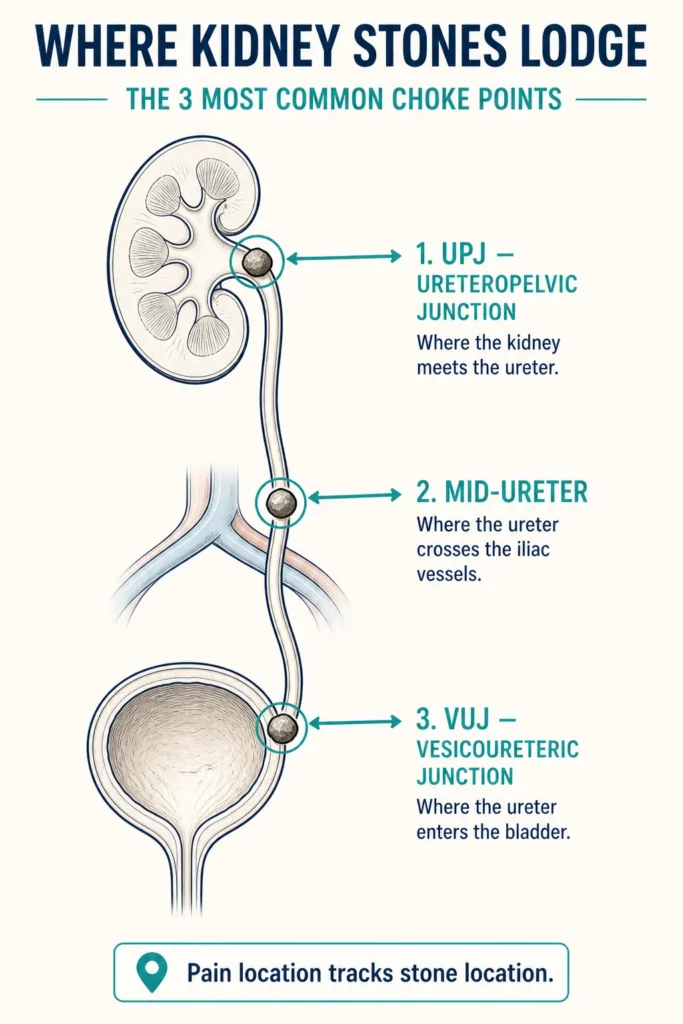
The location of pain helps identify where the stone is lodged: flank pain suggests the upper ureter or kidney; lower abdominal pain points to the mid-ureter; urinary urgency, frequency, and perineal pain indicate the stone is near the bladder (vesicoureteric junction, or VUJ).
Other Common Symptoms
- Hematuria (blood in urine) — present in about 85% of acute stone episodes. Urine may appear pink, red, or brown, or blood may only be detectable on urinalysis.
- Nausea and vomiting — caused by shared nerve pathways between the kidney and the gastrointestinal tract.
- Dysuria (painful urination) — especially when the stone is near the bladder.
- Urinary urgency and frequency — particularly with distal ureteric stones near the VUJ.
- Fever and chills — this is a red flag indicating infected obstruction (obstructive pyelonephritis), which is a urological emergency requiring immediate drainage.
Silent Stones
Not all stones cause symptoms. Some sit in the kidney for years without causing pain — discovered incidentally on imaging done for other reasons. Whether to treat them depends on size, location, and growth pattern over serial imaging. A stone sitting quietly in the kidney is not always harmless; it can still cause slow, silent damage to renal function if it causes partial obstruction.
Diagnosis: What Tests Will Your Doctor Order?
Initial Assessment
When a patient presents with suspected renal colic, the workup typically includes a urinalysis (looking for hematuria, infection, and urine pH), blood tests (serum creatinine for kidney function, full blood count, calcium, uric acid, and electrolytes), and a urine culture if infection is suspected.
Imaging
Non-contrast CT KUB (kidneys, ureters, bladder) is the gold standard for diagnosing kidney stones [4][5]. It has a sensitivity exceeding 95% and can detect virtually all stone types, determine exact size and location, identify the degree of obstruction (hydronephrosis), and guide treatment planning. It is the first investigation I order in any adult with suspected renal colic.
Ultrasound is the first-line tool in pregnant women and children (to avoid radiation exposure). It’s effective at detecting hydronephrosis and renal stones but less reliable for ureteric stones, particularly in the mid-ureter. X-ray KUB can identify radio-opaque calcium-containing stones but misses uric acid and cystine stones, which are radiolucent (invisible on plain X-ray).
Download Your Free Clinical Action Plan
Enter your email below to download Dr. Khalid’s complete 7-Day Kidney Stone Prevention Meal Plan as a free, printable PDF.
Treatment: How Are Kidney Stones Managed?
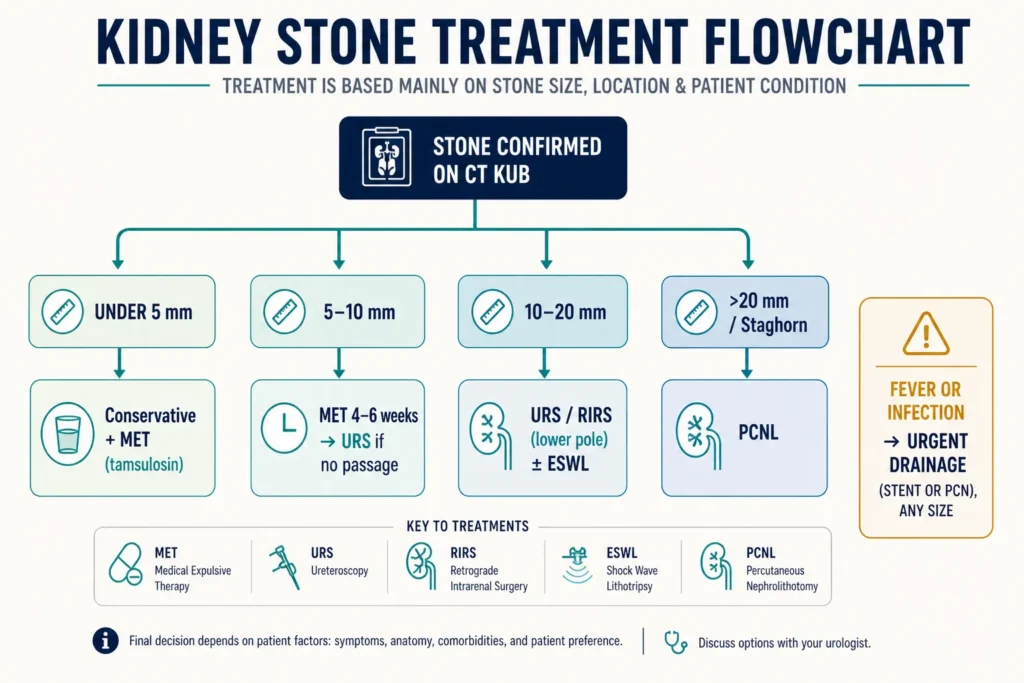
Treatment depends on three factors: stone size, stone location, and whether there are complications — specifically infection, complete obstruction, or deteriorating kidney function.
→ URS vs PCNL vs RIRS: how I decide which stone surgery fits which patientConservative Management — Watchful Waiting
For stones smaller than 5–6 mm (about 1/4 inch) in the ureter, spontaneous passage is likely. Approximately 68% of stones under 5 mm and 47% of stones 5–10 mm will pass on their own [6]. The approach includes aggressive hydration (2.5–3 liters per day, about 85–100 fl oz / 10–13 cups), NSAIDs (diclofenac or ibuprofen) as first-line analgesics — they work better than opioids for renal colic because they reduce ureteric spasm and inflammation — and medical expulsive therapy (MET) with alpha-blockers like tamsulosin (0.4 mg daily), which relax the smooth muscle of the distal ureter and increase the rate and speed of stone passage for stones 5–10 mm [7].
One critical and often overlooked step: patients should strain their urine to catch the stone for laboratory analysis. Knowing your stone composition changes everything about prevention. To estimate the likelihood your specific stone will pass on its own, use our Kidney Stone Passability Predictor, which factors in stone size, location, and patient characteristics.
Ureteroscopy (URS)
A thin scope is passed through the urethra, bladder, and into the ureter to directly visualize the stone. It is then fragmented using a holmium or thulium fiber laser, and fragments are extracted with a basket. URS is the most common surgical procedure for ureteric stones and lower pole renal stones under 15–20 mm (about 5/8 to 3/4 inch). Success rates exceed 90–95% for ureteric stones. It is typically a day-case procedure with a low complication rate. A ureteral stent (JJ stent) may be placed temporarily to prevent swelling from obstructing the ureter post-procedure.
Percutaneous Nephrolithotomy (PCNL)
For large renal stones (generally over 20 mm / about 3/4 inch) or staghorn calculi, PCNL is the procedure of choice. A small puncture is made through the back directly into the kidney, and a nephroscope is used to fragment and remove the stone percutaneously. This is a more involved procedure requiring general anesthesia and typically 2–3 days of hospitalization. Success rates for stones over 20 mm reach 85–95%. PCNL has largely replaced open surgery for large and complex stones.
Retrograde Intrarenal Surgery (RIRS)
RIRS uses a flexible ureteroscope to access stones within the kidney itself — valuable for stones 10–20 mm (about 3/8 to 3/4 inch), particularly in patients where PCNL carries higher risk due to bleeding disorders, obesity, or anatomical variations. It bridges the gap between URS and PCNL and has become more frequently used as flexible scope and laser technology has advanced.
Extracorporeal Shock Wave Lithotripsy (ESWL)
A non-invasive treatment that uses focused shock waves from outside the body to fragment stones into smaller pieces that pass naturally. Best suited for renal stones under 20 mm that are not in the lower pole, and in patients with soft stone compositions (calcium oxalate dihydrate, uric acid). Less effective for hard stones (calcium oxalate monohydrate, cystine) and in obese patients. Success rates range from 60–90% depending on stone size, location, and composition — and multiple sessions may be required.
Open Surgery
Required in fewer than 1–2% of cases today, thanks to advances in endourology. Reserved for extremely complex anatomical situations, failed minimally invasive procedures, or cases where concurrent anatomical reconstruction is needed (for example, pyeloplasty for ureteropelvic junction obstruction with concurrent stone).
Prevention: How to Stop Kidney Stones from Coming Back
Prevention matters more than treatment, because recurrence rates are high — up to 50% within 5–10 years without targeted measures [1]. If you want a sense of your own odds, our 5-year stone recurrence risk profiler weighs your stone history and metabolic factors. The starting point is always knowing your stone type.
Universal Preventive Measures (for all stone types)
- Hydration is the single most impactful intervention — aim for at least 2.5 liters of urine output daily (about 85 fl oz / 10 cups). Target pale yellow urine throughout the day. This alone reduces recurrence by 40–50%.
- Dietary sodium restriction — high salt intake increases urinary calcium excretion. Target under 2,300 mg sodium per day (about 1 teaspoon of salt); under 1,500 mg (about 3/4 teaspoon) is ideal.
- Adequate dietary calcium — low calcium diets increase stone risk by increasing gut absorption of oxalate. Target 1,000–1,200 mg per day from food sources — dairy, not supplements (about three servings of milk, yogurt, or cheese) [8].
- Limit animal protein — high red meat intake increases uric acid, decreases urinary citrate, and lowers urine pH.
- Increase citrus intake — lemon juice and orange juice are natural dietary sources of citrate, which inhibits crystal formation.
Stone-Type-Specific Prevention
For calcium oxalate stones, reduce the highest-oxalate foods (spinach, rhubarb, almonds, dark chocolate, beets, sweet potatoes). Maintain adequate calcium intake. Consider potassium citrate supplementation if urinary citrate is documented to be low on a 24-hour urine test.
For uric acid stones, alkalinize urine with potassium citrate (target pH 6.0–7.0). Reduce purine-rich foods — organ meats, shellfish, beer. Allopurinol is indicated if serum uric acid is elevated. Uniquely, uric acid stones can dissolve with aggressive alkalinization — making early medical management particularly important.
For cystine stones, very high fluid intake (over 3 liters per day, about 100 fl oz / 13 cups) is essential, combined with urine alkalinization to pH above 7.0. Refractory cases require tiopronin or D-penicillamine.
For struvite stones, complete surgical removal is the priority — dietary modification has minimal effect. Residual stone fragments harbor bacteria and lead to near-certain recurrence.
→ Related Read: Hydration & Kidney Health — The Water Myth vs. What Science Shows💡 In My Practice
Kidney stones are one of the conditions I see most frequently in both emergency and outpatient settings. The biggest clinical error I encounter is patients restricting calcium after getting a calcium stone — this actually worsens recurrence by increasing oxalate absorption. I correct this at every first consultation. The second most common mistake is not sending the stone for chemical analysis after removal — without a stone type, prevention is guesswork dressed up as advice.
I also tell every patient that a single episode of renal colic should be a wake-up call about hydration and diet — not just something to treat and forget. The patients who take prevention seriously almost never return with a second stone. Those who don’t take it seriously almost always do.
⚠️ When to See a Doctor — Urgently
- Fever with flank pain — this combination means an infected obstructed kidney (obstructive pyelonephritis). Without emergency drainage (ureteral stenting or percutaneous nephrostomy), this can progress to urosepsis and become rapidly life-threatening.
- Complete inability to urinate (anuria) — may indicate bilateral ureteric obstruction or obstruction of a solitary functioning kidney, causing acute kidney injury that requires immediate intervention.
- Persistent vomiting preventing oral fluids and medication — requires IV analgesia, IV fluids, and emergency room assessment.
- Uncontrollable pain not responding to oral analgesics — needs emergency IV diclofenac or opioid analgesia and imaging.
- Known single kidney with stone symptoms — any obstruction threatens the only functioning kidney and is always an emergency.
Frequently Asked Questions
How long does it take to pass a kidney stone naturally?
For small stones under 5 mm (about 1/5 inch), most pass within 1–2 weeks with adequate hydration and pain management. Stones 5–8 mm may take 2–4 weeks. If a stone hasn’t passed within 4–6 weeks despite conservative management, intervention is typically recommended — both to relieve symptoms and to prevent progressive kidney damage from prolonged obstruction. Never wait beyond this window without urological assessment. Our guide to passing a kidney stone fast covers the practical steps that speed up natural passage.
Can kidney stones permanently damage my kidneys?
Yes. Prolonged complete obstruction can cause irreversible kidney damage within 2–4 weeks. Infected obstruction (stone plus fever) can cause rapid kidney destruction within days. Even partial, silent obstruction over months to years can gradually reduce kidney function. This is why follow-up imaging after a stone episode matters — not just to confirm it has passed, but to rule out residual obstruction or remaining stone fragments. See our hydration and kidney health guide for the single most effective preventive step.
Do kidney stones run in families?
There is a meaningful genetic component. If a first-degree relative (parent or sibling) has had kidney stones, your risk is approximately 2.5 times higher [9]. Certain conditions like cystinuria are directly inherited. However, shared dietary and lifestyle habits within families also play a significant role — which means family members often benefit from the same preventive advice. The kidney stone diet protocol is the same whether the underlying driver is genetic or dietary.
Is beer or cranberry juice useful for kidney stones?
Neither. Beer is not an effective treatment despite the popular myth. While it increases urine output temporarily, alcohol causes net dehydration overall, and beer contains purines that elevate uric acid production. Cranberry juice may reduce UTI risk in women but does not prevent or treat kidney stones — it can actually increase urinary oxalate excretion, which raises calcium oxalate stone risk. Lemon water is the superior choice on all fronts. More on fluid choices is in the hydration guide.
Should I take calcium supplements if I form kidney stones?
Dietary calcium from food is protective against stones. Calcium supplements — particularly when taken between meals without food — may increase stone risk [8] because they don’t encounter dietary oxalate in the gut. If you genuinely need supplemental calcium (for example, for osteoporosis), take it with meals so it can bind dietary oxalate. And wherever possible, prioritize food sources: dairy, fortified plant milks, sardines with bones. The kidney stone diet protocol walks through specific food targets.
What is the difference between URS and PCNL?
URS (ureteroscopy) approaches the stone by going up through the natural urinary passage — urethra, bladder, then into the ureter or kidney with a thin scope. It’s ideal for ureteric stones and smaller renal stones under 15–20 mm. PCNL (percutaneous nephrolithotomy) creates a direct puncture access through the back into the kidney — used for large or complex renal stones over 20 mm. PCNL is more invasive but handles larger stone volumes in a single procedure. Both are performed under general anesthesia. To see which procedure may suit your specific stone, our passability predictor tool gives a starting estimate.
📚 References
- Moe OW. Kidney stones: pathophysiology and medical management. Lancet. 2006;367(9507):333–344. PubMed
- Alelign T, Petros B. Kidney stone disease: an update on current concepts. Advances in Urology. 2018;2018:3068365. PubMed
- Sakhaee K. Epidemiology and clinical pathophysiology of uric acid kidney stones. Journal of Nephrology. 2014;27(3):241–245. PubMed
- Assimos D, Krambeck A, Miller NL, et al. Surgical Management of Stones: AUA/Endourology Society Guideline. American Urological Association. 2016 (amended 2023). AUA Guidelines
- Skolarikos A, Neisius A, Petřík A, et al. EAU Guidelines on Urolithiasis. European Association of Urology. 2024. EAU Guidelines
- Jendeberg J, Geijer H, Alshamari M, et al. Size matters: the width and location of a ureteral stone accurately predict the chance of spontaneous passage. European Radiology. 2017;27(11):4775–4785. PubMed
- Campschroer T, Zhu X, Vernooij RW, Lock MTWT. Alpha-blockers as medical expulsive therapy for ureteral stones. Cochrane Database of Systematic Reviews. 2018;4:CD008509. Cochrane / PubMed
- Curhan GC, Willett WC, Speizer FE, Spiegelman D, Stampfer MJ. Comparison of dietary calcium with supplemental calcium and other nutrients as factors affecting the risk for kidney stones in women. Annals of Internal Medicine. 1997;126(7):497–504. PubMed
- Goldfarb DS, Fischer ME, Keich Y, Goldberg J. A twin study of genetic and dietary influences on nephrolithiasis. Kidney International. 2005;67(3):1053–1061. PubMed
Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.